Magnitude and patterns of using earphones and relationship with hearing loss, tinnitus and dizziness among medical students at the University of Dodoma
Zephania Saitabau Abraham
Department of Surgery, School of Medicine and Dentistry, University of Dodoma, Dodoma, Tanzania
Fadhili Nelson
Department of Surgery, School of Medicine and Dentistry, University of Dodoma, Dodoma, Tanzania
DOI: https://doi.org/10.55320/mjz.51.4.576
Keywords:Earphones; hearing loss; tinnitus
ABSTRACT
Background: Due to online learning and medical students' recreational usage of headphones and earphones, the trend of their usage among adolescents and young adults has kept increasing thus at risk of noise induced hearing loss. No study has been done to determine the magnitude and patterns of earphones usage and their relationship with tinnitus, hearing loss and dizziness among medical students in Tanzania.
Objective: To determine the magnitude and patterns of using earphones and relationship with hearing loss, tinnitus and dizziness among medical students at the University of Dodoma, Tanzania
Methods: A descriptive cross-sectional study was conducted among 323 medical students at the University of Dodoma from April to July 2024. Data was analysed using Statistical Package for Social Sciences version 29.
Results: A total of 323 participants aged 18-35 years were enrolled. Majority were males, (66.6%) and male to female ratio was 1.99:1. The magnitude of earphone usage was 94.7%. Predominant earphone usage was among males, (66%). Regarding patterns of using earphones, majority preferred loud volume of listening, (33%) and 65.4% of medical students used earphones for more than 2 years. Majority of the participants reported to have used earphones for relaxation, (38.9%) and the common type of earphone used was Bluetooth device (IPOD), (25.2%). A remarkable magnitude of subjective hearing loss was found, 100% and on respective basis, 37.9%, and 26.8% of medical students reported to have experienced tinnitus and dizziness following earphone use. There was no statistically significant relationship between volume of listening using earphones and sex (p-value=0.317), academic year (0.137), campus status (p-value=0.723), fathers’ educational level (p-value=0.708), mothers’ educational level (p-value=0.449), fathers’ occupational status (p-value=0.133), place of residence (p-value=0.137) except for marital status (p-value=0.003), age (p-value=0.018) and mothers’ occupational status (p-value=0.045).
Conclusion: The study has found a remarkable magnitude of earphone usage among medical students, (94.7%) and all students who reported to have used earphones were found to have subjective hearing loss, (100%). On respective basis, 37.9%, and 26.8% of medical students reported to have experienced tinnitus and dizziness following earphone use.
INTRODUCTION
Earphone use is one of the contributing factors to tinnitus, noise-induced hearing loss and dizziness, which are issues of public health concern.[1] Among teenagers and young adults worldwide, about 1.1 billion have noise induced hearing loss (NIHL), mainly from the use of headphones and personal music players or other recreational noise.[2 ,3] Generally young people who listen to loud music, especially through headphones, are at an extremely high risk of noise-induced hearing loss.[4] Teenagers and young adults, notably college students, frequently use headphones for leisure as well as to watch lectures (video clips) online. These behaviours could make people more susceptible to tinnitus, hearing loss and dizziness caused by exposure to loud sound stimulus.5 Generally, NIHL is a major socioeconomic and public health issue in global context.6
Notably most teenagers and young adults tends to listen to their MP3 player at a maximum volume thus subjecting them to hours of loud music.[7 ,8] University students are not excluded from this group of teens and young adults thus posing them to be at risk of NIHL. In recent decades, headphone use has increased significantly following greater accessibility and affordability, which allows students with hectic schedules to listen to music in their free time or for stress relief.[6,9] Published studies have documented poor thresholds in terms of hearing among adolescents and young adults who use headphones compared to those who do not use headphones.[10 ,11,12]
In recent decades there has been a growing popularity of portable music players and devices such as cell phones that are connected directly to the ears and they may increase the magnitude of hearing loss among users of such devices.12 Due to increased usage of personal listening devices (PLDs), studies have documented increase in the power to hear sounds with higher frequencies, ringing sensation in ears or inability to hear others’ voice in noisy environment among teenagers.[12,13,14]
It is approximated that 90% of the population in industrialized countries such as United States tend to use cell phones and headphones.[6,15] Following the immense use of mobile phones by adolescents and young adults in both developed and developing countries, the radiofrequency fields emitted by mobile phones may damage people’s hearing ability thus causing NIHL.[6,16] NIHL occurs when the hair cells in the inner ear are destroyed by prolonged exposure to loud noise. Hair cells tend to convert sound energy that is mechanical in nature into an electrical signal, which then travels to the auditory processing region of the brain that is the temporal lobe. When these cells are damaged, they are unable to regenerate.[6,17]
To document the findings on earphones and music player devices use by adolescents and young adults, a study that was done in Iran found 36.8% of the high school students to have listened music continuously without any rest or stop, 49.6% of the students reported listening to ‘somewhat loud’ or ‘very loud’ music and 44.3% of the respondents reported a history of hearing problems in the past.12 Another descriptive study in Iran found 91.2% of the college students to have used headphones, 10.4% of the students used headphones more than one hour a day, and 52% of the students set higher than three-fourths of the output capacity when using their headphones.,18] From the available literatures, there is not any study that has been conducted in Tanzania aiming at determining the magnitude of hearing loss among earphone users and assess whether there is any existing relationship between earphone usage and hearing loss, tinnitus and dizziness.
Despite such an observed trend elsewhere of adolescents and young adults including university students being more vulnerable to noise induced hearing loss, tinnitus and dizziness following recreational use of earphones and also for academic purposes, there is not any study to date of this type that has been conducted in Tanzania specifically at the University of Dodoma. The aim of this study was thus to determine the prevalence of earphone use and ascertain the patterns of using earphones and establish the existing relationship between earphone usage and hearing loss, tinnitus and dizziness among university students.
METHODS
Study design, area and study duration
It was a university-based cross-sectional study that was conducted at the University of Dodoma, School of Medicine and Dentistry from April to July 2024. As per 2023/2024 academic year, the number of medical students per class who are pursuing Doctor of Medicine are; first year (210 students), second year (190 students), third year (248 students), fourth year (160 students) and fifth year has 164 students, and all these adds up to 900 medical students. The University is located at Chimwaga area about 8 kilometres east of Dodoma town centre, within Dodoma city and covers an area of about 15000 acres (6000 hectares). The site has a very prominent view as it is situated on a hilly area.
