Exploring the perceptions and lived experiences of obstetric fistula among women of childbearing age: A qualitative inquiry at the University Teaching Hospital in Zambia
Loveness A. Nkhata
University of Zambia, School of Health Sciences, Department of physiotherapy, Lusaka-Zambia
Department of Health and Rehabilitation Sciences, Division of Physiotherapy, Stellenbosch University, Cape Town, South Africa
Jane M. Chela
University Teaching Hospital, Department of physiotherapy, Lusaka-Zambia
Kangwa M. Chileshe
University Teaching Hospital, Department of physiotherapy, Lusaka-Zambia
Margaret Phiri
Department of Physiotherapy, Kabwe Women New Born and Children's Hospital, Kabwe-Zambia
Margaret M. Mweshi
University of Zambia, School of Health Sciences, Department of physiotherapy, Lusaka-Zambia
DOI: https://doi.org/10.55320/mjz.51.2.514
Keywords:Perceptions, Experiences, Obstetric, Fistula, Women, Childbearing, Age
ABSTRACT
Background: Obstetric fistula, is a significant problem for women's health and rights. It primarily affects young women and perpetuates poverty and social vulnerability. Limited access to emergency obstetric care exacerbates the situation, hindering women to work or engage in community activities. This study aimed to explore the lived experiences and perceptions of obstetric fistula among women of childbearing age at the University Teaching Hospital in Zambia.
Methods: This was a qualitative study design and one-on-one interviews were used to explore how fistula affects women of childbearing age. The interviews were conducted in a private and comfortable setting to encourage open discussion. The data was transcribed and analysed for recurring patterns and themes using thematic analysis. The participants' responses were coded to capture the diverse experiences and perceptions related to fistula and outcomes were presented as narratives.
Results: The findings of our research indicate that women who are seeking treatment for obstetric fistula encounter significant challenges. The participants in our study emphasized the various ways in which fistula affects different stages of their reproductive life-cycle, highlighting the intricate relationship between medical and socio-economic factors.
Conclusion: Participants shared diverse experiences related to their lives with fistula, highlighting their views on its impact and the daily challenges of managing the condition. Their accounts reveal various difficulties associated with obstetric fistula, such as financial struggles, challenges in obtaining transportation, and a lack of available treatment options. To ensure comprehensive care and improve recovery and overall health for women impacted by this condition, it is crucial to incorporate targeted treatment approaches and foster collaboration among healthcare providers.
INTRODUCTION
Fistula impacts females across all age groups, occurring during both initial and subsequent pregnancies[1] . While once prevalent in Europe and America, advancements in healthcare and delayed marriage age have led to the eradication of the condition in these regions[2] . Nevertheless, research suggests that annually, a significant number of women ranging from 50,000 to 100,000 globally are impacted by obstetric fistula [3] . Obstetric fistula often occurs as a result of obstructed labour, causing damage to tissues and the formation of abnormal connections between the vagina and bladder/rectum. This can lead to urinary and/or faecal incontinence, and in severe cases, may result in maternal mortality[4,5] . Women afflicted by obstetric fistula endure persistent urinary or faecal incontinence, feelings of disgrace, social isolation, and various health complications[4] . Statistics indicate that over 2 million young women in Asia and sub-Saharan Africa are living with untreated obstetric fistula[5] . In Zambia, the 2018 ZDHS[6] shows that, women start having children at a young age, with over 33% giving birth before 18 and over 50% by age 20 and nearly 47.2% experience fistula during their first pregnancy, and multiple pregnancies increase the risk of obstetric fistula.
Obstetric fistula, particularly vesico-vaginal and recto-vaginal fistulas, poses a significant concern in terms of women's health and rights[7] . This condition predominantly impacts young women who are economically disadvantaged and lack education, particularly in low-resource settings. Consequently, it perpetuates a vicious cycle of poverty and social vulnerability[5,7] . Lack of access to emergency obstetric care exacerbates the condition, hindering women's ability to work or engage with their communities. Despite the importance of medical intervention during pregnancy and delivery in reducing the risks of maternal and infant mortality, Zambia has made remarkable progress in antenatal coverage in the last ten years. However, it is worth noting that only around 47% of deliveries in the country are attended by skilled health workers[8] .
