Mechanisms of Pseudobulbar Palsy in Artery of Percheron Infarction: Literature Study
Rita Komalasari
Yarsi University, Indonesia
DOI: https://doi.org/10.55320/mjz.51.2.515
Keywords:acute pseudobulbar palsy, artery of Percheron, infarction, neuroimaging, pathophysiology
ABSTRACT
Introduction: Acute pseudobulbar palsy (PBP) arising from infarction of the artery of Percheron (AOP) presents a challenging clinical scenario, with limited understanding of the underlying mechanisms.
Purpose: This essay aims to explore the mechanisms underlying PBP in the context of AOP infarction, addressing existing gaps in the literature and highlighting the potential for enhanced diagnostic and therapeutic strategies.
Methodology: Through a comprehensive review of existing neuroimaging studies, this essay synthesizes data to provide insights into the pathophysiological cascade driving PBP in AOP infarction.
Conclusion: By integrating clinical observations with neuroimaging findings and experimental data, the essay offers a deeper understanding of the structural and functional alterations underlying PBP in AOP infarction. This integrated approach elucidates the specific neural circuits affected by AOP infarction, paving the way for enhanced diagnostic and therapeutic strategies tailored to this unique vascular territory. Overall, this research contributes to bridging existing gaps in the literature and underscores the importance of further investigation into the mechanisms of PBP in AOP infarction for improved patient care and outcomes.
INTRODUCTION
Acute pseudobulbar palsy (PBP) presents a challenging clinical scenario, particularly when it arises from infarction of the artery of Percheron (AOP).[1] This unique manifestation underscores the intricate relationship between vascular anatomy and neurological function.[2] While clinical observations have hinted at a correlation between AOP infarction and isolated PBP, the underlying mechanisms remain elusive.[3] This paper seeks to explore the intricacies of PBP in relation to AOP infarction, highlighting the need for more study to fully understand the complex interactions between neuroanatomy and disease. The human brain, an intricate network of billions of neurons, is remarkably susceptible to disruptions in blood flow. One such disruption, an infarction in the artery of Percheron (AOP), can have devastating consequences, impacting vital functions like movement, cognition, and even emotional expression.[4] Among these, the emergence of acute pseudobulbar palsy (PBP) following AOP infarction presents a unique and intriguing challenge.[5] While a recent case report hints at a possible connection, the precise mechanisms underlying this association remain shrouded in mystery. This essay embarks on a journey to illuminate this enigmatic association.[6] The author starts by exploring the complex anatomical structure of the brain, emphasizing the vital function of the AOP and its susceptible areas. Next, we shed light on the debilitating symptoms of PBP, characterized by uncontrollable emotional outbursts and speech difficulties. The heart of this exploration lies in dissecting the potential links between AOP infarction and PBP. We critically examine the existing evidence, acknowledging both the suggestive case report and the need for further investigation. Drawing upon the latest advancements in neuroimaging, we propose avenues for future research. By exploring connectivity disruptions and functional changes within the corticobulbar pathway, we aim to unlock the secrets hidden within the brain's response to AOP infarction. This research endeavour has the capacity to further our comprehension of this intricate connection and open the door to more accurate diagnosis, effective treatment, and eventually, hope for those dealing with this difficult illness. Throughout this exploration, we will weave together insights from diverse fields, including neuroanatomy, stroke medicine, and emotional neuroscience. By critically analysing current knowledge and proposing future directions, we aim to bridge the gap between clinical observation and a deeper understanding of the mechanisms at play. Join us as we embark on this intellectual journey, one step closer to unravelling the fascinating puzzle of acute pseudobulbar palsy and artery of Percheron infarction.