Study population
The study population included medical students at the School of Medicine and Dentistry at the University of Dodoma
Sampling technique
Proportional cluster sampling method was used in selection of the desired sample where a list of classes was obtained from medical school at the University of Dodoma and classes were chosen upon being divided into homogenous clusters with consideration being taken on the number and sex of students in each class to ensure homogeneity of the chosen clusters. To mitigate bias in cluster sampling technique, probability sampling method was utilized coupled with larger sample size.
Sample size estimation
The representative sample from the target population was obtained using Kish and Leslie formula that is given by
Where by N stands for Sample size, Z stands for Standard normal deviate which is equal to 1.96 for 95% confidence level and P stands for Propotion, which equals to 73.3% which was the proportion of students who used personal audio devices in the United Arab Emirates.[19] E corresponds to margin of error which was assumed to be 5%. Therefore, N=~301. The minimum estimated sample was 301
Adjusting for non-response rate (f% assumed to be 10%) (Smith and day-1984) due to the possibility of unavailability of the sampled units since some university students may be attending field works outside the university or moving from one teaching hospital to another when data was to be collected. Then N’=N x adjusted factor (100%/100%-f %); N’=301 X (100%/100%-10%) =334. Therefore, the adjusted required sample size was 334 medical students. However, the study recruited a total of 323 medical students.
Inclusion criteria
All medical students from the University of Dodoma, School of Medicine and Dentistry (from first to fifth year of their training) who consented to participate
Exclusion criteria
Medical students who did not consent to participate in this study and medical students with no history of using earphones or personal assisted hearing devices during their lifetime even at a single occasion.
Data collection tools
A semi-structured questionnaire using KoboTool box was used as the data collecting technique to determine the magnitude and patterns of using earphones and relationship with hearing loss, tinnitus and dizziness among medical students at the University of Dodoma. To gather as much data as possible, the questionnaire consisted of both closed- and open-ended questions. It was adapted from previously published studies and changed to suit the set objectives.[6 ,12] Moreover, reviewing the literature as well as pilot testing the instrument prior to the study by involving 10% of the actual sample size from the university and who were excluded from the actual study assessed validity of the tool.
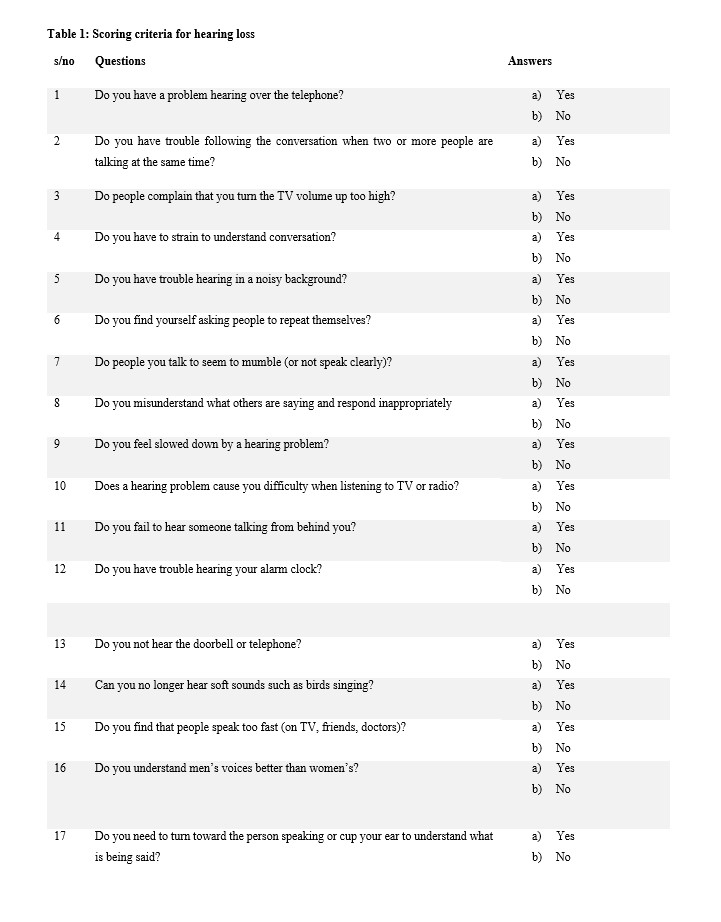
Scoring criteria for subjective hearing loss using an adapted 17-item hearing loss questionnaire
The 17-item hearing loss questionnaire, which was adapted from Mohammadpoorasl et al., 2019, was used to assess medical students' self-reported hearing loss. "No" responses was scored as 1 in this study, while "Yes" replies was coded as 2. The range of scores was 17–34, where a higher score denoted more severe hearing loss. For a medical student to be considered to have hearing loss, the overall score was 17 and above.[12]
Measurement of variables
Dependent variables: The dependent variables for the study were (i) magnitude of using earphones (ii) patterns of using earphones (iii) occurrence of hearing loss (iv) occurrence of tinnitus (v) occurrence of dizziness among medical students (vi) occurrence of other otological complaints such as otalgia
Independent variables: The independent variables for the study were (i) socio-demographic characteristics of the medical students (age, sex, academic year, living status as to whether in campus or off campus, marital status, place of residence, marital status, fathers’ educational level and occupation, mothers’ educational level and occupation.
Data processing and analysis
After data collection, data was stored in a computer and other external devices for easy accessibility and security. Data entry was done using an epidata software. Data was analysed using Statistical Package for Social Sciences (SPSS) version 29 software. Descriptive statistics was performed for the obtained data. A p-value <0.05 was considered to be statistically significant.
Ethical approval and consent to participate
Ethical clearance was obtained from the Ethics and Research Committee of the University of Dodoma with an approval number MA.84/261/74/40. All prospective participants were required to sign a consent form after being given appropriate information about the importance of this study before their recruitment. Instructions were given to the study participants before their recruitment. The Participants were informed that their participation is voluntary and any person may/may not wish to participate provided that they meet the criteria for inclusion in the study. Data collected from this study was kept strictly confidential. To maintain confidentiality, names of students that may be identifiers were not recorded in the questionnaires but rather numbers were coded. Furthermore, the information obtained from the study participants was not provided to other people who were not involved in the study and this also aimed to maintain confidentiality.
