Dermatopathology Practice in Sub-Saharan Africa: Analysis of Skin Biopsies from a Dermatology Clinic in Nigeria
Abdullahi Muhammad Ahmad
1. Department of Pathology, Aminu Kano Teaching Hospital, Kano, Nigeria
Hassan Adam Murtala
2. Department of Epidemiology and Population Health, Kano Independent Research Center Trust (KIRCT), Kano
DOI: https://doi.org/10.55320/mjz.52.5.760
Keywords:Dermatopathology, Skin biopsies, Sub Saharan Africa
ABSTRACT
Background: Dermatopathology serves as a critical foundation for accurate diagnosis in dermatology clinics; however, it remains underdeveloped or absent in many pathology departments across Sub-Saharan Africa
Methods: A cross-sectional study was conducted on skin biopsies at a newly established dermatopathology unit within the Pathology Department of a major tertiary hospital in sub-Saharan Africa
Results: The median patient age was 35.0 years (IQR: 23.0–48.0), with near-equal gender distribution. The lower limb was the most common biopsy site (30.0%). Neoplastic conditions accounted for 38.9% of biopsies, with Kaposi sarcoma (20 cases) and basal cell carcinoma (14 cases) being the most frequent malignancies. Inflammatory dermatoses comprised 61.1% of cases, dominated by papulosquamous disorders (22.0%), particularly psoriasis and lichen planus. Infectious conditions represented only 5.9% of cases, with viral infections most common. Pigmentation disorders, autoimmune dermatoses, and other rare conditions were also identified.
Conclusion: This study highlights the diverse spectrum of dermatopathology cases encountered at our institution, with papulosquamous disorders and cutaneous tumors being the most frequently diagnosed categories. It also underscores the discrepancy between the broad range of skin conditions seen in the dermatology clinic and the relatively narrower subset selected for biopsy, reflecting the clinical thresholds and decision-making processes that guide histopathological evaluation.
INTRODUCTION
Skin diseases are among the most common human health conditions worldwide and represent a substantial source of non-fatal disease burden. According to the 2013 Global Burden of Disease study, dermatologic conditions rank as the fourth leading cause of disability-adjusted life years among non-fatal diseases.[1] This burden is especially significant in low-resource settings, such as sub-Saharan Africa, where skin disorders are often neglected yet remain widespread and underdiagnosed.[2] [3] [4]
In sub-Saharan Africa, the prevalence of skin diseases in population-based studies ranges from 27% to 80%, reflecting wide variability influenced by socioeconomic, environmental, and cultural factors.[2] [4] Conditions such as scabies, fungal infections, and other infectious dermatoses are particularly prevalent and are exacerbated by overcrowding, poor hygiene, malnutrition, and poverty.[5] [7] These diseases are also major contributors to the burden of neglected tropical diseases (NTDs).[1]
Urbanization and changing lifestyles have further complicated the landscape of dermatological conditions in the region. Increased exposure to chemical irritants in cosmetic products has led to a rise in allergic skin diseases, which were previously uncommon. This has resulted in a clear rural–urban divide in disease patterns, with infectious diseases such as scabies and tinea more prevalent in rural areas, and allergic or irritant dermatitis more common in urban populations.[1]
Given these geographic and socioeconomic disparities, understanding the local epidemiology of skin disease is critical. Although clinic-based studies provide some insight into disease burden, many dermatological diagnoses are made clinically without histopathological confirmation.[8] Only a minority of cases undergo skin biopsy, often when the diagnosis is uncertain or neoplastic disease is suspected.[9]
In 2016, a dermatopathology unit was established within the Department of Pathology at Aminu Kano Teaching Hospital (AKTH), providing an opportunity to study histologically confirmed skin diseases in this region. The AKTH dermatology clinic serves as a referral center and manages a wide spectrum of dermatologic conditions, including allergic, infectious, and neoplastic skin diseases. An average of 60 patients are seen weekly, including hospital and external referrals.
This study aims to describe the histopathological pattern of skin biopsies submitted from the AKTH dermatology clinic. Given that biopsy-confirmed diagnoses represent a subset of dermatologic disease with diagnostic uncertainty or severity, this analysis offers unique insights into the burden and nature of skin conditions requiring histological evaluation in northern Nigeria.