A comprehensive literature study was conducted to gather evidence and insights into the mechanisms of pseudobulbar palsy (PBP) secondary to artery of Percheron (AOP) infarction. This involved systematic review and analysis of peer-reviewed articles, clinical case reports, and neuroimaging studies pertaining to PBP, AOP anatomy, and vascular neurology. In order to find patterns, trends, and gaps in the body of literature already in existence, data analysis required combining information from several sources. A comprehensive knowledge of the pathophysiological processes behind PBP in AOP infarction was made possible by the integration of data from clinical observations, neuroimaging investigations, and experimental models. To conduct a comprehensive literature study on the mechanisms of pseudobulbar palsy (PBP) secondary to artery of Percheron (AOP) infarction, a systematic approach was adopted involving the following components:
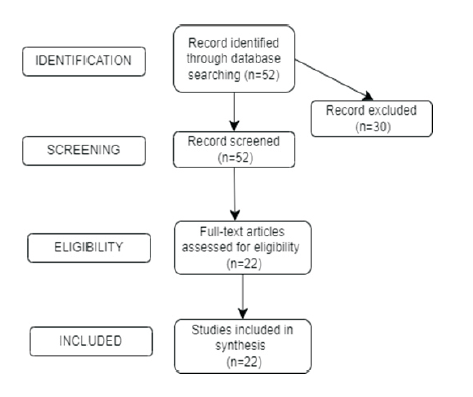
Search Strategies: A combination of keywords related to pseudobulbar palsy, artery of Percheron infarction, neuroimaging, vascular neurology, and related terms were used. Databases such as Google Scholar were searched. Search filters were applied to limit results to peer-reviewed articles, clinical case reports, and neuroimaging studies.
Inclusion Criteria: Articles and studies were included if they addressed the relationship between pseudobulbar palsy and AOP infarction. Peer-reviewed articles, clinical case reports, and neuroimaging studies were considered for inclusion. Studies providing insights into the pathophysiological mechanisms underlying pseudobulbar palsy in the context of AOP infarction were prioritized. Both human and experimental animal studies were included to gather comprehensive insights. Exclusion Criteria: Articles not written in English were excluded. Studies not directly relevant to the topic or lacking substantial information were excluded. Publications without full-text availability or inaccessible resources were excluded.
Data Synthesis: Data synthesis involves collating information from various sources, including clinical observations, neuroimaging investigations, and experimental models. Key findings, trends, patterns, and gaps in the literature were identified through thorough analysis. Comparative analysis of clinical presentations, imaging findings, and pathophysiological mechanisms was conducted to elucidate the relationship between PBP and AOP infarction. The integration of data from diverse sources facilitated a comprehensive understanding of the pathophysiology of PBP in the context of AOP infarction. Synthesized data were organized and presented to provide insights into the mechanisms underlying PBP secondary to AOP infarction and to identify areas for further research.
By following these systematic procedures for search, inclusion/exclusion criteria, and data synthesis, the literature study aimed to provide a comprehensive understanding of the mechanisms underlying pseudobulbar palsy in the context of artery of Percheron infarction.
LITERATURE REVIEW
Role of the AOP in corticobulbar connectivity
Acute pseudobulbar palsy (PBP) is a multifaceted neurological condition characterized by bilateral upper motor neuron dysfunction affecting the bulbar muscles, resulting in symptoms such as dysarthria, dysphagia, and emotional lability.[7] This debilitating disorder often arises from various aetiologies, including vascular events such as infarction.
The artery of Percheron (AOP) represents a rare vascular variant originating from the posterior cerebral artery.[8] This arterial structure plays a crucial role in supplying blood to pivotal brain regions, including the bilateral thalami and portions of the midbrain. Consequently, infarction involving the AOP can precipitate a spectrum of neurological manifestations, ranging from altered consciousness to motor and sensory deficits.
Of particular relevance to PBP, the AOP supplies critical components of the corticobulbar pathway, facilitating communication between cortical motor areas and brainstem nuclei responsible for controlling bulbar musculature.[9] Thus, infarction of the AOP can disrupt these neural circuits, leading to the characteristic clinical features of PBP.
Understanding the intricate vascular anatomy and its implications for neurological function is paramount in deciphering the pathophysiological mechanisms underlying PBP secondary to AOP infarction. This introduction sets the stage for further exploration into the complexities surrounding this unique manifestation, emphasizing the pivotal role of the AOP in mediating corticobulbar connectivity and highlighting the need for a comprehensive understanding of this vascular territory in clinical practice and research.