RESULTS
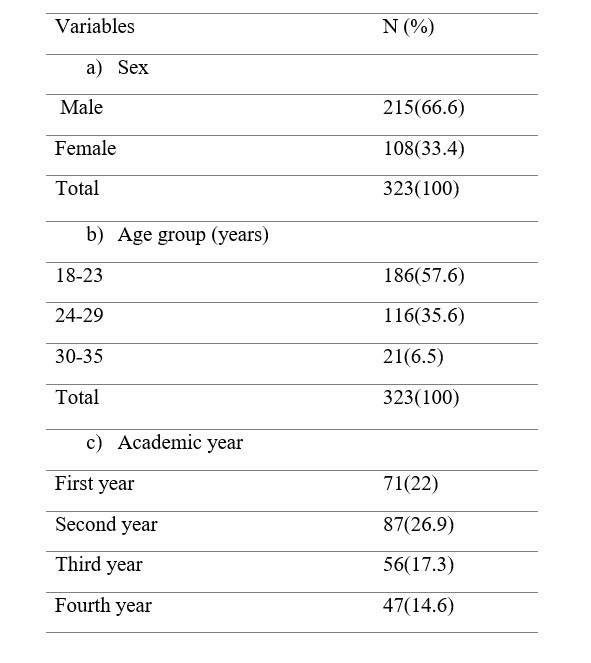
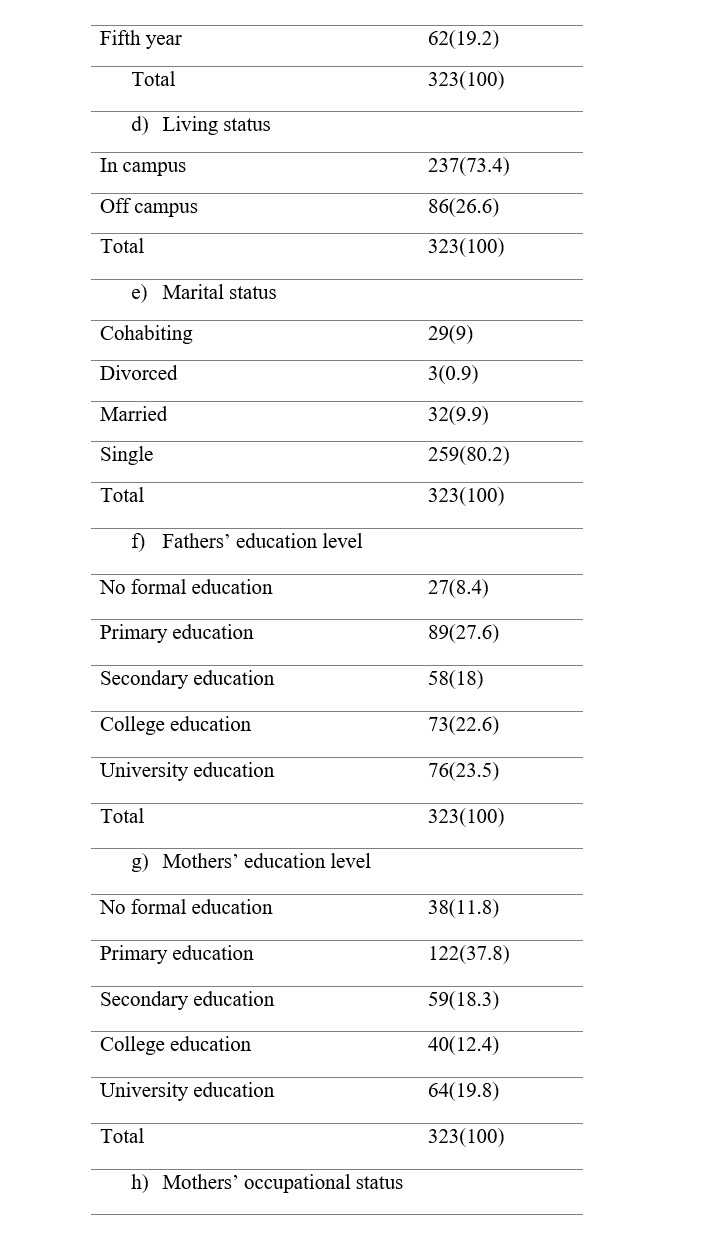
Socio-demographic characteristics of the participants
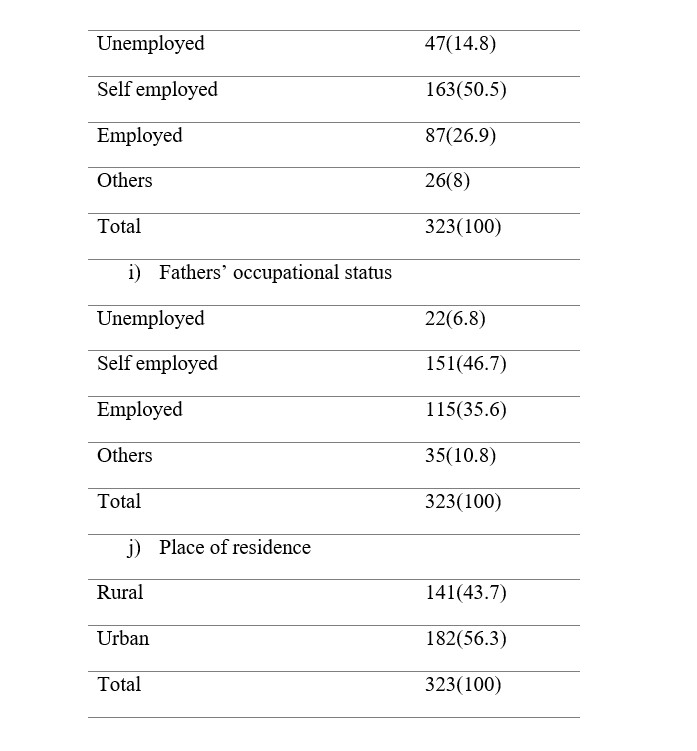
In this study, a total of 323 medical students were recruited, where majority were from urban area, 182 (56.3%) while those from rural area were 141 (43.7%) students. Male participants were 215 (66.6%) and females were 108 (33.4%) (M: F =1.99:1). Majority of the participants were aged 18-23 years, 186 (57.6%) and least number of participants were aged ≥ 30 years, 21(6.5%). Most of the participants were from second year, 87 (26.9%), and least were from fourth year, 47 (14.6%) of their medical training. Similarly, the study found majority of the students to be living in campus, 237 (73.4%) and pertaining marital status of the participants those who were single were, 259 (80.2%) medical students. Regarding fathers’ and mothers’ education level, primary level education was reported by 89 (27.6%) and 122 (37.8%) medical students respectively and least number of medical students reported no formal education of their fathers’ and mothers’ and this was accounted by 27 (8.4%) and 38 (11.8%) medical students. Pertaining occupational status of both mothers’ and fathers’ of the recruited medical students, majority were self-employed as reported by 163 (50.5%) and 151 (46.7%) medical students respectively. (Table 2)Table 2: Socio-demographic characteristics of the participants
The magnitude of using earphones among medical students
In this study where 323 participants were recruited, 306 (94.7%) medical students reported to have used earphones while 17 (5.3%) medical students did not use earphones. (Figure 2)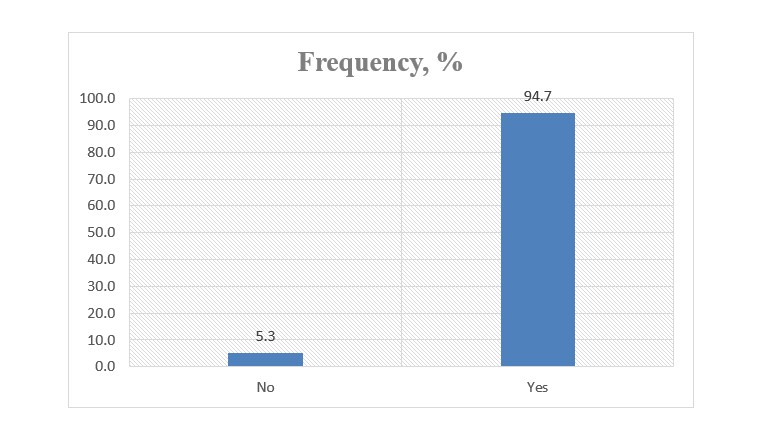
Patterns of using earphones among medical students
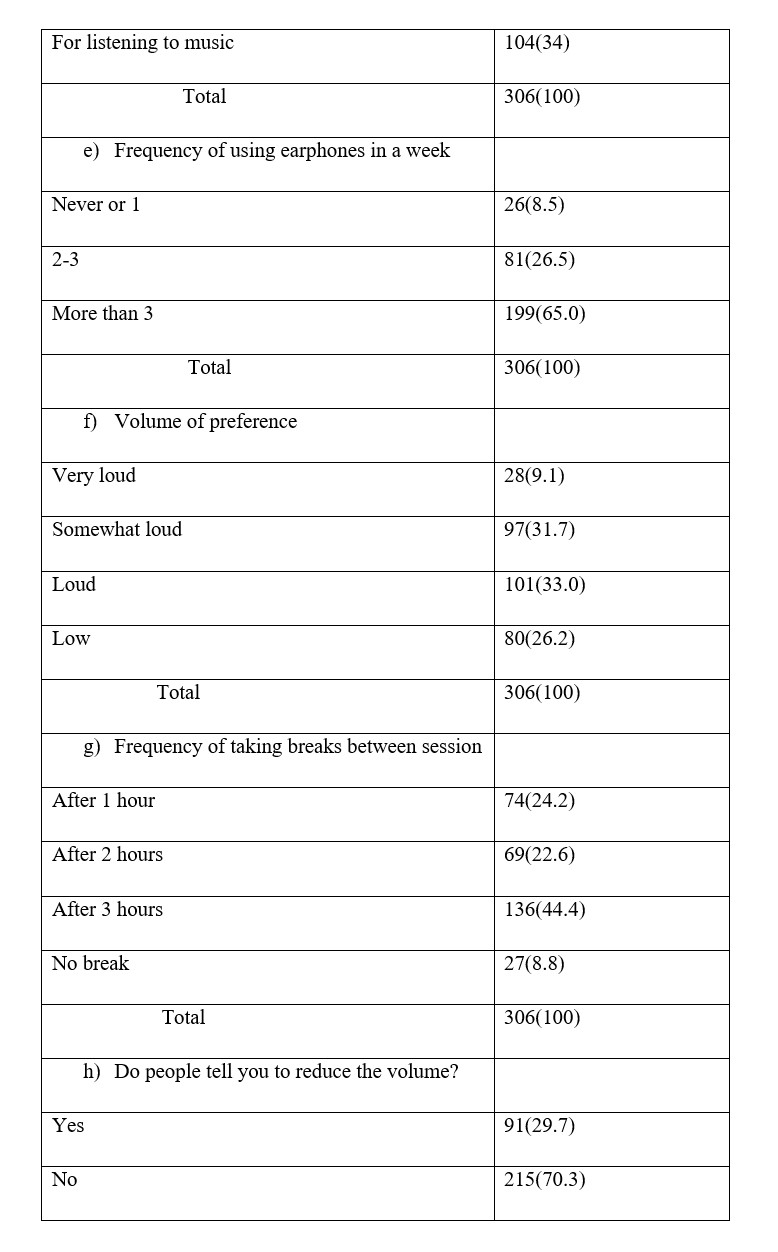
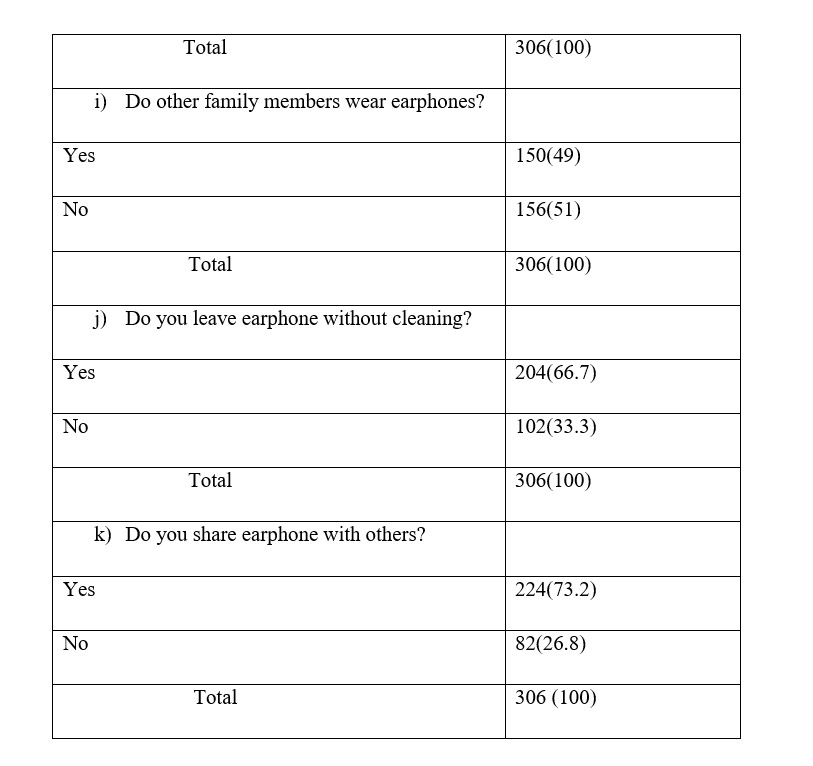
The study found majority of the participants to have reported to use combined type of earphones, 131 (42.8%), and least used insertion type of earphone, 49 (16%). Also majority, 77 (25.2%) used bluetooth device (IPOD) followed by combined bluetooth device and headphones, 73 (23.8%) while minority of the participants used headphones, 39 (12.7%) as form of audio device. In assessing the duration of using earphones, majority of medical students reported to have used for more than 2 years, 200 (65.4%) and least used for less than a year, 49 (16%). Majority of the medical students reported to have used earphones at a frequency of more than 3 times in a week, 199 (65%) and least, 26 (8.5%) reported to have never used earphones or used only once in a week. In addition, majority preferred loud volume of listening, 101 (33%) and most of the medical students used to take breaks after 3 hours in between