The medical manifestation of fistula belies its roots in social, cultural, and economic contexts, underscoring wider vulnerabilities in reproductive health. Initiatives aimed at preventing fistula prioritize health education initiatives advocating for postponed marriage and childbirth, effective measures in reducing risks[9] . Nevertheless, there is lack of insight into the viewpoints and comprehension of patients regarding this condition. Bulndi[10] emphasizes the prevalent misconceptions held by women concerning fistula, which hinders prevention initiatives. Cultural beliefs, especially in rural regions, frequently endorse giving birth at home as a secure option, further complicating the task of effectively tackling fistula[11] . Given these intricate issues, examining fistula from the perspective of women of reproductive age presents valuable perspectives on potential strategies and regulations aimed at decreasing maternal morbidity and mortality rates[12] . The aim of this study was to explore the perceptions and lived experiences of obstetric fistula among women of childbearing age at the University Teaching Hospital in Lusaka, Zambia. Positioned in the southern region of Africa, Zambia is a landlocked country surrounded by eight neighbouring nations. The government's focus on improving healthcare and education access is evident through continuous initiatives aimed at enhancing infrastructure and service quality in these crucial sectors[6] . This investigation yields crucial evidence of the deficiencies within healthcare and social structures in meeting women's fundamental requirements, emphasizing the necessity to enhance their welfare.
METHODOLOGY
Study design
This study employed a descriptive phenomenological approach, using semi-structured, in-depth interviews to explore the lived experiences of women of childbearing age with obstetric fistula. This method is particularly suited for examining complex human experiences in healthcare contexts as it allows researchers to explore participants' subjective experiences. By focusing on participants' narratives, the study aimed to gain insight into the impact of obstetric fistula on affected women and their families, potentially informing more holistic, patient-centred care strategies.
Participants
The study was conducted at the University Teaching Hospital (UTH) in Lusaka, Zambia, between January and May 2010. The selection of the study site was based on its ability to grant access to participants who were pertinent to the research goals. Additionally, the chosen study site was deemed practical due to considerations of logistics and time limitations, given its accessibility and manageability within the study's parameters. For this study, a carefully chosen group of five (5) women of childbearing age, all of whom were living with fistula, was selected from the inpatient records. The decision on the sample size was influenced by the availability of appropriate participants undergoing treatment during the research period, as well as the unique characteristics of the population being studied. We conducted a thorough assessment of how well the selected sample aligned with the research objectives, methodological standards, and ethical considerations. This approach allowed for an in-depth exploration of each participant's personal experiences, perspectives, and narratives. The research team believed that such a detailed analysis would uncover important insights that might be overlooked in a larger sample. Hence, it was resolved that this sample size was adequate to provide relevant and comprehensive data on the experiences of women living with fistula within the specified time frame, effectively balancing the need for depth of understanding with practical constraints.
Data Collection
Data collection was carried out through recorded in depth interviews, allowing for an exploration of participants' experiences throughout their pregnancy, labour, delivery, and post-delivery periods, as well as the subsequent impact of fistula on various aspects of their lives, including psychological, physical, financial, and social dimensions. Interviews were conducted in a private and comfortable setting to facilitate open and honest dialogue.
Data Analysis
Recordings of the interviews were transcribed verbatim and meticulously reviewed for accuracy. Thematic analysis was employed to identifyrecurring patterns and themes within the data. Responses from participants were systematically coded to capture the diverse range of experiences and perceptions regarding fistula.