Numerous clinical observations and case reports have contributed to our understanding of isolated pseudobulbar palsy (PBP) secondary to infarction of the artery of Percheron (AOP).[10] These documented cases often present with a distinct clinical profile characterized by acute-onset bulbar symptoms, including dysarthria and dysphagia, alongside signs indicative of bilateral upper motor neuron dysfunction.
Relationship between AOP infarction and corticobulbar dysfunction
Isolated pseudobulbar palsy (PBP) refers to a neurological condition characterized by dysfunction of the bulbar muscles, which are involved in functions such as speech, swallowing, and emotional expression.[11] PBP is termed "isolated" when it occurs without other significant neurological deficits. Infarction of the artery of Percheron (AOP) is a rare vascular event where a single artery supplies blood to critical brain regions, including bilateral thalami and parts of the midbrain.[8] When AOP infarction occurs, it can lead to diverse neurological manifestations, including PBP. In these cases, patients typically present with sudden onset of bulbar symptoms such as dysarthria (difficulty speaking) and dysphagia (difficulty swallowing), along with signs of bilateral upper motor neuron dysfunction. Notably, the absence of other focal neurological deficits distinguishes PBP secondary to AOP infarction from other causes of bulbar dysfunction. These cases underscore the importance of considering AOP infarction as a potential aetiology in patients presenting with isolated pseudobulbar symptoms.
Importantly, the hallmark of PBP secondary to AOP infarction is the absence of other focal neurological deficits typically associated with lesions in alternative vascular territories. This suggests a specific involvement of corticobulbar pathways supplied by the AOP, underscoring the unique clinical presentation observed in these cases. The specific involvement of corticobulbar pathways supplied by the artery of Percheron (AOP) refers to the disruption of neural circuits connecting cortical motor areas with brainstem nuclei responsible for controlling bulbar musculature. In cases where AOP infarction occurs, the compromised blood supply to critical brain regions, including the bilateral thalami and parts of the midbrain, can lead to dysfunction within these corticobulbar pathways.
Clinical observations and case reports have documented instances where patients present with isolated pseudobulbar palsy (PBP) secondary to AOP infarction.[12] These cases typically manifest as acute-onset bulbar symptoms, such as dysarthria and dysphagia, accompanied by signs indicative of bilateral upper motor neuron dysfunction. Notably, the absence of other focal neurological deficits suggests a specific involvement of corticobulbar pathways supplied by the AOP. Following an AOP infarction, neuroimaging studies employing methods like diffusion tensor imaging (DTI) and functional magnetic resonance imaging (fMRI) have shed more light on the structural and functional changes within these corticobulbar circuits. These results underline the crucial role that corticobulbar pathways provided by the AOP play in modulating bulbar function, and they support the concept that there is a direct association between the clinical signs of PBP and the anatomical distribution of infarction affecting the AOP. Overall, the occurrence of PBP secondary to AOP infarction underscores the specific involvement of corticobulbar pathways supplied by the AOP and highlights the importance of considering vascular anatomy in understanding the pathophysiology of bulbar dysfunction.
Milder Manifestations and Transient Symptoms
Clinical observations further highlight the variability in symptomatology and severity among individuals affected by PBP secondary to AOP infarction.[13] While some patients may present with profound bulbar symptoms leading to significant functional impairment, others may exhibit milder manifestations or transient symptoms, reflecting the diverse spectrum of neurological deficits associated with AOP infarction. When artery of Percheron (AOP) infarction causes pseudobulbar palsy (PBP), the extent and location of the infarct, individual differences in neuroplasticity and compensatory mechanisms, and underlying comorbidities all play a role in the variability of symptomatology and severity among affected individuals.
Clinical observations and case reports have highlighted the diverse spectrum of manifestations seen in patients with PBP secondary to AOP infarction.[14] While some individuals may present with profound bulbar symptoms, such as severe dysarthria and dysphagia leading to significant functional impairment, others may exhibit milder manifestations or transient symptoms. The variability in symptomatology can be attributed to the anatomical distribution of the infarct within the AOP territory. Infarcts involving different regions of the bilateral thalami and midbrain may result in varying degrees of disruption to corticobulbar pathways and associated neural circuits, leading to heterogeneous clinical presentations. Additionally, individual differences in neuroplasticity and compensatory mechanisms may influence the severity and course of symptoms in PBP secondary to AOP infarction. Some patients may exhibit greater capacity for neural adaptation and recovery, resulting in partial or transient symptoms, while others may experience more persistent deficits due to impaired compensatory mechanisms.
