Prevalence of Low Back Pain among Expectant Mothers Attending Antenatal Care at St. Francis Hospital in Katete District, Zambia
Eliness Lungu
Ministry of Health Zambia, St. Francis Mission Hospital, Katete Zambia
Fair Banji Mwiinga
Lusaka Apex Medical University, Lusaka Zambia
Lweendo Mapani
Lusaka Apex Medical University, Lusaka Zambia
Deborah Chileya
Lusaka Apex Medical University, Lusaka Zambia
Billiat Chongo
Lusaka Apex Medical University, Lusaka Zambia
Chilufya Muya
Lusaka Apex Medical University, Lusaka Zambia
DOI: https://doi.org/10.55320/mjz.51.3.546
Keywords:low back pain, prevalence, expectant mothers, attending antenatal care
ABSTRACT
Background: Low back pain (LBP) in pregnancy is a serious health concern that can range from acute pain to chronic pain, and can significantly decrease one’s quality of life and physical function, and increase financial impoverishment. However, there is scanty information on the prevalence of LBP among expectant mothers at St. Francis Mission Hospital in Eastern Zambia.
Objective: The aim of this study was to determine the prevalence of LBP among expectant mothers attending Antenatal Care services at St. Francis Mission Hospital.
Methods: A descriptive cross-sectional study design was adopted using quantitative methods. The study was conducted among 150 random expectant mothers attending Antenatal Care services at St. Francis Mission Hospital. Data were collected using a researcher-administered questionnaire adapted from the Oswestry Low Back Pain Disability Questionnaire. Using SPSS v27.0, descriptive statistical analysis was done in terms of numerical measures of central tendency and variability.
Results: One-hundred and fifty expectant mothers were successfully recruited. One-third of the participants were aged 18-25years; 65% were married; and 50% were self-employed. Seventy-three percent were 27-42 weeks pregnant; 86.7% were multiparous while 13.3% were primiparous. Forty percent had gained 5-10kg during pregnancy. Prevalence of LBP was found to be 86.7%. While 50% of the LBP cases started in the second trimester, 53.3% of the participants experienced more severe LBP in the third trimester. Based on the visual analogue scale, 46% of the participants had moderate pain which was intermittent. Functional limitations attributed to LBP were noted in lying, sitting, standing, walking and travelling.
Conclusion: Pregnancy-related LBP remains a serious public health problem. Therefore, there is need for healthcare providers to strengthen education programs, routine assessment and timely provision of targeted interventions in managing LBP among expectant mothers for improved quality of life.
INTRODUCTION
Low back pain is defined as pain, muscle tension, or stiffness localized below the coastal margin and above the inferior gluteal fold with or without leg pain.[1] Alnaami et al[2] . argue that low back pain is one of the most common complaints necessitating health care and also is the most frequently experienced type of musculoskeletal disorder. Pregnancy LBP has been found to be one of the most common musculoskeletal pains that most women experience for the first-time during pregnancy and may cause many problems and disabilities for them.[3] LBP in pregnancy can range from pain associated with specific activities to acute pain that becomes chronic, and can so severe that it can interfere with the ability to work or carry out normal activities, with a marked decrease in health-related quality of life and physical function; poor work performance; and increased economic financial burden from costs of health-care.[4] In addition, it has been ranked highest of the 291 conditions studied and accounted for 83 million disability-adjusted life years lost in 2010. [5]
Globally, LBP affects 40-80% of pregnant women[6] and 24-90% in sub-Saharan Africa. [7] A recent study conducted in Malawi by Manyozo et al.[7] revealed that at least 2 in every 3 pregnant women reported back pain. Another study that was done in 2018 reported that in Ethiopia, at least one-third of pregnant women had pregnancy-related LBP in Ethiopia.[8] In Zambia, the percentage of pregnant women affected by LBP remains unclear.