Ethical Considerations
Ethical clearance for the study was obtained from the University of Zambia School of Medicine undergraduate Research Ethics Committee of the University of Zambia (UNZASOMUREC No. S18/06/125). Additionally, written permission to conduct the research was sought and obtained from the administration of the University Teaching Hospital. All participants were assured of confidentiality, and their rights and privacy were upheld throughout the research process.
RESULTS
SAMPLE DESCRIPTIONS
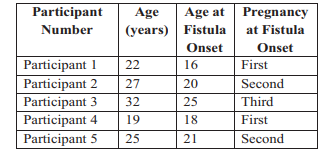
The study included participants aged between 17 and 32 years, who developed fistula at ages 16 (during their first pregnancy) and 31 (during their third pregnancy), respectively. The data summarized in this section is derived from the first-hand accounts shared by the participants during the interviews.
PARTICIPANTS PERCEPTIONS ON THE VARIOUS EFFECTS OF OBSTETRIC FISTULA.
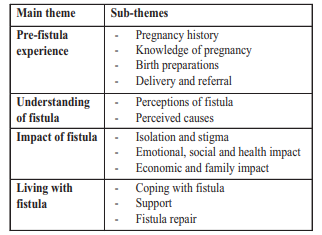
Our research findings on women's experiences with obstetric fistula is organized into four main themes, each with specific sub-themes detailed in Table 2, providing a structured and thorough breakdown. Pre-Fistula Experiences reviews participants' lives before the onset of fistula, focusing on their pregnancy and childbirth histories. Understanding Fistula explores their perceptions of the condition and its causes. Impact of Fistula outlines the broad effects of living with the condition, including social isolation, stigma, emotional repercussions, relationship difficulties, health challenges, financial strains, and family impacts. Living with Fistula examines daily experiences and the support systems available to those affected.
PREGNANCY HISTORY
All participants received antenatal care during their pregnancies, although in one case, attendance was delayed due to fear and attempts to conceal the pregnancy. Health education prompted one participant to opt for hospital delivery due to her age, while another attended antenatal appointments regularly.
Knowledge of pregnancy
One participant expressed familiarity with pregnancy and labour based on prior experience, while another participant recounted discovering her pregnancy only after a friend remarked on her appearance and advised her to seek medical confirmation. Another woman said,
“I didn't know I was pregnant until a friend of mine commented: you look so beautiful and your skin is so smooth, you might be pregnant. You need to go for a check-up at the hospital to be sure.” (P2)
Birth preparations, Labour, delivery and referral
Participants indicated intentions to deliver at healthcare facilities and had allocated funds for associated labour costs. All participants-initiated labour at home and experienced delays before receiving assistance and being referred to larger hospitals with the necessary resources as their facilities were not equipped to assist the women. However, participants encountered delays in reaching facilities equipped for safe delivery. Unfortunately, all experienced stillbirths. One participant underwent caesarean section, while another had a vacuum delivery. Reflecting on their experiences, one participant recalled realizing the problem only upon being informed of the need for surgery, while another noted the lack of progress during a prolonged labour. The woman stated,
“I realized that there was a problem after I was examined and told that I would deliver by operation.” (P4)
“I realized that there was a problem after spending the whole night with no progress.” (P1)
PERCEPTIONS OF CAUSES OF FISTULA
Based on insights gleaned from the in-depth interviews, participants expressed varied perspectives regarding the causes of fistula, spanning from the baby being too big and it being God's will. Other attributions included factors associated with the delivery process itself to delays in accessing delivery care and instruments used during delivery. One participant remarked,
"The baby was too big, had I sought medical attention promptly, I might not have developed fistula."(P3)
Similarly, another participant opined,
"I believe my prolonged labour and the instruments during delivery may have contributed to the rupture of my bladder." (P5)
IMPACT OF FISTULA ON THE WOMEN
The duration of living with fistula ranged from 7 months to 1 year among participants. One participant expressed that despite their marital happiness, she and her husband no longer shared a bed or engaged in sexual relations due to the fistula, leading to pressure from relatives for her husband to leave. Another participant reported being abandoned by her partner during pregnancy and being refused marriage due to the fistula and the loss of the baby. All participants noted that fistula had significantly impacted their ability to work, resulting in reduced income and increased dependence on others. Reasons for decreased work capacity included physical discomfort, constant need for cleanliness, and social stigma associated with the condition.