Milder manifestations or transient symptoms in cases of pseudobulbar palsy (PBP) secondary to artery of Percheron (AOP) infarction reflect the diverse spectrum of neurological deficits associated with this rare vascular event.[15] In some instances, patients may present with less severe bulbar symptoms, such as mild dysarthria or transient episodes of dysphagia, which may resolve spontaneously or with minimal intervention. These milder manifestations suggest partial involvement or temporary dysfunction of the corticobulbar pathways supplied by the AOP. Furthermore, transient symptoms may occur due to the presence of collateral circulation or compensatory mechanisms that help mitigate the effects of the infarct. Collateral blood supply from neighbouring arteries or recruitment of alternative neural pathways may temporarily sustain bulbar function, resulting in transient or fluctuating symptoms. Clinical observations and case reports have documented instances where patients with AOP infarction present with mild or transient symptoms, underscoring the variability in the clinical presentation of this condition.[15] While some individuals may experience profound and persistent deficits, others may exhibit milder manifestations that resolve over time. Overall, the occurrence of milder manifestations or transient symptoms in cases of PBP secondary to AOP infarction highlights the heterogeneous nature of neurological deficits associated with this rare vascular event. Comprehending the fluctuations in clinical manifestation is essential for precise diagnosis and suitable therapy of impacted persons. Furthermore, underlying comorbidities such as vascular risk factors, pre-existing neurological conditions, and concurrent injuries may exacerbate or modulate the clinical presentation of PBP in individuals with AOP infarction. The intricate interaction of structural, physiological, and individual elements in forming the clinical phenotype of PBP related to AOP infarction is highlighted by the overall diversity in symptomatology and severity across afflicted people.[16] Understanding these factors is essential for tailoring diagnostic and therapeutic strategies to the unique needs of each patient. Overall, the accumulation of clinical observations and case reports provides valuable insights into the distinct clinical features and natural history of PBP secondary to AOP infarction. These results emphasize how crucial it is to take AOP infarction into account when diagnosing patients with isolated pseudobulbar symptoms. This will help to inform treatment plans that are customized for this particular vascular region.
DISCUSSION
The pathophysiological mechanisms driving pseudobulbar palsy (PBP) in the context of artery of Percheron (AOP) infarction involve the disruption of corticobulbar pathways and associated neural circuits.[17] Advanced neuroimaging methods like functional magnetic resonance imaging (fMRI) and diffusion tensor imaging (DTI) have shed light on the structural and functional changes that underlie these phenomena. DTI studies have revealed microstructural changes in the corticobulbar tracts, indicating axonal injury or degeneration secondary to AOP infarction.[18] These alterations disrupt the integrity of the neural pathways connecting cortical motor areas to brainstem nuclei responsible for controlling bulbar musculature, thereby contributing to the development of PBP. Furthermore, fMRI studies have demonstrated functional changes in regions associated with motor control and speech production following AOP infarction. Disruptions in functional connectivity within the corticobulbar network are evident, reflecting the impaired coordination of motor commands necessary for bulbar function. Importantly, the findings from neuroimaging studies support a direct correlation between the anatomical distribution of infarction involving the AOP and the clinical manifestations of PBP. Regions supplied by the AOP, including the bilateral thalami and midbrain structures, exhibit structural and functional abnormalities that align with the observed bulbar symptoms in affected individuals. Overall, the integration of neuroimaging data with clinical observations provides compelling evidence for the role of corticobulbar pathway disruption in the pathogenesis of PBP secondary to AOP infarction. These findings underscore the importance of understanding the underlying mechanisms driving this condition, with implications for guiding diagnostic evaluations and developing targeted therapeutic interventions aimed at preserving corticobulbar function in affected individuals. Despite significant progress in elucidating the mechanisms of pseudobulbar palsy (PBP) in artery of Percheron (AOP) infarction, several challenges persist, warranting further investigation and exploration of future directions.[19]