Pregnancy-related LBP can be attributed to a combination of mechanical, hormonal, systemic, and psychosocial factors such as scoliosis, spondylolisthesis, spinal stenosis, leg lengthy inequality, joint hypermobility and other postural abnormalities, osteoporosis, muscle imbalance, renal pathology, and overuse.[9,10] Davenport et al.[11] note that women who have experienced pregnancy-related backache are more likely to experience it in subsequent pregnancies. Management of LBP in pregnancy depends on the stage of pregnancy, underlying causes, aggravating factors, and the presence of co-morbidities. [12,13] Maintaining an optimal level of function throughout the pregnancy and having the least amount of discomfort are the main goals of treatment for pregnancy-related LBP, and interventions may include antenatal exercises for at least 150 min per week or 20–30 min of moderate to intense aerobic activity, postural correction, supported side-sleeping, lumbar roll while sitting, as well as limiting standing and walking.[11,14]
Despite evidence of the efficacy of various physiotherapy interventions for preventing and managing LBP among expectant mothers, gestational LBP remains a public health concern to this day. While several studies in various settings globally and in sub-Saharan Africa have reported and documented the prevalence and determinants of LBP, scanty studies have documented the pattern of pregnancy-related LBP, especially in Zambia. In Katete District of Eastern Zambia, very little is known regarding the prevalence of LBP among expectant mothers attending Antenatal care in Katete District—hence the need for this study.
METHODS
Study design:
This was a descriptive cross-sectional study design utilizing quantitative methods.
Study site:
Study was conducted at St. Francis Mission Hospital in Katete District of the Eastern Province of Zambia. St Francis Mission Hospital is a 450-bed third level Hospital offering services in General medicine, Surgery, Paediatrics, Obstetrics and Gynaecology, Physiotherapy, Radiology, Dentistry, and Ophthalmology. This setting was selected as it is the only hospital in Katete District and therefore carters for a larger population that extends as far as Mozambique.
Study population:
The study population included pregnant women of childbearing age attending Antenatal Care services at St. Francis Mission Hospital between June and December 2023. the months of August and September 2023. At the time of data collection, there were 240 expectant mothers who met the inclusion criteria. Expectant mothers below the legal age of consent, i.e. 16 years, were excluded from the study along with those Who had a history of backache prior to pregnancy and those with back pain attributed to other factors such as trauma or infection.
Sample selection:
Simple random sampling was used to select study participants using hospital attendance registers as the sampling frame. This method was appropriate to ensure a fair representation of expectant mothers, and to minimize selection bias.
Sample size:
A sample size of 150 expectant mothers was determined using the Yamane formula as follows: n = N/[1+N(e)2]. Where: n is the required sample size; N is the total population=240 expectant mothers (based on facility records, on average 20 expectant mothers are commenced on ANC per month at St Francis Mission Hospital, giving an annual estimate of 240); and e is the margin of error=0.05 at 95% confidence level. Substituting: n = 240/[1+240(0.05)2] n = 150. Therefore, n = 150expectant mothers
Data collection:
Data were collected using a researcher-administered structured questionnaire adapted from the Oswestry Low Back Pain Disability Questionnaire.[15] The questionnaire consisted of three sections as follows: Section A collected sociodemographic data such as age, weight gained during pregnancy, marital status and occupation of the expectant mother; Section B sought obstetric information such as the trimester of pregnancy, number of past pregnancies, and presence/absence of LBP in previous pregnancies; Section C collected information about LBP such as the trimester of onset, trimester when back pain was most severe, functional limitations due to LBP, and pain-easing modalities. The following specific sections were adapted from the Oswestry Low Back Pain Disability Questionnaire to measure functional limitations of LBP in Section C of our study: section 1 (pain intensity), section 3 (limitations of LBP on lifting), section 4 (limitations of LBP on walking), section 5 (limitations of LBP on sitting), section 6 (limitations of LBP on standing), section 7 (limitations of LBP on sleeping), and section 10 (limitations of LBP on travel).
In this study, validity was achieved by adapting and using the Oswestry Low Back Pain Disability Questionnaire, a validated tool with a Cronbach alpha coefficient of 0.87 ,[16] which is considered good. To ensure reliability, the data collection tool was pre-tested in a pilot study conducted on 5 randomly selected expectant mothers attending ANC at Chibolya Clinic, Katete District. Following the pilot study, changes were made to the questionnaire by removing some questions on sociodemographic characteristics such as age and occupation of participant’s spouse as these were deemed irrelevant for the study.