METHODS
This is a cross sectional hospital based study of all skin biopsies from the dermatology clinic that were sent to the dermatoapthology unit of pathology department of AKTH.
Study Design
We conducted a retrospective review of skin biopsy records of patients who were clinically diagnosed with skin pathologies at the Dermatology clinic of AKTH and subsequently underwent histopathological evaluation at the hospital pathology department. The data extracted included patients’ demographic information (age, sex), site of tissue biopsy, clinical and final histopathological diagnoses. Skin biopsy is undertaken exclusively using skin punch. The biopsies are sent to the department of Pathology of the same hospital for histopathologic diagnosis. Records were excluded if either clinical or histopathological diagnoses were non-specific diagnoses or absent. Ethical approval of the study was granted by AKTH Ethics Research Committee (AKTH/MAC/SUB/12A/P-3/VI/4047)
Study Site
The study was done at Aminu Kano Teaching Hospital, Kano, Nigeria. (AKTH) AKTH is a 600- bed teaching hospital serving the whole population of the Kano, which is the most populous state in Nigeria. The hospital also serves the population of neighbouring states like Katsina, Jigawa and Bauchi. AKTH operates a twice-weekly dermatology clinic which about 20,000 outpatients visit yearly. The dermatology clinic runs a robust residency program training dermatology resident’s doctor.
Data Analysis
Data analysis was executed using R statistical software, version 4.4.3 (R Statistical Corp., Vienna, Austria) and for all statistical procedures, a type 1 error rate was set at 5% (α=0.05). Descriptive statistic was used to summarize patient demographics and biopsy characteristics. Continuous variable was presented as mean and standard deviation (SD) or median and interquartile range (IQR) depending on the distribution, which was assessed using the Shapiro-Wilk test. Categorical variables were summarized using frequencies and percentages.
RESULTS
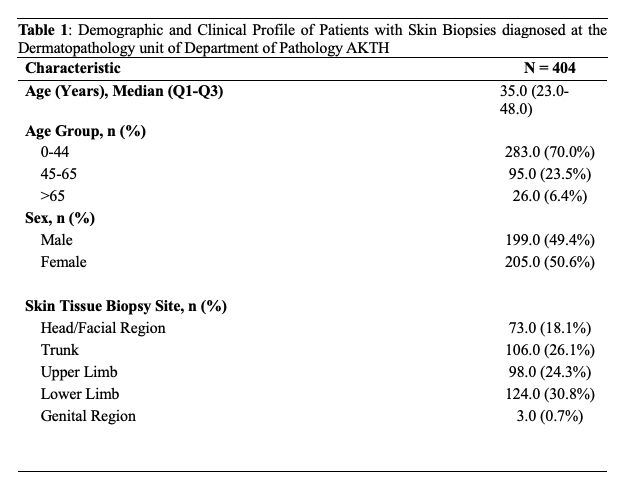
A total of 404 skin biopsies were documeted during the study period. Table 1 describes the demographic and clinical characteristics of the patients. The median age of the population is 35.0 years (23.0-48.0). The majority of the population is young with those less than 44 years accounting for 70% of the population, while those above 65 years constitute 4.5%.
Males account for 49.6% of the population with females comprising 50.6%. The lower limb is the predominant site of biopsy at 30.0%. This is followed by the trunk and upper limb at 26.1% and 24.3%. Biopsies from the head and neck region account for 18.1%. while the groin is the least common at less than 1% of cases.
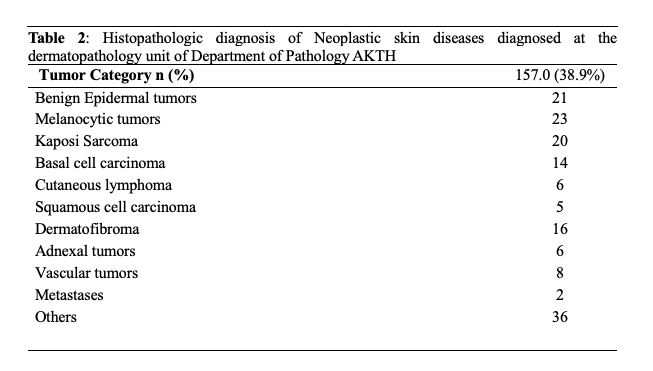
There was a wide distribution across the different skin categories. Table 2 describe the relative distribution of the neoplastic skin disease categories, which account for 38.9% of the total dermatopathology samples received. This sub category of the neoplastic diseases are: Melanocytic tumors accounts for 23 out of 103 cases, Benign Epidermal tumors 21 out of 103 cases, lymphocytic tumors 6 out of 103 cases, Metastatic tumors 1 out of 103 cases. Basal cell carcinoma 14 out of 103 cases, Squamous cell carcinoma 5 out of 103 cases, Kaposi sarcoma 20 out of 103 cases.