session of listening earphones, 136 (44.4%). In assessing the reasons for using earphones, majority reported to have used earphones for relaxation, 119 (39%) followed by listening to music, 104 (34%) and least number of medical students reported to have used earphones for gaming, 12 (3.9%). On the other hand, majority of the medical students, 215 (70.3%) reported not to have been told to reduce the volume of audio device by people who are nearby, 150 (49%) medical students reported that other family members wear earphones, 204 (66.7%) medical students reported to leave earphones without cleaning while 224 (73.2%) medical students used to share earphones with others. (Table 3)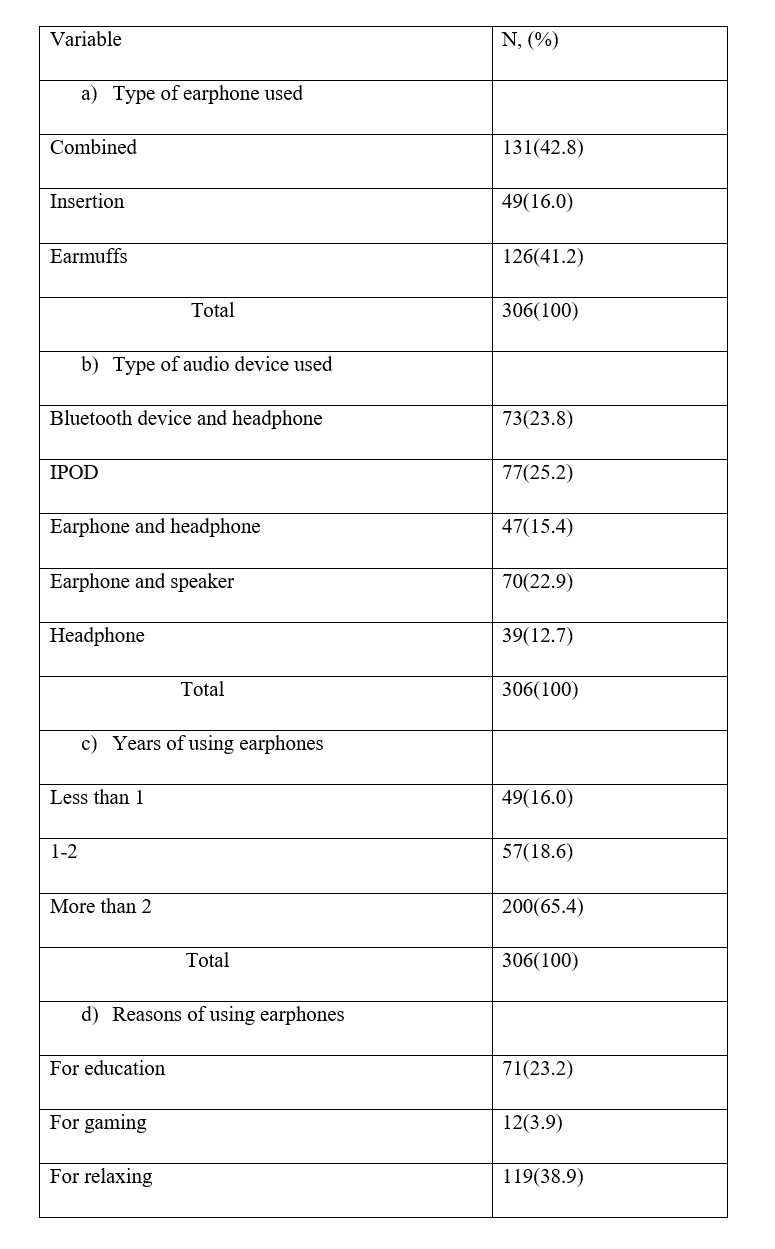
Prevalence and severity of hearing loss among medical students who are earphone users
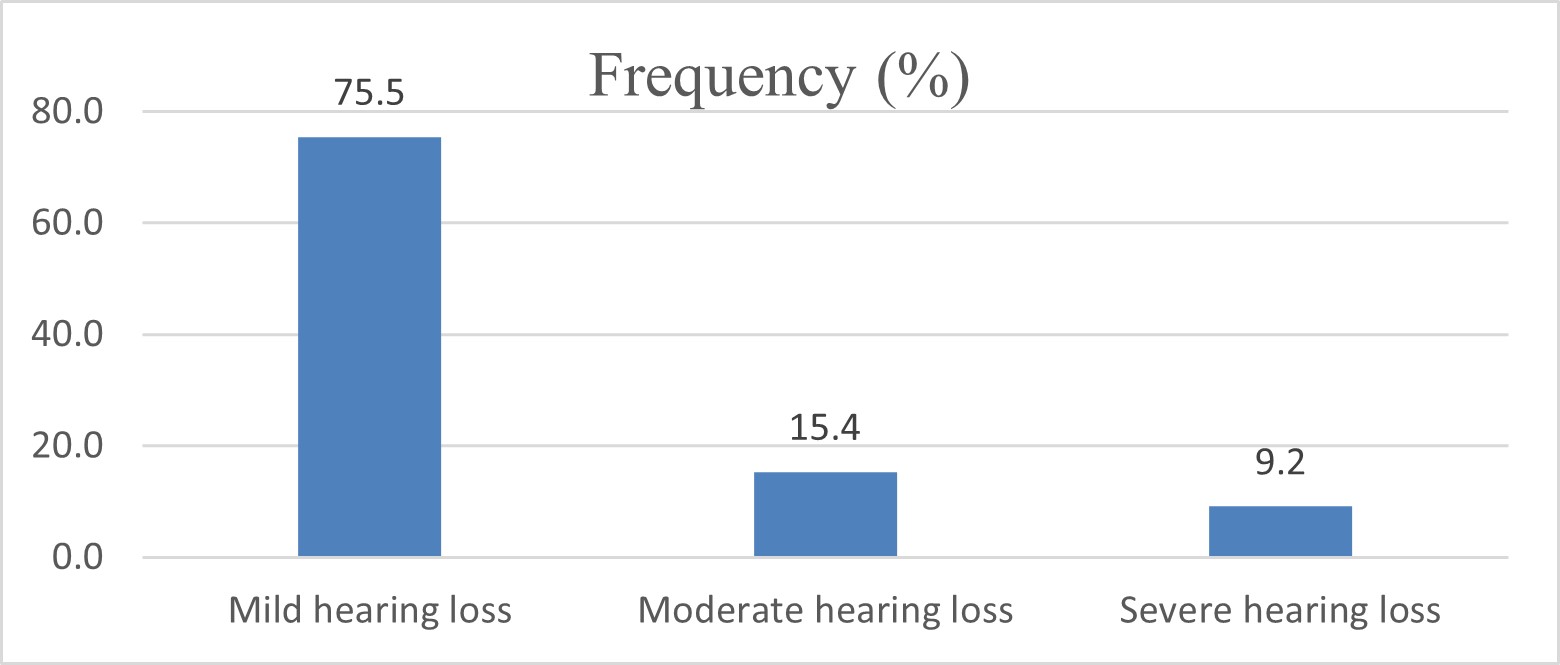
In this study, all the study participants, 100% (306/306) who were earphone users were found to have hearing loss as established on subjective basis. Regarding the severity of hearing loss on subjective basis, most of the study participants had mild hearing loss, 231 (75.5%) while 47 (15.4%) medical students had moderate hearing loss and 28(9.2%) medical students had subjective severe hearing loss. (Figure 3)
Self-reported magnitude of tinnitus, dizziness and history of experiencing other otological complaints among medical students who are earphone users
In assessing the self-reported magnitude of dizziness, tinnitus and history of experiencing other otological complaints among medical students who are earphone users, 82 (26.8%) medical students reported to have experienced episode of dizziness after using earphone (Figure 3) and 116 (37.9%) medical students reported to have experienced tinnitus. (Figure 4) Pertaining history of experiencing other otological complaints among medical students who were using earphones, the study found majority of the students to have reported history of ear itching, 99 (32.4%), followed by sensation of ear fullness, 46 (15%) while least number of participants reported ear pain, 2 (0.7%) and headache, 3 (1%). (Figure 5)
The relationship between volume level of listening using earphones and socio-demographic characteristics of medical students
a) Sex and volume level of listening using earphones
When analyzing the relationship between sex and volume level of listening using earphones, it was observed that the majority of male students listened at a loud volume, 70 (34.7%), and equal number of female students listened to loud and somewhat loud volume, 31(29.8%). Generally, male students preferred loud volume of listening, 70 (34.7%) compared to female students, 31 (29.8%). There was no a statistically significant relationship between sex and volume level of listening using earphones (p-value= 0.317). (Table 4)