Data management and analysis:
Submitted questionnaires were checked for completeness and stored securely in a box file to which only the researcher had access. Collected data were sorted; coded; entered into the Statistical Package for Social Sciences (SPSS) v27.0 for Windows. The data were stratified and analysed based on the sections of the data collection tool and study variables. Using SPSS, descriptive statistical analysis was performed. Descriptive statistics included numerical measures such as mean, median, mode and standard deviation. These statistical operations were useful to demonstrate the central tendency and dispersion of the data, in line with the descriptive study design. No inference was done as that was outside the scope of the study. Results were summarized as frequencies and percentages and presented in form of tables and charts.
RESULTS
One hundred and fifty expectant mothers were successfully recruited and interviewed using a researcher-administered questionnaire, representing a response rate of 100%. The findings of this study have been presented in the form of frequency tables and charts for ease of interpretation as follows:
Sociodemographic characteristics
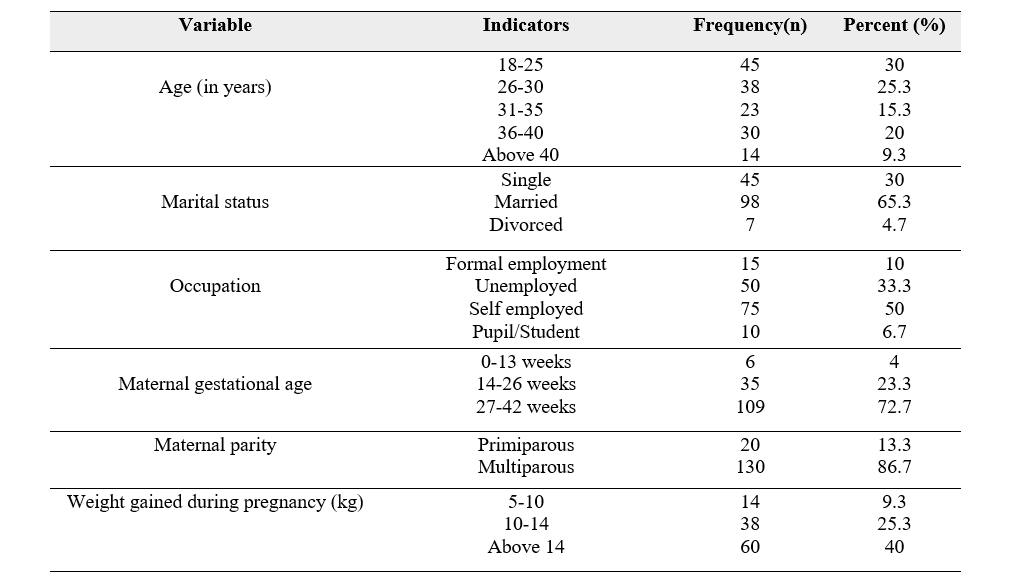
The age of participants ranged from 18 to 45 years, with highest proportion being in the age group 18-25years (30%, n=45). Sixty-five percent of the participants (n=95) were married, 30% (n=45) were single while 4.7% were divorced. The study further established that half of the participants (n=75) were self-employed and only 10% (n=15) were in formal employment. Seventy-three percent of the participants (n=109) were 27-42 weeks pregnant at the time of the study; 23.3% (n=35) were 14-26 weeks pregnant; and only 4% (n=6) had gestational age of 13 weeks and below. Cumulatively, 86.7% of the participants (n=130) were multiparous while 13.3% (n=20) were primiparous. In terms of pregnancy-related weight gain, the majority of the participants (40%, n=60) gained between 5 and 10 kilograms. Other demographic characteristics of the participants is summarized in Table 1 below:
Participants’ LBP characteristics
Majority of the participants reported having had experienced pregnancy-related LBP four or more times in the past while 13.3% did not have any experience of LBP. Of those who experienced pregnancy-related LBP, the majority (50%) experienced it during second trimester as compared to 35% who experienced it during third trimester, and 15% who experienced it during first trimester. In terms of the intensity of LBP, 46% of the participants reported having moderate LBP; 27% had no pain at all; 17.3 % were in mild pain; and 9.3% reported severe pain. Seventy percent of the participants reported having experienced LBP of intermittent nature while 30% reported having experienced continuous LBP, as summarized in Table 2 below:

Functional limitations caused by LBP
Study participants reported some of the functional limitations they experienced as a result of pregnancy-related LBP. These are summarized in Table 3 below:

Modalities used to ease LBP
Majority of the participants (47%) were taking analgesics (paracetamol); 40% used exercises; and 13% used rest as mode of easing their pregnancy-related LBP:

DISCUSSION
While a number of interventions have been put in place to avert the risk of LBP, pregnant women are still at risk. Determining the prevalence and patterns of pregnancy-related LBP is an important step in the formulation and/or strengthening of preventive strategies for mitigating the impact of LBP. The aim of this study was to determine the prevalence of LBP among expectant mothers attending antenatal care at St. Francis Hospital in Eastern Zambia. Below is a discussion of the findings:
Eighty-seven percent of the expectant mothers in our study reported to have experienced LBP. This finding is in line with previous studies that have reported pregnancy-related LBP prevalence of 68.5 – 90% [17,18] . However, much lower LBP prevalence rates have been reported as 76.8% in Lahore[19] ; 73% in Norway; 64% in central Portugal; and 68% in Brazil [20] . These discrepancies could be attributed to the variations in the study settings, study periods and demographic characteristics of the study participants. Our finding highlights the need to strengthen the inclusion of Physiotherapy services in antenatal care to enhance the prevention, screening for, and early management of LBP among expectant mothers.