Amongst inflammatory dermatoses (Table 3), Papulosquamous dermatoses were the predominant. Psoriasis being the predominat accounted for 16 out of 89 cases followed by lichen planus with 13/89 cases. Pityriasis rubra pilaria and pityriasis lichenoides chronica each had 11 out of 89 cases. Pityriasis rosea and PLEVA each accounts for a single case. Eczematous disorders account for 4.5% (18 out of 89 cases). The predomint subtype was sub acute spongiotic dermatitis with 5 out of 18 cases, followed by chronic spongiotic dermatitis with 2 out of 18 cases.
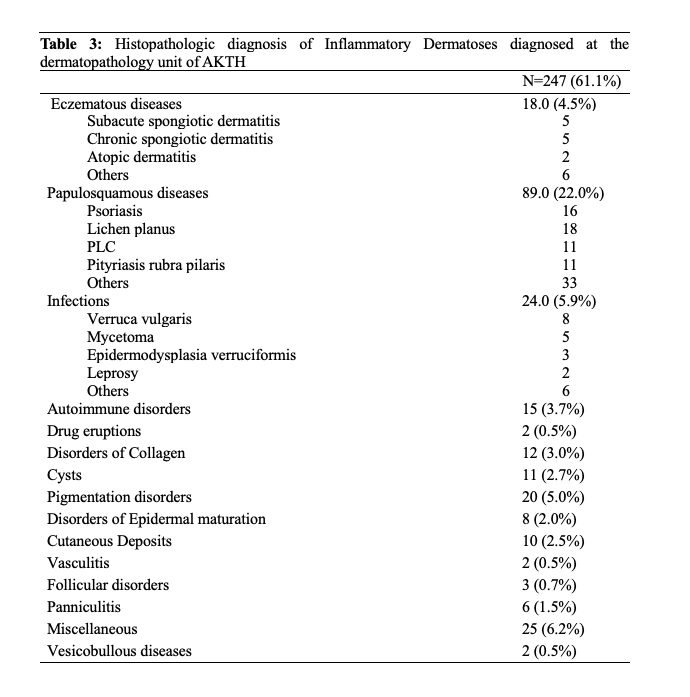
Atopic dermatitis account for 2 out of 18 cases, Follicular eczema, Seborrheic dermatitis, Allergic contact dermatitis, statsis dermatitis and peri orofacial dermatitis each had 1 case. The infectious diseases account for 5.9% (n=24). Viral infections were the most predominant and represented by verruca vulgaris with 8 out of 24 cases followed by EDV with 2/24 cases (). Parasitic infestations were seen in a single case each of leismaniasis and Schistosomiasis.
Pigmentation diseases comprised 5% (n=20 ); and the comprise Progressive macular hypomelanosis (PMH) 12/20 cases, Idiopathic guttate hypomelanosis (IGH) 3 out of 20 cases, ashy dermatosis, Pityriasis alba and post inflammatory hypopigmentation had 1 case each.
Autoimmune cutaneous disorder was made up of 15 cases, and was distrubuted as: lupus erythematosis 13 out of 15 cases and dermatomyosistis 2 out of 15 cases. Cutaneous deposits comprised 10 cases. Disorders of epidermal maturation comprised 8 cases, while follicular disorders and drug eruptions comprised 3 and 2 cases respectively. Panniculitides and Vasculitis are comprised 6 and 2 cases respectively. The miscellaneous group comprised 25 cases.
DISCUSSION
This study examined the pattern of dermatopathology biopsies received at a major dermatology clinic in Nigeria. Over the study period, 404 dermatopathology samples were analyzed. These biopsies represented approximately 3% of total patient visits to the clinic and just 1% of all surgical pathology samples processed in the pathology department.