Isolation and stigma
Women with fistula isolated themselves from the community, avoiding public gatherings and social interactions due to feelings of shame and fear of embarrassment. The seclusion experienced by individuals was a direct consequence of their profound feelings of disgrace regarding their circumstances, coupled with an intense determination to avoid any instances of soiling themselves in the presence of others or emitting unpleasant odours. One participant expressed,
"While I maintain good relations with the community, I avoid visiting them because I am ashamed of my urinary leakage."(P2)
Emotional, social and health impact
Participants indicated that their family members underwent stress and worry regarding their situation. Furthermore, they encountered a range of emotional, social, and health consequences including alterations in health, sensations of illness or discomfort in the genital region, diminished vitality, debility, and exhaustion.
Economic and family impact
Treatment costs, including fistula repair and associated expenses such as transportation and hospitalization, posed financial burdens on the families of affected women. Participants mentioned expenses for treatment, clothes, and soap as common financial obligations. Family members were also affected economically, with decreased income due to the inability of affected women to engage in income-generating activities. One participant highlighted the strain on her family, with her brother bearing the financial responsibility for her medical care, while another participant noted the economic impact of purchasing soap for daily washing, diverting funds from other essential needs.
“It is hard on my family, because my brother is forced to look after me, and he has to look for money to treat my problem.”(P4)
“My family has suffered economically because I can no longer engage in any income-generating activities. Washing daily is costly, you must buy the soap. This money could be used for other things.” (P1)
COPING WITH FISTULA
Every participant expressed their unwavering dedication to upholding proper hygiene practices, which encompassed regular laundering of clothes and frequent bathing. One participant specifically stated,
"I prioritize the act of bathing regularly and ensuring that my clothes are frequently washed; this way, I guarantee that I don't emit any unpleasant smells associated with my urinary leaking problem, thus maintaining a sense of discretion." (P5)
Additionally, participants employed various other strategies to tackle concerns related to odour and leakage, such as changing clothes frequently, utilizing padding, and applying lotions. Reflecting on these approaches, one participant further explained,
"I effectively utilize padding to lessen the odour of urine that persists despite occasional instances of leakage." (P2)
SUPPORT
All the participants reported receiving different types of support from their families, indicating that none of them felt isolated or lacked support. The participants mentioned both financial and emotional support as forms of assistance they received. One participant highlighted her reliance on her husband for all her needs, including basic necessities. Meanwhile, another participant expressed the distress her family feels as she is their only daughter.
“They feel bad because I am the only daughter and rely on them for everything, even basic needs.” (P4)
FISTULA REPAIR
At the time of the interviews, all women were actively seeking fistula repair, a process that demanded significant sacrifices from their families in terms of both time and financial resources. One participant vividly recounted her difficult journey through a failed attempt at fistula repair, enduring a 41-day hospital stay without resolution of the issue. Despite the disappointment of returning home without success, she and her family remained resilient, determined to pursue a second attempt at treatment. Another participant provided insight into the challenges that had hindered her from seeking treatment earlier. Apart from logistical hurdles, such as travel and accommodation expenses, financial constraints emerged as the primary barrier. As she candidly expressed,
"Our financial situation limited our ability to seek treatment promptly, as the costs associated with travel and medical expenses were expensive." (P3)
DISCUSSION
The narratives shared by the participants in this study shed light on the multifaceted challenges they face when seeking treatment for obstetric fistula, underscoring the need for comprehensive support mechanisms to address not only the medical aspects but also the socio-economic barriers to care. These challenges extend beyond the medical procedure itself, encompassing financial burdens, logistical obstacles, and the necessity for emotional resilience. Recognizing and addressing these challenges is paramount in ensuring equitable access to quality healthcare for all women affected by obstetric fistula. The findings of this study challenge prevailing notions about the demographic profile of women affected by fistula. While data from other countries[13,14] often portrays fistula as primarily affecting young girls, our study revealed the presence of prime gravid and para-three gravid women presenting with fistula. This highlights the importance of public education and interventions that address the full reproductive life-cycle of girls and women, rather than focusing solely on young adolescents[15] . Despite the widespread utilization of antenatal care services, our study uncovered inadequacies in the care provided, particularly in addressing complications during labour. The need for comprehensive birth preparedness, including timely recognition of potential complications and prompt action, is evident. Health care providers require adequate training, supplies, and equipment to ensure the delivery of quality antenatal services that can effectively prevent emergencies[16] .