b) Age and volume level of listening using earphones
In this study, most participants aged 18-23 years preferred loud volume of listening, 63 (34.8%) followed by somewhat loud, 57 (31.5%), while majority of those aged 24-29 years preferred somewhat loud volume of listening, 37(34.3%). The relationship between age and volume of listening using earphones was not statistically significant (p-value=0.018). (Table 5)
c) Academic year and volume level of listening using earphones
Most of the first year students preferred loud volume of listening, 23(33.3%), second year preferred mostly somewhat loud volume, 32(38.1%), third year preferred loud volume, 22(41.5%), fourth year preferred mostly, somewhat loud volume, 15(34.1%) and fifth year preferred loud volume of listening, 22(39.3%) when using earphones. The relationship between academic year and volume of listening using earphones was not statistically significant (p-value=0.137). (Table 6)
d) Place of living (campus life) and volume level of listening using earphones
Majority of the in campus medical students listened earphone in somewhat loud volume, 30 (37.5%) while off campus medical students preferred to listen in somewhat loud volume, 73 (32.3%). There was no association between where the medical students live and volume level of listening using earphones (p-value=0.723). (Table 7)
e) Marital status and volume level of listening using earphones
Most of the medical students who were cohabiting and single preferred loud volume, 9 (39.1%), and somewhat loud volume, 82 (32.5%) respectively. However, those who were divorced preferred equally both loud (50%) and somewhat loud volume (50%) while using earphones. The relationship between marital status and volume of listening using earphones was statistically significant. (p-value=0.003). (Table 8)
f) Fathers’ educational level and volume level of listening using earphones
Majority of fathers’ of medical students with no formal education, primary level of education and university level of education preferred loud volume of listening, 9 (36%), 28 (35%) and 26 (35.6%) respectively. This was contrary to those with secondary and college level of education who favored somewhat loud volume of listening, 21 (36.8%) and 24 (33.8%) respectively. No association was established between fathers’ educational level and volume of level of listening using earphones since p-value=0.708. (Table 9)
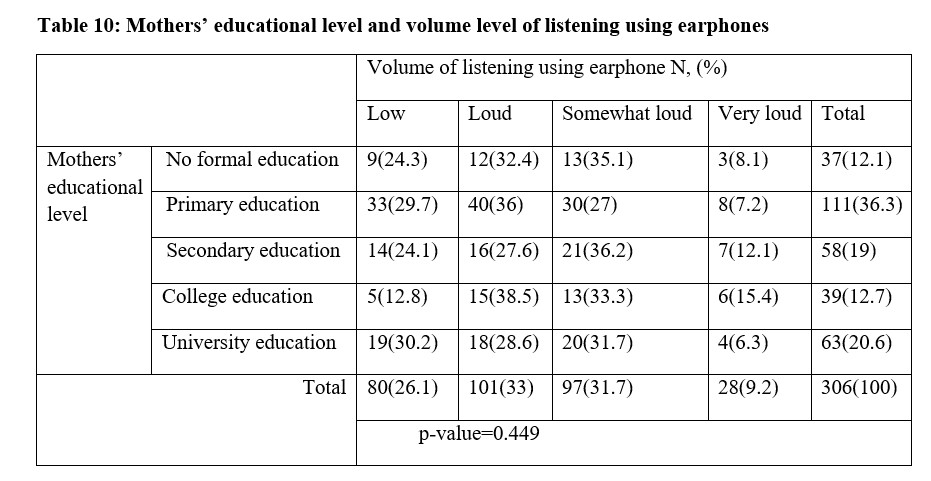
g) Mothers’ educational level and volume level of listening using earphones
