Recurrent Lactation Anaphylaxis: A case report from Zambia
Moses Chirwa
Zambia Association of Gynaecologists and Obstetricians, formerly Chipata Central Hospital, Department of Obstetrics and Gynaecology 1. Zambia Association of Gynaecologists and Obstetricians, formerly Chipata Central Hospital, Department of Obstetrics and Gynaecology
Melinda Katongo
Chipata Central Hospital, Department of Obstetrics and Gynaecology
DOI: https://doi.org/10.55320/mjz.51.3.565
Keywords:lactation, anaphylaxis
ABSTRACT
Lactation anaphylaxis is a rare condition that occurs during the postpartum period and is characterised by respiratory, gastrointestinal, and cardiovascular symptoms. This is a case report of a 31-year-old para 3 woman who presented at the Adult Emergency Department with lactation anaphylaxis, a rare condition with only 10 cases reported at the time of reporting our case. She presented with difficulties in breathing, pruritis, urticaria, and angioedema. Her symptoms were severe during periods of exclusive breastfeeding. She was treated with a corticosteroid and antihistamines which worked to good effect. The symptoms completely resolved after cessation of breastfeeding. She had similar symptoms with her second child but had none with her first child. This case shows that lactation anaphylaxis can be recurrent and responds well to standard treatment for anaphylactic reactions.
INTRODUCTION
Lactation anaphylaxis is rare with very few cases reported in the past 30 years [1] . Our search on MEDLINE, PubMed and Google Scholar identified 10 previous case reports reporting about the condition. Patients usually present in the Adult Emergency Department (AED) units with respiratory, gastrointestinal, and cardiovascular symptoms. Literature suggests that hormonal changes that occur in the mother after birth can cause an exaggerated histamine response that can trigger anaphylactic reactions [1] . This response has been suggested to be an IgE-independent reaction that occurs due to the drop in progesterone following childbirth coupled with a relative increase in oestrogens resulting in the degranulation of mast cells and therefore release of histamines [2] . However, some case studies have reported findings of normal IgE levels in women with lactation anaphylaxis [3] . Another possible mechanism proposed is the rapid reduction of other steroids and a rise in prolactin which occurs postnatally [1] . Steroid hormones suppress mast cell degranulation and therefore this drop in steroids postnatally results in loss of suppression of mast cell activity [1] . During pregnancy, there is an increase in mast cell population and a rise of steroid hormones such as progesterone. Mast cell degranulation is stabilized by an increased amount of progesterone, a steroid hormone and corticosteroids that are released during labour [4] . However, the steroid hormones fall during the postpartum period to induce lactogenesis. This drop in progesterone and other steroid hormones postnatally has been thought to trigger exaggerated mast cell response in women with lactation anaphylaxis [4] .
Other case reports have also documented the potential roles of prolactin surge, oxytocin, adrenocorticotropic hormone (ACTH), and corticotropin-releasing hormone (CRH) in the aetiology of lactation anaphylaxis [3] . Lactogenesis usually gets established around 48 to 72 hours after delivery hence most previously reported cases report that patients experience anaphylaxis symptoms at least 2 days after delivery of the baby [5] .
Mast cell degranulation can be confirmed through a rise in serum tryptase that can occur within 15 minutes to 3 hours of the onset of symptoms. Some women with lactation anaphylaxis have shown an increase in serum tryptase while it’s been negative in others [1] . Skin prick tests have also been shown to be insignificant for the diagnosis of lactation anaphylaxis [3] . However, a previous history of lactation anaphylaxis has been reported to be a risk factor [4] .
So far only case reports have been recorded about the condition with no big studies done to make strong conclusions. Standard treatment of anaphylaxis with antihistamines, epinephrine and glucocorticoids has been reported to be effective [4] . Another method of treatment reported to have been effective in the treatment of breastfeeding anaphylaxis was the suppression of breastmilk production with bromocriptine [4] . Prophylaxis with oral antihistamines before lactation has also been reported to be beneficial for the prevention of lactation anaphylaxis [3] .