The lack of access to emergency obstetric care in our study, including timely caesarean sections, poses a significant threat to women's lives, particularly in rural areas where barriers to transportation and skilled health care workers are prevalent. Urgent measures are therefore, needed to ensure that women in these areas have access to timely and appropriate care during childbirth. High-quality fistula repair services as recommended by Deribe and colleagues[17] must be made available and accessible to all women, regardless of their geographical location or financial status. The substantial sacrifices made by women and their families to access treatment underscore the urgent need for subsidized or low-cost services in provincial centres. Despite receiving support from their families, the emotional and economic impacts of fistula on women and their families are substantial. Efforts must be intensified to reduce the stigma associated with the condition and alleviate the economic burden faced by affected individuals and their families through targeted interventions and advocacy[18] .
The accounts shared by the participants in our study highlight the various complex obstacles encountered by individuals seeking treatment for obstetric fistula. Apart from tackling socio-economic hindrances, it is crucial to acknowledge the significance of comprehensive care strategies in managing this medical condition[19] . Moreover, cooperation among healthcare providers is vital for administering thorough and well-coordinated care to women affected by fistula[20] . This collaborative method entails the involvement of diverse medical teams consisting of obstetricians, urologists, gynaecologists, nurses, midwives, and physiotherapists, among others. Through collective efforts, these medical professionals can offer holistic care that caters to the intricate needs of women coping with fistula, encompassing surgical correction, post-operative therapy, emotional support, and reintegration into society[21] . Effective management of obstetric fistula necessitates the implementation of various interventions. These approaches aim to strengthen pelvic floor muscles, improve bladder and bowel functionality, and enhance the overall quality of life for individuals impacted by this condition. By incorporating these strategies into comprehensive fistula management programs, healthcare professionals can achieve better treatment results while fostering the physical and emotional health of women. Customizing techniques such as pelvic floor exercises, biofeedback therapy, and bladder training to meet the unique requirements of each woman can facilitate their recovery and reintegration into society[22] . Effective collaboration among health personnel also extends to the prevention of obstetric fistula through improved antenatal and obstetric care. By working collaboratively, healthcare providers can ensure early detection and management of obstetric complications, timely referral to appropriate facilities for emergency obstetric care, and comprehensive birth preparedness education for women and their families.
LIMITATIONS AND CONCLUSION
Participants shared a variety of experiences related to their lives with fistula, highlighting their views on its impact and the daily challenges faced in managing the condition. Their stories reveal numerous difficulties associated with obstetric fistula, such as financial hardships, transportation issues, and a lack of treatment options. To provide comprehensive care and improve recovery and overall health for women affected by this condition, it is crucial to implement targeted treatment approaches and foster collaboration among healthcare providers. Additionally, it is important to acknowledge the study's limitations, particularly the small sample size due to the limited number of fistula patients and available resources, as these factors may affect the generalizability of the findings. Moreover, the conclusions drawn from the study rely on the researchers' interpretations and understanding of the data, which could introduce bias. To effectively manage obstetric fistula, a comprehensive approach is necessary, addressing not only the medical aspects but also the socioeconomic, psychosocial, and rehabilitative needs of affected women. To support and expand these findings, further research with larger and more diverse populations is necessary.