Forty percent of our participants reported having had gained more than 14 kilograms of body weight during pregnancy. Empirical evidence has shown that weight gain during pregnancy is essential to support the growth of the foetus, and is usually between 11 and 15 kilograms. This additional load in the mother and the weight of the growing baby add to the pressure on the blood vessels and nerves located in the back and pelvic region, which has a higher prevalence of back pain in the third trimester than in the second and first [21,22] .
This study found that LBP onset was around the second trimester. Several studies have consistently reported that LBP typically begins in the second trimester[16,17,23] . The onset of LBP in the second trimester could be explained by the significant changes that occur in the musculoskeletal system such as changes in spinal flexibility, spinal joint stress, increased spinal load from the growing foetus, and exaggerated lordosis [24] . The clinical implication of this trend is that starting around the second trimester, LBP can lead to significant functional limitation, and compromise a pregnant woman’s ability to perform activities of daily living, such as sitting, standing, walking, sitting, and engaging in travel or chores, which could significantly affect her quality of life. Therefore, there is need for consistent education and sensitization about back care in pregnancy, prevention of LBP, as well as prompt management of LBP among expectant mothers.
The majority of our participants reported experiencing more severe LBP in the third trimester. This finding resonates with that reported by Szymański et al[25] . who found that LBP worsened with increasing gestational age, that is, pregnant women were likely to experience LBP in their second trimester, and experience the most severe LBP in the third trimester due to high spinal loading as maternal weight increases in late stages of pregnancy.
Forty-six percent of the participants who experienced LBP during pregnancy reported that they had moderate pain based on the Visual Analogue Scale. This is similar to findings of a related US study where the majority of the 645 surveyed pregnant women also reported moderate pain severity [26] . Due to the seriousness of pregnancy-related LBP, expectant mothers should be discouraged from believing that LPB is a normal and inevitable part of pregnancy for which it is not necessary to seek medical attention.
We found a number of functional limitations caused by pregnancy-related LBP such as sleeping, sitting, standing, walking, strenuous work and travelling. Similarly, Cheema et al.[17] found a number of limitations and concluded that LBP in pregnant women was aggravated by standing and relieved by resting. The implication of this finding is that it highlights the reduction in the quality of life, as well as the reduction in productivity among pregnant women as a result of LBP. These limitations, if unattended to, are likely to lead to inactivity and its associated musculoskeletal complications.
Over half of the participants in this study had experienced LBP in past pregnancies. Other studies have concluded that pregnant women who had a history of back pain in a previous pregnancy are 2.54 times more likely to have back pain in their subsequent pregnancy than those who do not[27,28] . Additionally, in a Japanese study, Skaggs et al.[20] concluded that back pain during pregnancy is not related to back pain before pregnancy but is related to back pain during menstruation and pregnancy.