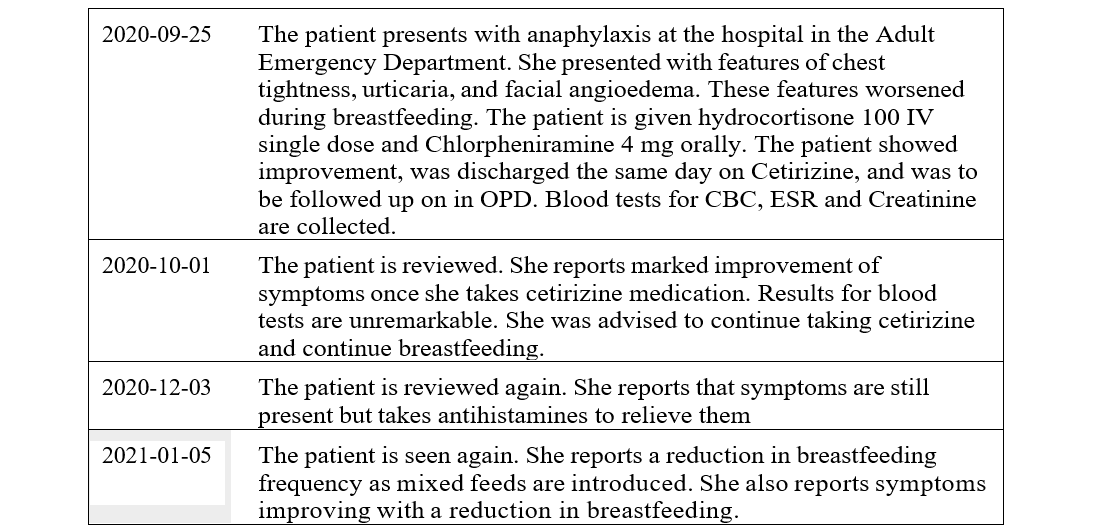
TIMELINE
NARRATIVE
A 31-year-old para 3 woman presented at Chipata Central Hospital in Zambia with features of anaphylaxis 4 days after giving birth to her third child. She presented at the hospital's AED unit with respiratory symptoms of difficulties in breathing and chest tightness. She also reported having generalized itching. She was noted to have urticaria, and facial angioedema which was more pronounced around the lips. In AED, she was treated with a single dose of hydrocortisone 100mg intravenous slowly and chlorpheniramine 4mg orally. She responded well to this initial treatment and was later referred to the Obstetrics and Gynaecology Unit on the same day for further management. She reported that her symptoms would start with general body itching and hotness before the appearance of hives. These symptoms would appear at any time of the day but were worse at night when she would breastfeed the most.
PREVIOUS HISTORY
The patient reported experiencing similar symptoms when breastfeeding her second child but not with her first child. The patient thought the itching was due to allergic reactions to lotions and baby products she was using. She frequently changed these products hoping she'd be fine, but the symptoms persisted. To relieve her symptoms, she used to take chlorpheniramine 2-4mg once daily, usually in the evening before going to sleep. Symptoms were also severe in the night when she breastfed the most. Her symptoms improved when breastfeeding frequency was reduced after introducing other baby foods at 6 months. The symptoms eventually disappeared a few weeks after she stopped breastfeeding.
The patient also reported an allergy to pork which she last ate 12 years ago at the time we were attending to her. She developed a rash after eating pork meat. The patient has never experienced any other forms of allergies.
TREATMENT
As earlier described, the patient received a single dose of dexamethasone 100mg given intravenous slowly together with oral chlorpheniramine 4mg in AED. We then changed the patient's antihistamine treatment from chlorpheniramine to oral cetirizine 10mg daily. We changed her to cetirizine because chlorpheniramine has sedative effects that could have affected her breastfeeding schedule. She took the cetirizine mainly in the evenings since her symptoms were usually worse at night when the baby breastfed the most.
The patient reported tolerating symptoms when taking cetirizine and therefore opted to breastfeed exclusively for the first six months. Symptoms further improved when she reduced the breastfeeding frequency when the baby was introduced to other feeds at six months. We did not prescribe further medicines. She eventually stopped taking cetirizine three weeks after cessation of breastfeeding. Her baby stopped breastfeeding at 17 months.