One major challenge is the limited availability of experimental models that accurately simulate AOP infarction. The scarcity of robust animal models hampers our ability to validate hypothesized mechanisms and explore potential therapeutic interventions. Developing more sophisticated experimental models that closely mimic the anatomical and physiological characteristics of AOP infarction is essential for advancing our understanding of the pathophysiological processes underlying PBP. Furthermore, additional research is needed to unravel the precise pathophysiological cascade involved in PBP secondary to AOP infarction. Even while neuroimaging research has shed light on structural and functional changes, further work is needed to clarify the molecular and cellular processes behind these changes. Investigating the role of neuroinflammatory processes, secondary neurodegeneration, and other pathophysiological mechanisms in AOP infarction induced PBP could provide critical insights into potential therapeutic targets. Moreover, exploring the long-term consequences and outcomes of PBP in AOP infarction is essential for informing clinical management and prognostication. Longitudinal studies tracking the evolution of symptoms, functional outcomes, and quality of life in affected individuals can shed light on the natural history of the condition and identify factors influencing disease progression and recovery. Addressing these challenges and pursuing future research directions, including the development of experimental models, elucidation of pathophysiological mechanisms, and exploration of long-term outcomes, is crucial for advancing our understanding of PBP in the context of AOP infarction. These endeavours hold promise for informing diagnostic strategies, guiding therapeutic interventions, and improving patient outcomes in this unique vascular territory. The insights derived from understanding the mechanisms of pseudobulbar palsy (PBP) in artery of Percheron (AOP) infarction carry significant clinical implications, offering avenues for improved diagnostic strategies and targeted therapeutic interventions.[20] Improved diagnostic approaches, such as the application of cutting-edge neuroimaging methods like functional magnetic resonance imaging (fMRI) and diffusion tensor imaging (DTI), have the potential to enable early identification of PBP related to AOP infarction. By accurately delineating the structural and functional alterations within the corticobulbar pathways, neuroimaging can aid in the timely identification of patients at risk for PBP, enabling prompt interventions and improved patient outcomes.
Clarifying the pathophysiological cascade that underlies PBP in AOP infarction also offers chances for the creation of focused treatment therapies meant to maintain corticobulbar function and lessen impairment in those who are impacted. Pharmacological agents targeting neuroinflammatory processes, neuroprotective strategies aimed at preventing secondary neurodegeneration, and rehabilitative interventions focused on optimizing motor function and speech articulation represent potential avenues for therapeutic exploration. The integration of mechanistic insights into clinical practice holds promise for improving the management and prognosis of PBP secondary to AOP infarction. By leveraging advanced diagnostic modalities and targeted therapeutic interventions informed by our understanding of the underlying pathophysiology, clinicians can enhance patient care and outcomes in this unique vascular territory. Continued research efforts aimed at further elucidating the mechanisms driving PBP in AOP infarction are essential for advancing clinical practice and improving the quality of life for affected individuals. The evidence presented throughout this essay underscores the intricate interplay between vascular anatomy and neurological function in the context of pseudobulbar palsy (PBP) secondary to artery of Percheron (AOP) infarction. By integrating clinical observations, neuroimaging studies, and experimental models, a comprehensive understanding of the pathophysiological mechanisms driving this condition has been achieved. The convergence of clinical observations highlighting the distinct clinical profile of PBP secondary to AOP infarction, neuroimaging studies revealing structural and functional alterations within corticobulbar pathways, and experimental models providing insights into underlying pathophysiological processes collectively contributes to a deeper understanding of this complex neurological phenomenon. This multifaceted approach not only elucidates the mechanisms driving PBP in AOP infarction but also holds significant implications for clinical practice and patient care. Enhanced diagnostic strategies utilizing advanced neuroimaging techniques can facilitate early recognition of PBP, leading to timely interventions and improved patient outcomes. Moreover, the identification of targeted therapeutic interventions aimed at preserving corticobulbar function and mitigating disability in affected individuals underscores the potential for tailored management strategies informed by our mechanistic understanding of the condition.