Majority of mothers’ of medical students with no formal education, secondary and university level of education preferred somewhat loud volume, 13 (35.2%), 21 (36.2%) and 20 (31.7%) respectively but those with primary and college level of education preferred loud volume, 40 (36%) and 15 (38.5%) respectively. There was no a statistically significant association between volume level of listening using earphones and mothers’ educational level (p-value=0.449). (Table 10)
h) Mothers’ occupational status and volume level of listening using earphones
Majority of mothers’ of medical students who were unemployed and self-employed preferred loud volume, 20 (42.6%) and 56 (35.9%) respectively. This was contrary to those who were employed where majority preferred somewhat volume, 31(39.2%) and those with other occupational status preferred low volume of listening, 12(50%). Among those who were self-employed majority preferred loud volume of listening using earphones, 56 (35.9%). There was a statistically significant association between mothers’ occupational status and volume of listening using earphones (p-value=0.045). (Table 11)
i) Fathers’ occupational status and volume level of listening using earphones
In assessing fathers’ occupational status of medical students and volume level of listening using earphones, it was found that majority of medical students whose parents were unemployed and employed preferred to use loud volume of listening, 10 (47.6%) and 38 (34.5%) respectively. However, majority of self-employed and those with other occupation preferred somewhat volume of listening, 48 (33.1%) and 12 (40%) respectively. The study found no association between fathers’ occupational status and volume level of listening using earphones (p-value=0.133). (Table 12)
j) Place of residence and volume level of listening using earphones
This study found majority of rural residents, 44 (33.1%) to have preferred listening to low volume, followed by somewhat loud volume, 41 (30.8%) contrary to urban residents where majority preferred loud volume, 65 (37.6%) followed by somewhat loud volume of listening, 56 (32.4%). The study found no statistically significant relationship between place of residence and the volume level of listening using earphones (p-value=0.137). (Table 13)
k) Ordinal regression analysis for some selected socio-demographic characteristics of students
On ordinal regression analysis age was significantly associated with listening to loud volume where those aged 18 to 23 years were 2 times more likely to use loud volume of listening using earphones (OR=2.927;95%CI (0.978-8.756),P=0.045). Additionally, no significant statistical association was shown between various academic years and volume level of listening however, first year students were 2 times more likely to use loud volume of listening using earphones than fifth year and fourth year students. Place of residence was found to be statistically associated with volume level of listening using earphones where those who lived in rural area were 2 times more likely to listen to loud volume than urban residents (OR= 2.074;95%CI (1.198-3.591),P=0.009) (Table 14)