The number of skin biopsies is not reflective of the total volume of dermatological diagnoses made at the clinic. This is primarily due to the clinical practice of diagnosing many skin conditions based on their characteristic appearance without histological confirmation. Additionally, many patients with advanced skin diseases, particularly neoplastic conditions, tend to present directly to surgical departments, further reducing the number of biopsies performed in the dermatology clinic.
The dermatopathology cases in this study encompassed the two major categories of skin diseases: neoplastic and inflammatory. Inflammatory dermatoses were more frequent, accounting for 61.1% of cases, while neoplastic lesions comprised 38.9%.
Among the neoplastic diseases, malignant lesions were predominant, with Kaposi sarcoma (KS) being the most common, followed by epithelial malignancies such as basal cell carcinoma (BCC) and squamous cell carcinoma (SCC). The high prevalence of KS may be attributed to its common clinical presentation as plaques and nodules, which frequently lead patients to seek dermatological consultation. Moreover, this finding likely reflects the significant burden of HIV in the patient population, consistent with previous studies.[11] A similar pattern was reported in Kenya, where KS was also the most prevalent skin malignancy.[13]
Conversely, other studies from Nigeria and other sub-Saharan African countries have reported SCC as the most common skin malignancy.[14] The lower frequency of SCC observed in our study may be due to advanced-stage cancers being managed predominantly in surgical departments. Notably, the relatively high number of BCC cases in this study may be linked to a substantial population of patients with albinism, who are at increased risk for this cancer.
Inflammatory dermatoses constituted the most common indication for biopsy, with papulosquamous disorders being the predominant subgroup, followed by infectious and eczematous conditions. While community- and clinic-based studies frequently report eczematous and infectious diseases as the most common skin conditions,[8-9] our lower biopsy rates for these diseases are likely due to their typical clinical presentations, which usually do not require histological confirmation. Biopsies were generally reserved for cases with diagnostic uncertainty.
Among papulosquamous diseases, lichen planus was the most common, followed by psoriasis and pityriasis lichenoides chronica (PLC). This pattern contrasts with an Indian study that reported psoriasis as the most common papulosquamous condition.[15] Our higher frequency of PLC and the singular case of pityriasis rosea diverge from findings by Yahya H. in Kaduna, Nigeria, who reported a higher prevalence of the latter.[16] This discrepancy may reflect diagnostic challenges in identifying pityriasis rosea clinically in our setting.
Infections were less frequently encountered in our biopsied samples, with viral etiologies being the most common. Although skin infections have been widely reported as prevalent in Nigeria and other regions,[9] their low representation in our dataset may be due to clinical diagnosis being sufficient in most cases. Only two cases of leprosy were recorded, despite the region’s known high prevalence. This may reflect the shift toward clinical diagnosis of leprosy; both cases biopsied in our study presented with atypical nodular lesions that warranted histological evaluation.[11]
Pigmentation disorders were infrequent, with post-inflammatory hyperpigmentation (PIH) and idiopathic guttate hypomelanosis (IGH) being most common. This contrasts with findings from Nnoruka EN in Enugu, Nigeria, who reported vitiligo as the predominant pigmentation disorder.[12] The difference may be due to varying patterns of healthcare-seeking behavior among patients with pigmentary disorders.
Based on our findings, we recommend strengthening dermatopathology services in Nigeria and the wider Sub- Saharan African region. This could include designating select pathology departments as centers of excellence, and fostering collaborative teams of dermatologists and pathologists to improve diagnostic expertise in dermatopathology. Given the growing acceptance and use of digital technology in the region, teledermatopathology can offer promising solution to bridge the significant diagnostic gap. Establishing partnerships with established dermatopathology centers in developed countries could further support training, capacity building, and knowledge exchange.
As our study is retrospective in nature, it is subject to certain limitations, including the exclusion of some clinical information due to missing data. Additionally, the study was conducted at a single tertiary hospital and only biopsy-proven cases were included and this may affect the generalizability to all skin diseases.
CONCLUSION
This study provides insight into the pattern of dermatopathology cases managed within a pathology department in sub-Saharan Africa. Papulosquamous disorders and cutaneous tumors were the most frequently biopsied lesions. Notably, this distribution differs from the broader spectrum of skin diseases typically encountered in community settings and dermatology clinics. These discrepancies have important implications for dermatopathology training and clinical practice in the region.