While the current literature provides valuable insights into the role of the artery of Percheron (AOP) in corticobulbar connectivity and the clinical manifestations of pseudobulbar palsy (PBP) secondary to AOP infarction, several potential limitations should be acknowledged. Infarction involving the AOP can result in diverse patterns of neural injury, leading to heterogeneous clinical presentations. The variability in infarct size, location, and extent of involvement may confound the interpretation of findings and complicate efforts to establish consistent diagnostic criteria and treatment protocols. Despite efforts to elucidate the pathophysiological mechanisms underlying PBP secondary to AOP infarction, our understanding remains incomplete. The intricate interplay between vascular anatomy, neural pathways, and compensatory mechanisms is not fully elucidated, warranting further investigation using advanced neuroimaging techniques and experimental models. Conducting a comprehensive literature study requires significant time and resources to search, review, and synthesize a large volume of literature. Time constraints may limit the depth and breadth of the search, potentially overlooking relevant studies or emerging research in the field.
To further advance our comprehension of pseudobulbar palsy (PBP) secondary to the artery of Percheron (AOP) infarction and enhance outcomes for affected individuals, future research directions and specific clinical applications have been identified: elucidating the pathophysiological mechanisms underlying PBP secondary to AOP infarction is crucial. This entails investigating the specific neural pathways and neurotransmitter systems involved, as well as exploring the roles of neuroinflammation, neurovascular coupling, and neuroplasticity in modulating clinical progression and recovery trajectories.
CONCLUSION
To sum up, the combination of neuroimaging research, clinical observations, and experimental models has yielded important new understandings of the pathophysiological processes behind PBP resulting from AOP infarction. This comprehensive understanding not only enhances our knowledge of this unique vascular territory but also has significant implications for advancing clinical practice and optimizing patient care in affected individuals. Continued research efforts aimed at further elucidating the complexities of this condition are essential for improving diagnostic accuracy, refining therapeutic strategies, and ultimately improving outcomes for individuals affected by PBP secondary to AOP infarction.
REFERENCES
- Rissardo JP, Caprara AF. Isolated acute pseudobulbar palsy with infarction of artery of Percheron: case report and literature review. Afr Health Sci. 2021;21(1):166-71. https://doi.org/10.4314/ahs.v21i1.22
- Troili F, Cipollini V, Moci M, Morena E, Palotai M, Rinaldi V, et al. Perivascular unit: this must be the place. the anatomical crossroad between the immune, vascular and nervous system. Front Neuroanat. 2020;14:17. https://doi.org/10.3389/fnana.2020.00017
- Wardlaw JM, Benveniste H, Nedergaard M, Zlokovic BV, Mestre H, Lee H, et al. Perivascular spaces in the brain: anatomy, physiology and pathology. Nat Rev Neurol. 2020;16(3):137-53. https://doi.org/10.1038/s41582-020-0312-z
- Musa J, Rahman M, Guy A, Kola E, Guy A, Hyseni F, et al. Artery of Percheron infarction: a case report and literature review. Radiol Case Rep. 2021;16(6):1271-5. https://doi.org/10.1016/j.radcr.2021.02.059
- Ciurea AV, Mohan AG, Covache-Busuioc RA, Costin HP, Glavan LA, Corlatescu AD, et al. Unraveling Molecular and Genetic Insights into Neurodegenerative Diseases: Advances in Understanding Alzheimer's, Parkinson's, ALS, and Huntington's Disease. https://doi.org/10.20944/preprints202305.1229.v1
- Sami DG, Salama M. An Understanding of Different Mechanisms Leading to Neurodegenerative Diseases. In: Handbook of Neurodegenerative Disorders. Singapore: Springer Nature Singapore; 2023. p. 1-53. https://doi.org/10.1007/978-981-19-3949-5_10-1
- Warghane UM, Sharma R, Pohekar S, Warghane AJ. Case Report on Acute Cerebrovascular Episode with Pseudobulbar Palsy. https://doi.org/10.21203/rs.3.rs-2225270/v1
- Kheiralla OAM. Artery of Percheron infarction a rare anatomical variant and a diagnostic challenge: Case report. Radiol Case Rep. 2021;16(1):22-9. https://doi.org/10.1016/j.radcr.2020.10.032
- Chiang YK, Ling YH, Chang FC, Fuh JL. A clinical study of artery of Percheron infarction. J Chin Med Assoc. 2022;85(11):1098-100. https://doi.org/10.1097/JCMA.0000000000000769
- Macedo M, Reis D, Cerullo G, Florêncio A, Frias C, Aleluia L, et al. Stroke due to Percheron artery occlusion: description of a consecutive case series from southern Portugal. J Neurosci Rural Pract. 2022;13(1):151-4. https://doi.org/10.1055/s-0041-1741485
- Kwon N, Choi WI, Kim HS. Isolated Bilateral Cerebral Peduncular Infarction Manifesting Pseudobulbar Palsy and Quadriparesis: a Case Report. Brain Neurorehabil. 2020 Dec 2;14(2) doi: 10.12786/bn.2021.14.e16. PMID: 36743434; PMCID: PMC9879499.