DECLARATIONS
Acknowledgement
The content of this publication relies on first-hand accounts gathered from patients who have utilized healthcare services at the University Teaching Hospital (UTH). We would like to extend our appreciation to the individuals who took part in this study, as well as the administration and personnel at UTH for their support in facilitating the involvement of these participants.
Competing interest
The authors maintain that their financial and interpersonal connections did not unintentionally influence their development of this article.
Author's contribution
All participants played a crucial role in the successful accomplishment of this project. The preliminary manuscript of the article was prepared by L.A.N, J.M.C, and K.M.C. The conceptualization and planning of our research were carried out by M.P and M.M.M. The ultimate rendition of the text underwent a comprehensive evaluation and obtained the endorsement of all the authors.
REFERENCES
- Landry, E., Vera, F., Ruminjo, J., Asiimwe, F.,Barry, T. H., Bello, A., Danladi, D., Ganda, S.O., Inoussa, M., Kanoma, B., Lynch, M.,Mussell, F., Podder, D. C., Wali, A., Mielke, E., & Barone, M. A. (2013). Profiles and experiences of women undergoing genital fistula repair: Findings from five countries. Global Public Health, 8(8), 926-942. https://doi.org/10.1080/17441692.2013.824018
- Finlay, J. E., & Lee, M. A. (2018). Identifying Causal Effects of Reproductive Health Improvements on Women's Economic Empowerment through the Population Poverty Research Initiative. The Milbank Quarterly, 96(2), 300-322. https://doi.org/10.1111/1468-0009.12326
- World Health Organisation (2018). Obstetric fistula. https://www.who.int/news-room/facts-in-pictures/detail/10-facts-on-obstetric-fistula
- Polan, M.L., Sleemi, A., Bedane, M.M., et al. (2015). Obstetric Fistula. In: Debas HT, Donkor P, Gawande A, et al., editors. Essential Surgery: Disease Control Priorities, Third Edition (Volume 1). Washington (DC): The International Bank for Reconstruction and Development / the World Bank; Chapter 6. Available from: https://www.ncbi.nlm.nih.gov/books/NBK333495/ doi: 10.1596/978-1-4648-0346-8_ch6
- Hareru, H. E., Wtsadik, D. S., Ashenafi, E., Debela, B. G., Lerango, T. L., Ewunie, T. M., & Abebe, M. (2023). Variability and awareness of obstetric fistula among women of reproductive age in sub-Saharan African countries: A systematic review and meta-analysis. Heliyon, 9(8). https://doi.org/10.1016/j.heliyon.2023.e18126
- ZDHS (2022) Obstetric Fistula Strategic Plan 2022 – 2026 https://www.afro.who.int/countries/zambia/publication/obstetric-fistula-strategic-plan-2022-2026
- Wall, L.L. (2006). Obstetric vesicovaginal fistula as an international public-health problem. Lancet (London, England), 368(9542), 1201–1209. https://doi.org/10.1016/S0140-6736(06)69476-2
- Mukonka, V., Sialubanje, C., McAuliffe, F. M., Babaniyi, O., Malumo, S., Phiri, J., & Fitzpatrick, P. (2024). Effect of a mother-baby delivery pack on institutional deliveries: A community intervention trial to address maternal mortality in rural Zambia. PLOS ONE, 19(3). https://doi.org/10.1371/journal.pone.0296001
- Rundasa, D. N., Wolde, T. F., Ayana, K. B., & Worke, A. F. (2021). Awareness of obstetric fistula and associated factors among women in reproductive age group attending public hospitals in southwest Ethiopia, 2021. Reproductive Health, 18. https://doi.org/10.1186/s12978-021-01228-2