The pregnancy-related LBP in 47% of the participants was managed with exercise therapy, while others used analgesics and rest. In line with our finding, a Malawian study by Manyozo et al.[7] also found that the majority of pregnant women resorted to LBP self-management through the exercises, stretching, massage, and self-prescribed analgesics. On the contrary, Kinser et al [29] . noted that pregnant women did not any medical intervention for their LBP because they perceived it as a normal and unavoidable part of pregnancy. The use of non-pharmacological interventions such as soft tissue manipulation, postural education, hydrotherapy, and stabilization exercises, often provided by physiotherapists, have been found to be effective in managing LBP during pregnancy and has since been recommended as first line of management for the treatment of LBP in pregnancy[7] . In fact, the adverse health risks that come with the use of analgesics in pregnancy are well documented, and the management of LBP with drugs during pregnancy has been unsatisfactory. For example, Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) are contraindicated in the third trimester of pregnancy while opiate drugs are considered unsafe throughout pregnancy[30] . This finding emphasizes the need to strengthen the routine incorporation of guidance and referrals to physiotherapy as part of antenatal care to address effectively persistent symptoms of LBP, and to minimize excessive intake of pain medications which could have significant adverse effects on both the mother and the developing foetus.
CONCLUSION
At 86.7%, pregnancy-related LBP poses a serious public health problem which significantly compromises one’s functional independence. This study also identified a number of precipitating factors for pregnancy-related LBP including sitting, standing, walking and traveling. In order to minimize risk for pregnancy-related LBP, there is need for healthcare providers to strengthen education programs, routine assessment and timely provision of targeted interventions in managing LBP among expectant mothers which could lead to improved quality of life and reduction of the LBP problem in pregnant women.
What is already known on this topic:
1. Prevalence of low back pain in the general population 2. Risk factors for low back pain in the general population
What this study adds:
1. This study highlights the need to continuously provide health education and improve ergonomic patterns among expectant mothers to minimize the risk and burden of low back pain, and reduce morbidity related to low back pain among expectant mothers 2. This study also adds to the body of knowledge on the prevalence of low back pain among expectant mothers in Katete District, Eastern Zambia
STUDY LIMITATIONS
This study was hospital-based and as such, the prevalence reported may not necessarily be generalizable to the general population in this catchment area.
RECOMMENDATIONS
The study makes the following recommendations:
1. There is need to strengthen the inclusion of physiotherapy in antennal care services at St. Francis Hospital for prompt assessment and management of pregnancy-related LBP and subsequently reduce pharmacological prescription burden 2. Health care providers at St Francis Hospital are encouraged to step up their patient education programs and nutritional counselling during antenatal care visits as these have been demonstrated to influence LBP in pregnancy. In addition, pregnant women should be advised to promptly seek medical attention as soon as they experience LBP to prevent further complications that may arise 3. The study recommends that more studies be undertaken, especially analytical studies to determine factors associated with LBP among expectant mothers at St Francis Hospital
DECLARATIONS
Ethics approval
Ethics approval for the study was granted by the Lusaka Apex Medical University Bio-medical Research Ethics Committee (FWA 00029892, IRB 00001131, Ref 00546-23). Signed consent was obtained from willing eligible participants after explaining to them the purpose of the study. All study participants were treated with utmost respect and privacy during data collection. Anonymity was upheld by ensuring that all study data collected did not have any identifying remarks, and codes were used to identify participants instead of names. Collected data was kept confidential on an encrypted drive which was accessible only to the researchers and for purposes limited to the scope of this study.
Acknowledgements
The contribution of all who made this undertaking possible is acknowledged as follows: Management, staff and expectant mothers at St. Francis Mission Hospital in Eastern Province, Zambia, as well as Faculty members at the Lusaka Apex Medical University.
Conflicts of interest
Authors declared that they have no conflicts of interest
Competing interests
Authors declared that they have no competing interests
Funding statement
No external funding was received for the study
Authors’ contributions
Eliness Lungu – principal investigator, drafting discussion section of manuscript Fair Banji Mwiinga – research supervisor, data analysis, overall editing of manuscript Lweendo Mapani – research co-supervisor, drafting methodology of manuscript Deborah Chileya – proof-reading of manuscript Chilufya Muya – review and editing of manuscript
REFERENCES
- Doualla M, Aminde J, Aminde LN, Lekpa FK, Kwedi FM, Yenshu EV, Chichom AM. Factors influencing disability in patients with chronic low back pain attending a tertiary hospital in sub-Saharan Africa. BMC Musculoskelet Disord. 2019;20(25):1-9. doi:10.1186/s12891-019-2403-9.