- Morais J, Oliveira AA, Burmester I, Pires O. Artery of Percheron infarct: a diagnostic challenge. BMJ Case Rep. 2021;14(4). https://doi.org/10.1136/bcr-2020-236189
- Li J, Ge J, Yang S, Yao G. Clinical review and analysis of artery of Percheron infarction. IBRO Neurosci Rep. 2023. https://doi.org/10.1016/j.ibneur.2023.04.006
- Barilyak NL, Ponomarev GV, Shatsman IG, Zhukovskaya NV, Skoromets A. Artery of Percheron infarction of the brain: clinical case. J Clin Pract. 2020;11(3):114-9. https://doi.org/10.17816/clinpract41827
- Ranasinghe KMIU, Herath HMMTB, Dissanayake D, Seneviratne M. Artery of Percheron infarction presenting as nuclear third nerve palsy and transient loss of consciousness: a case report. BMC Neurol. 2020;20:1-5. https://doi.org/10.1186/s12883-020-01889-9
- Dec-Ćwiek M, Boczarska-Jedynak M, Pera J. An Unusual Presentation of Progressive Supranuclear Palsy. Neurol India. 2021;69(6):1789-93. https://doi.org/10.4103/0028-3886.333499
- Ashraf S, Allena N, Shrestha E, Dhallu M, Khaja M. Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy (CADASIL): A Rare Cause of Transient Ischemic Attack. Cureus. 2022;14(10). https://doi.org/10.7759/cureus.30940
- Olowoporoku IG, Digala LP, Attele DP, Olowoporoku I, Attele D. Central pontine myelinolysis: a case report of persistent hyperglycemia with normal serum sodium. Cureus. 2022;14(9). https://doi.org/10.7759/cureus.29470
- Jha NK, Chen WC, Kumar S, Dubey R, Tsai LW, Kar R, et al. Molecular mechanisms of developmental pathways in neurological disorders: A pharmacological and therapeutic review. Open Biol. 2022;12(3):210289. https://doi.org/10.1098/rsob.210289
- Alfonsi E, Todisco M, Fresia M, Tassorelli C, Cosentino G. Electrokinesiographic study of oropharyngeal swallowing in neurogenic dysphagia. Dysphagia. 2021;1-15. https://doi.org/10.1007/s00455-021-10336-x
- Feldman EL, Goutman SA, Petri S, Mazzini L, Savelieff MG, Shaw PJ, et al. Amyotrophic lateral sclerosis. Lancet. 2022;400(10360):1363-80. https://doi.org/10.1016/S0140-6736(22)01272-7
- Rawji V, Latorre A, Sharma N, Rothwell JC, Rocchi L. On the use of TMS to investigate the pathophysiology of neurodegenerative diseases. Front Neurol. 2020;11:584664. https://doi.org/10.3389/fneur.2020.584664
Medical Journal of Zambia, Vol 51, 2
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.