DISCUSSION
Due to increase usage of earphones, it has been reported to be associated with remarkable health effects of public health significance being mainly noise induced hearing loss. Therefore, this study was designed to determine the magnitude and patterns of using earphones and relationship with hearing loss and tinnitus among medical students who were earphones users. Regarding magnitude of earphone usage among medical students, 94.7% reported to have used earphones. This finding appears to be similar to other studies done in Iran and India where 86.4% and 97.7% of the respondents respectively reported to have used earphones.[12,20] In this study 66% of males used earphones whereas 34% of females also used earphones. Such findings appear to be like those from a study done in India where 68% of male students had used earphones.[5] Dissimilar findings were depicted from other studies done in India and Iran where more earphone usage was among females by 57.1% and 64.5% respectively.[12,20]
In this study majority of the participants preferred combined type of earphone (42.8%) and Bluetooth devices (iPod), (25.2%). Such findings were similar to those from a study done in India where 31.7% had used Bluetooth device[20] contrary to what was found in the study that was done in India where Bluetooth earphone usage was reported by 7% of the respondents.[21]
Pertaining patterns of using earphones among medical students, majority preferred loud volume of listening, (33%). Such finding appear to be similar to those obtained from two studies done in Iran where participants preferred somewhat loud volume of listening by 28% and 49.6% respectively.[7,12] 7,12 Similarly, another study done in the United Arab Emirates showed majority of the participants to have preferred very loud volume of listening using earphones, (41.8%).[19] In this study, majority of the participants used earphones for more than 2 years, (65.4%). Similar findings can be depicted from the study done in Iran among students where 61.5% used earphones for more than 2 years. When assessing the frequency of earphone usage in a week, 65% of the participants reported to have used earphones more than 3 times in a week contrary from the same study done in Iran where majority, (40.3%) reported to have used earphones 2 to 3 times in a week.[12] The reason for the observed difference can be due to hectic schedules of medical students at the University of Dodoma who tends to use earphones for academic purposes compared to students from the study done in Iran thus more tendency of using earphones compared to counterparts.