- Alnaami I, Awadalla NJ, Alkhairy M, Alburidy S, Alqarni A, Algarni A, Alshehri R, Amrah B, Alasmari M, Mahfouz AA. Prevalence and factors associated with low back pain among health care workers in southwestern Saudi Arabia. BMC Musculoskelet Disord. 2019;20(1):1-7. doi:10.1186/s12891-019-2431-5.
- Citko A, Górski S, Marcinowicz L, Górska A. Sedentary lifestyle and non-specific low back pain in medical personnel in North-East Poland. Biomed Res Int. 2018; (1). doi:10.1155/2018/1965807.
- World Health Organization. Low back pain [Internet]. World Health Organization. 2023 [Updated 2023; cited 2024 May 14]. Available from: https://www.who.int/news-room/fact-sheets/detail/low-back-pain
- Ravindra VM, Senglaub SS, Rattani A, Dewan MC, Härtl R, Bisson E, Park KB, Shrime MG. Degenerative lumbar spine disease: estimating global incidence and worldwide volume. Global Spine J. 2018;8(8):784-94. doi:10.1177/2192568218770769
- Shijagumayuma Acharya R, Tveter A, Grotle M, Eberhard-Gran M, Stuge B. Prevalence and severity of low back-and pelvic girdle pain in pregnant Nepalese women. BMC Pregnancy Childbirth. 2019; 19(1): 247. doi:10.1186/s12884-019-2398-0. PMID: 31307421.
- Manyozo S. Low back pain during pregnancy: Prevalence, risk factors and association with daily activities among pregnant women in urban Blantyre, Malawi. Malawi Med J. 2019;31(1):71-6. doi:10.4314/mmj.v31i1.12
- Abebe E, Singh K, Adefires M, Abraha M. History of low back pain during previous pregnancy had an effect on development of low back pain in current pregnancy attending antenatal care clinic of the University of Gondar Hospital, Northwest Ethiopia. Jour of Med Sc & Tech. 2014;3(3). 37-44
- Szatko A, Kacperczyk-Bartnik J, Bartnik P, Mabiala E, Goryszewska M, Dobrowolska-Redo A, Romejko-Wolniewicz E. Physical activity during pregnancy—the state of Polish women’s knowledge. Ginekol Pol. 2021;92(11):804-11. doi:10.5603/GP.a2021.0050
- Mottola MF, Nagpal TS, Bgeginski R, Davenport MH, Poitras VJ, Gray CE, Davies GA, Adamo KB, Slater LG, Barrowman N, Barakat R. Is supine exercise associated with adverse maternal and fetal outcomes? A systematic review. Br J Sports Med. 2019;53(2):82-9. doi:10.1136/bjsports-2018-099919.
- Davenport HM, Marchand AA, Mottola MF, Poitras VJ, Gray CE, Garcia AJ, Barrowman N, Sobierajski F, James M, Meah VL, Skow RJ, Riske L, Nuspl M, Nagpal TS, Courbalay A, Slater LG, Adamo BK, Davies GA, Barakat R, Ruchat SM. Exercise for the prevention and treatment of low back, pelvic girdle and lumbopelvic pain during pregnancy: a systematic review and meta-analysis. Br J Sports Med 2019;53(2):90–98. doi:10.1136/bjsports-2018-099400
- Al-Hadidi F, Bsisu I, Haddad B, AlRyalat SA, Shaban M, Matani N, et al. The prevalence of low back pain among female hospital staff at childbearing age. Peer J. 2020;8:e9199.
- Rabiee M, Sarchamie N. Low back pain severity and related disability in different trimesters of pregnancy and risk factors. Int J Women’s Health Reprod Sci. 2018;4:438–43
- Ceprnja D, Chipchase L, Fahey P, Liamputtong P, Gupta A. Prevalence and factors associated with pelvic girdle pain during pregnancy in Australian women: a cross-sectional study. Spine. 2021;46(14):944-9. doi:10.1097/BRS.0000000000003954.
- Fairbank J, Pynsent P. The Oswestry Disability Index. Spine. 2000;25(22):2940-2953.
- Tan K, Zheng M, Yang BX, Ernest V, Liu H, He J, Jiang M, Li XS. Validating the Oswestry Disability Index in patients with low back pain in Sichuan. Sichuan Da Xue Xue Bao Yi Xue Ban. 2009;40(3):559-61. PMID: 19627029.