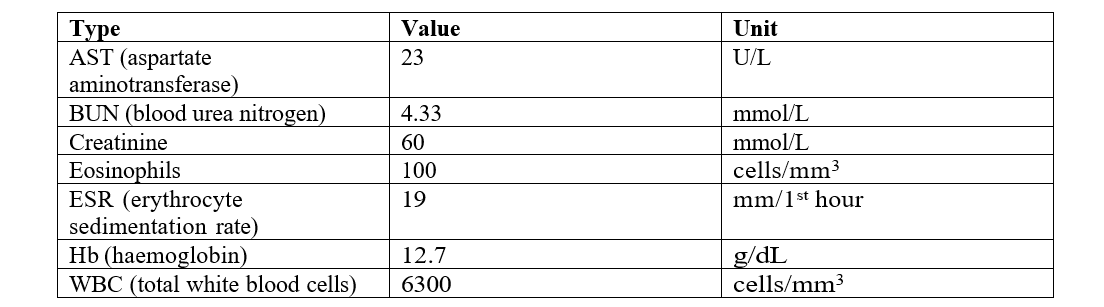
DIAGNOSTICS
DISCUSSION
There are few reported cases of lactation anaphylaxis worldwide. Women present with respiratory, gastrointestinal, and cardiovascular symptoms. Just like previously reported cases, our patient also had clinical features of urticaria, chest tightness, difficulties in breathing, and angioedema. We also noted that these symptoms started with her second child while reporting none with her first child, suggesting a possibility of a sensitisation process. Previously reported cases showed some patients developing lactation anaphylaxis with their first child while others reported onset with the second child.
Lactation anaphylaxis symptoms have been reported to be attributed to the changes in mast cell function due to hormonal changes occurring after delivery [2] . Falling levels of progesterone following delivery have been suggested as a possible cause of this mast cell dysfunction [3] .
Progesterone with other steroids stabilises mast cells during pregnancy [2] . There has also been a role of prolactin surge and oxytocin though the exact mechanisms have not been described [3] .
Lactation anaphylaxis symptoms can be life-threatening with patients reporting to the emergency department units. Lactation anaphylaxis requires a good history to diagnose [1] . As a result, some cases may be missed since many patients will present in the AEDs. It is therefore important that clinicians get a good history to diagnose it.
Women presenting with lactation anaphylaxis have been treated using standard treatment for anaphylaxis shock with antihistamines, epinephrine, and glucocorticoids to good effect [2] . Our patient was also treated with an initial dose of dexamethasone and chlorpheniramine before we switched her to cetirizine. She responded well to this treatment. Cessation of breastfeeding has also been shown to improve symptoms [4] . Like some previously reported cases, our patient also improved significantly on antihistamines which made it possible for her to continue breastfeeding. However, there are also reported cases where mothers had to completely stop breastfeeding to relieve their symptoms. The mother in one case report had to rely on donated milk [1] .
PATIENT PERSPECTIVE
The patient was generally happy with the outcome of her treatment. She expressed concerns about the possibility of the condition recurring and probably getting worse in future. She was happy to share her experience and therefore allowed us to publish her case for others to learn from.
CONCLUSION
Lactation anaphylaxis continues to be an extremely rare condition with this case being the first reported in Zambia. Patients can be treated with standard treatment for anaphylaxis such as the use of antihistamines and glucocorticoids. Cessation of breastfeeding results in the resolution of symptoms. With more case report publications and vigilant case finding, more cases could be identified. As more cases keep being unearthed, there's a need to conduct studies for clinicians to have a better understanding of the condition. Future research will also provide information for improved quality of care to the patients. Studies on the condition will also help provide data on its prevention for women at risk and help empower them with knowledge about their disease.
REFERENCES
- Knutson J, Youssef A. Supporting Families Facing Lactation Anaphylaxis: A Case Report. J Midwifery Women’s Health. 2023 Jul 5;68(4):531–4.
- Dharia T, Fadugba O. A Case of Recurrent Hives with Lactation. Annals of Allergy, Asthma & Immunology. 2022 Nov;129(5):S111.
- McKinney KK, Scranton SE. A case report of breastfeeding anaphylaxis: successful prophylaxis with oral antihistamines. Allergy. 2011 Mar;66(3):435–6.
- Durgakeri P, Jones B. A rare case of lactation anaphylaxis. Australas Med J. 2015;8(3):103–5.
- Shawkat E, Hussain N, Myers JE, Gillham J, Helbert M. Breast milk: friend or foe? Case Reports. 2011 Oct 28;2011(oct27 1):bcr0120113766–bcr0120113766.
- Pescatore R, Mekkaoui S, Duffell B, Riviello R. A Case of Lactation Anaphylaxis. Cureus. 2019 Aug 27;
- Shank JJ, Olney SC, Lin FL, McNamara MF. Recurrent Postpartum Anaphylaxis with Breast-Feeding. Obstetrics & Gynaecology. 2009 Aug;114(2):415–6.
Medical Journal of Zambia, Vol 51, 3
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.