Regarding the reason for using earphones by medical students, this study has found majority of the participants to have used earphones for relaxing,(38.9%) followed by listening to music, (34%). Dissimilar finding can be depicted in the study done in Saudi Arabia where most participants used earphones for listening music, (68.9%) followed by educational purposes, (44.6%).[22] This study found, 44.4% of the medical students to have taken break after 3 hours of using earphones which was different from what has been observed in the study that was conducted in the United Arab Emirates where majority of the participants took breaks after 1 hour of using earphones, (56.5%). In addition, 70.3% of the medical students in this study reported not to be told by people around them to reduce volume when using earphones. Dissimilar findings can also be depicted from the same study that was done in the United Arab Emirates where majority of the participants, (64.5%) reported to be told by people around them to reduce volume when using earphones.[19]
Regarding self-reported magnitude of hearing loss, all the participants had subjective hearing loss, (100%). Such significant magnitude of subjective hearing loss among medical students who were earphone users can be depicted in the study done in Iran where 60.2% of them had subjective hearing loss.[12] On the other hand, lesser magnitude of hearing loss among medical students who were earphone users has been found in the study that was done in India where 10.6% of them had hearing loss.[23] The reason for these differences can be explained by differences in the tool used in assessing hearing loss among medical students who were earphone users where our study used the 17-item questionnaire adopted from Mohammadpooras et al while Basu et al used 5-item Likert type scale with options ranging from 1 (very likey) to 5 (unlikely). On the other hand, the reason for the higher prevalence of subjective hearing loss among local Tanzanian students can be due to remarkable earphone usage by university students for various reasons such as relaxation and following lectures and its well known that earphone usage is associated with noise induced hearing loss.
Pertaining the occurrence of tinnitus among medical students who were earphone users, this study has found 37.9% of the medical students who were earphone users to have had tinnitus and this finding appear to be contrary to that from Iran where 8.8% of medical students who used earphones reported tinnitus.[12] The observed differences in these studies may be attributed to high frequency of earphone usage among medical students at the University of Dodoma compared to students in Iran. Another study from Indonesia found almost similar findings where 27% and 8.1% of risky and non-risky earphone users respectively experienced tinnitus and this appear to depict similarity to the significant magnitude of tinnitus among earphone users.[24]
Regarding the occurrence of dizziness among students who were earphone users, 26.8% of the medical students who were earphone users reported dizziness. This finding appear to be similar to that from the study done in Iran where 23.6% of medical students who were earphone users had experienced dizziness.[12] However, the magnitude of dizziness in this study appear to be somewhat higher compared to the study done among Iranian teenagers where 18.8% of them reported dizziness.[7] Regarding reported history of other otological complaints among medical students who were using earphone, majority had ear itching (32.4%) and least reported ear pain (0.7%) contrary to a study done in India where majority had headache (41.9%) followed by ear pain (36.1%) and itching was reported by 27% of the participants who were using earphones.[20]
Pertaining the relationship between volume level of listening using earphones and socio-demographic characteristics of medical students, this study has found 34.7% of male students to have preferred loud volume compared to female students, (29.8%). Additionally, those aged 18-23 years preferred loud volume, (34.8%) and those aged 24-29 years preferred somewhat volume of listening using earphones, (34.3%). Generally, this study has found no statistical significance between most of socio-demographic characteristics and volume level of listening using earphones (p-value>0.05). However, statistical significance was observed between marital status of medical students and volume level of listening using earphones (p-value=0.003) where those medical students who were single preferred somewhat loud volume of listening using earphones, (32.5%). Such findings were different from those found in the study that was conducted in Iran where majority of those aged 18-21 years, 54.3% preferred very loud volume (gain setting more than 50%) of listening using earphone.[12] Similarly, findings from this study appear to be different from those reported in the study done in India among medical students where majority of male students preferred low volume level of listening using earphones, (57%) compared to female students, (54.8%).[23]
Generally, clear interventions should be laid by the Ministry of Health and other stakeholders through policies aiming at educating university students on health consequences related to earphones usage. This should be made with greater efforts since the magnitude and pattern of earphones use may be worse in other universities particularly those offering non-health related courses as they lack detailed awareness on health related impacts of using earphone usage.
Study limitations
This study has utilized a small sample size where it only included medical students from the University of Dodoma and therefore results may not be generalized to students at the University of Dodoma or medical students in Tanzania at large.
Additionally, no objective hearing test (audiometry) was performed rather the study used only the 17-items questionnaire that was adopted from Mohammadpoorasl et al where all participants had subjective hearing loss. Therefore, it was required to study these participants with the use of audiometry to understand the exact number of participants with actual hearing loss. The study has however paved a way for further researches to done among university students to determine the magnitude of earphone use and ascertain relationship to hearing loss, tinnitus and dizziness in an objective manner. Such future studies are important in preventing the young generation from being deaf with time due to their remarkable habit of using earphones for various reasons such as relaxation and academics.
CONCLUSION
The study has found a remarkable magnitude of earphone usage among medical students at the University of Dodoma and all the students who reported to have used earphones were found to have subjective hearing loss. Less than half of the recruited students who used earphones reported to have experienced tinnitus, dizziness and other otological complaints such as ear itching, ear pain, ear fullness and ear discharge. Future researches should be done among university students to determine the magnitude of earphone use and ascertain relationship with hearing loss, tinnitus and dizziness by aid of pure tone audiometry. Health education as a means of intervention should be provided to university students on health-related consequences of earphones us such as associated sensorineural hearing loss, otalgia, tinnitus and dizziness.
Authors’ contributions
Authors contributed as follows to the conception or design of the work; the acquisition, analysis, or interpretation of data for the work; and drafting the work or revising it critically for important intellectual content: ZSA contributed 55% while FN contributed 45%, All authors approved the version to be published and agreed to be accountable for all aspects of the work
Statements and declarations
Ethics approval and consent to participate
Informed consents were obtained from medical students and ethical clearance was obtained from Ethics and Research Committee of the University of Dodoma
Data availability
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author
Competing interests
The authors declare that they have no competing interests
Funding
No funding source to be declared
Consent for publication
Not applicable
REFERENCES
Medical Journal of Zambia, Vol 51, 4
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.