- Fatmarizka T, Ramadanty RS, Khasanah DA. Pregnancy-related low back pain and the quality of life among pregnant women: a narrative literature review. J Pub Health Trop Coastal Region. 2021;4(3):108-16. doi:10.14710/jphtcr.v4i3.10795.
- Hall H, Cramer H, Sundberg T, Ward L, Adams J, Moore C, Sibbritt D, Lauche R. The effectiveness of complementary manual therapies for pregnancy-related back and pelvic pain: A systematic review with meta-analysis. Medicine. 2016;95(38):e4723. doi:10.1097/MD.0000000000004723
- Cheema ZR, Akhtar MW, Alam MM, Saeed S, Burhan M, Rizwan M. Prevalence of Low Back Pain in Pregnant Females. J Health and Rehabil Res. 2024;4(2):291-5. doi:10.61919/jhrr.v4i2.775
- Gutke A, Boissonnault J, Brook G, Stuge B. The Severity and Impact of Pelvic Girdle Pain and Low-Back Pain in Pregnancy: A Multinational Study. J Women's Health. 2018;27(4):510-7. doi:10.1089/jwh.2017.6342
- Malmqvist S, Kjaermann I, Andersen K, Økland I, Brønnick K, Larsen JP. Prevalence of low back and pelvic pain during pregnancy in a Norwegian population. J Manipulative Physiol Ther. 2012;35(4):272–8. doi:10.1016/j.jmpt.2012.04.004
- Skaggs CD, Prather H, Gross G, George JW, Thompson PA, Nelson DM. Back and pelvic pain in an underserved United States pregnant population: a preliminary descriptive survey. J Manipul Physiol Ther. 2007;30(2):130–4. doi:10.1016/j.jmpt.2006.12.008
- Fontana-Carvalho A, Dufresne SS, Oliveira MR, Furlanetto KC, Dubois M, Dallaire M. Effects of lumbar stabilization and muscular stretching on pain, disabilities, postural control and muscle activation in pregnant woman with low back pain. Eur J Phys Rehabil Med. 2020;56(3):297-306. doi:10.23736/S1973-9087.20.06086-4
- Otero-Ketterer E, Peñacoba-Puente C, Ferreira Pinheiro-Araujo C, Valera-Calero JA, Ortega-Santiago R. Biopsychosocial Factors for Chronicity in Individuals with Non-Specific Low Back Pain: An Umbrella Review. Int J Environ Res Public Health. 2022;16;19(16):10145. doi:10.3390/ijerph191610145
- Szymański, J., Słabuszewska-Jóźwiak, A. & Jakiel, G. Sacral Neuromodulation in Pregnant Women-A Case Report and Literature Review. Int J Environ Res Public Health. 2022, 19, 8340. doi:10.3390/ijerph19148340
- Parveen U, Brohi ZP, Sadaf A. Frequency of Backache and Its Management in Pregnant Women Attending IUH OPD. Pakistan J Med Health Sci. 2021. 28(68.9):15-16. doi:10.53350/pjmhs2115113441.
- Salari N, Mohammadi A, Hemmati M, Hasheminezhad R, Kani S, Shohaimi S and Mohammadi M. The global prevalence of low back pain in pregnancy: a comprehensive systematic review and meta-analysis. BMC Pregnancy Childbirth. 2023;23(1)830. doi:10.1186/s12884-023-06151-x
- Tavares P, Barrett J, Hogg-Johnson S, Ho S, Corso M, Batley S, et al. Prevalence of low back pain, pelvic girdle pain, and combination pain in a postpartum Ontario population. J Obstet Gynaecol Canada. 2020;42(4):473-80. doi:10.1016/j.jogc.2019.08.030
- Kinser PA, Pauli J, Jallo N, Shall M, Karst K, Hoekstra M, et al. Physical Activity and Yoga-Based Approaches for Pregnancy-Related Low Back and Pelvic Pain. J Obstet Gynecol Neonatal Nurs. 2017;46(3):334-46. doi:10.1016/j.jogn.2016.12.006
- Gorginzadeh M, Imani F, Safari S. Pregnancy-Related Pelvic Pain: A Neglected Field in Developing Countries. Anesth Pain Med. 2016;6(1):e35506. doi: 10.5812/aapm.35506
Medical Journal of Zambia, Vol 51, 3
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.