- Bulndi, L. B., Ireson, D., Adama, E., & Bayes, S. (2023). Original research: Women’s views on obstetric fistula risk factors and prevention in north-central Nigeria: An interpretive descriptive study. BMJ Open, 13(6). https://doi.org/10.1136/bmjopen-2022-066923
- Adatara, P., Strumpher, J., Ricks, E., & Mwini-Nyaledzigbor, P. P. (2019). Cultural beliefs and practices of women influencing home births in rural Northern Ghana. International Journal of Women's Health, 11, 353-361. https://doi.org/10.2147/IJWH.S190402
- Institute of Medicine (US) Committee on Improving Birth Outcomes; Bale JR, Stoll BJ, Lucas AO, editors (2003). Improving Birth Outcomes: Meeting the Challenge in the Developing World. Washington (DC): National Academies Press (US). Reducing Maternal Mortality and Morbidity. Available from: https://www.ncbi.nlm.nih.gov/books/NBK222105/
- Changole, J., Thorsen, V. C., & Kafulafula, U. (2017). “I am a person but I am not a person”: Experiences of women living with obstetric fistula in the central region of Malawi. BMC Pregnancy and Childbirth, 17. https://doi.org/10.1186/s12884-017-1604-1
- Cowgill, K. D., Bishop, J., Norgaard, A. K., Rubens, C. E., & Gravett, M. G. (2015). Obstetric fistula in low-resource countries: An under-valued and under-studied problem – systematic review of its incidence, prevalence, and association with stillbirth. BMC Pregnancy and Childbirth, 15. https://doi.org/10.1186/s12884-015-0592-2
- Loureiro, F., Ferreira, M., & Antunes, V. (2021). Interventions to Promote a Healthy Sexuality among School Adolescents: A Scoping Review. Journal of Personalized Medicine, 11(11). https://doi.org/10.3390/jpm11111155
- Hussen, M. A., & Worku, B. T. (2022). Quality of Antenatal Care Service and Factors Associated with Client Satisfaction at Public Health Facilities of Bele Gasgar District. Journal of Patient Experience, 9. https://doi.org/10.1177/23743735221083163
- Deribe, K., Fronterre, C., Dejene, T., Biadgilign, S., Deribew, A., Abdullah, M., & Cano, J. (2020). Measuring the spatial heterogeneity on the reduction of vaginal fistula burden in Ethiopia between 2005 and 2016. Scientific Reports, 10. https://doi.org/10.1038/s41598-020-58036-0
- Pulerwitz, J., Michaelis, A., Weiss, E., Brown, L., & Mahendra, V. (2010). Reducing HIV-Related Stigma: Lessons Learned from Horizons Research and Programs. Public Health Reports, 125(2), 272-281. https://doi.org/10.1177/003335491012500218
- Schwarz, T., Schmidt, A. E., Bobek, J., & Ladurner, J. (2022). Barriers to accessing health care for people with chronic conditions: A qualitative interview study. BMC Health Services Research, 22. https://doi.org/10.1186/s12913-022-08426-z
- Pollaczek, L., El Ayadi, A. M., & Mohamed, H. C. (2022). Building a country-wide Fistula Treatment Network in Kenya: Results from the first six years (2014-2020). BMC Health Services Research, 22. https://doi.org/10.1186/s12913-021-07351-x
- El Ayadi, A. M., Painter, C. E., Delamou, A., Korn, A., Obore, S., Byamugisha, J., & Barageine, J. K. (2019). Rehabilitation and reintegration programming adjunct to female genital fistula surgery: A systematic scoping review. International Journal of Gynaecology and Obstetrics, 148(Suppl 1), 42-58. https://doi.org/10.1002/ijgo.13039
- 22. Brook, G., & ICS Physiotherapy Committee (2019). Obstetric fistula: The role of physiotherapy: A report from the Physiotherapy Committee of the International Continence Society. Neurourology and urodynamics, 38(1), 407–416. https://doi.org/10.1002/nau.23851
Medical Journal of Zambia, Vol 51, 2
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.