REFERENCES
- Seth D, Cheldize K, Brown D, Freeman EF. Global burden of skin disease: inequities and innovations. Curr Dermatol Rep. 2017;6(3):204–10. doi:10.1007/s13671-017-0192-7. PMID: 29226027; PMCID: PMC5718374.
- Figueroa JI, Fuller LC, Abraha A, Hay RJ. The prevalence of skin disease among school children in rural Ethiopia--a preliminary assessment of dermatologic needs. Pediatr Dermatol. 1996;13(5):378–81. doi:10.1111/j.1525-1470.1996.tb00704.x. PMID: 8893236.
- Komba EV, Mgonda YM. The spectrum of dermatological disorders among primary school children in Dar es Salaam. BMC Public Health. 2010;10:765. doi:10.1186/1471-2458-10-765. PMID: 21162714; PMCID: PMC3009652.
- Hogewoning A, Amoah A, Bavinck JN, Boakye D, Yazdanbakhsh M, Adegnika A, et al. Skin diseases among schoolchildren in Ghana, Gabon, and Rwanda. Int J Dermatol. 2013;52(5):589–600. doi:10.1111/j.1365-4632.2012.05822.x. PMID: 23557028.
- Canizares O. Epidemiology and ecology of skin diseases in the tropics and subtropics. In: A manual of dermatology for developing countries. Oxford: Oxford University Press; 1993. p. 22–35.
- Hay R, Andersson N, Estrada R. Guerrero, Mexico: community dermatology. Lancet. 1991;337:906–7.
- Ryan TJ. Healthy skin for all. International Committee of Dermatology. Int J Dermatol. 1994;33(12):829–35. doi:10.1111/j.1365-4362.1994.tb01014.x. PMID: 7883403.
- Akinkugbe AO, Amira OC, Ozoh OB, Bandele E. Pattern of skin disorders in a rural community in Lagos State, Nigeria. Niger Health J. 2016;16(2):1–15. doi:10.60787/tnhj.v16i2.251.
- Taal AT, Post EB, Hussaini T, Barminus AG, Dahiru T. First-line health care provider performance in the management of common skin diseases using an algorithmic approach in Kano State, Nigeria. Res Rep Trop Med. 2015;6:85–94. doi:10.2147/RRTM.S87600. PMID: 32669896; PMCID: PMC7337236.
- Sa DK, Kumar P. Clinicopathological consistency in diagnosis of skin disorders: a retrospective study of 371 histopathology reports. J Pak Assoc Dermatol. 2016;26:96–8.
- World Health Organization. WHO Expert Committee on Leprosy: Eighth report. WHO Tech Rep Ser. 2012;968:1–61.
- Nnoruka EN. Skin diseases in south-east Nigeria: a current perspective. Int J Dermatol. 2005;44(1):29–33. doi:10.1111/j.1365-4632.2004.02485.x. PMID: 15663655.
- Beltraminelli H, Kiprono S, Zuriel D, Swai B, Giabbani E, Grossmann H, et al. Dermatopathology in sub-Saharan Africa: a systematic 5-year analysis of all histopathological diagnoses from the Regional Dermatology Training Centre (RDTC) in Moshi, Tanzania. J Eur Acad Dermatol Venereol. 2015;29(7):1370–5. doi:10.1111/jdv.12877. PMID: 25438656.
- Okwor VC, Folasire A, Okwor CJ, Nwankwo K, Ntekim A, Arua CS. Clinico-epidemiological profile of skin cancer in South Western Nigeria. Malawi Med J. 2024;36(2):67–72. doi:10.4314/mmj.v36i2.2. PMID: 40191561; PMCID: PMC11970198.
- Patel M, Nijhawan M, Awasthi S, Rijhwan M, Nijhawan S. Clinical and histopathological study of papulosquamous skin disorders at a tertiary care center: a hospital-based prospective study. Afr J Biomed Res [Internet]. 2024 [cited 2025 Apr 10];27(3S):3604–13. Available from: https://africanjournalofbiomedicalresearch.com/index.php/AJBR/article/view/2988
- 16. Yahya H. Pityriasis rosea in Kaduna, North-West Nigeria: a 20-year experience. West Afr J Med. 2023;40(7):704–10. PMID: 37515778.
Medical Journal of Zambia, Vol 52, 5
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.