BREAST TUBERCULOSIS: A RARE OCCURRENCE WITH DIAGNOSTIC CHALLENGE IN A 21st CENTURY NIGERIAN FEMALE
Horace Ojobo Agada
Department of Surgery, Dalhatu Araf Specialist Hospital, Lafia, Nasarawa State, Nigeria.
Grimah Vechu
Department of Surgery, Dalhatu Araf Specialist Hospital, Lafia, Nasarawa State, Nigeria.
Godwin Tanze Joseph
Department of Surgery, Dalhatu Araf Specialist Hospital, Lafia, Nasarawa State, Nigeria.
DOI: https://doi.org/10.55320/mjz.51.1.473
Keywords:Anti-tuberculous medication, Breast tuberculosis, Carcinoma, Extra-pulmonary
ABSTRACT
Tuberculosis of the breast, also referred to as tuberculous mastitis, represents an extremely rare presentation of tuberculosis. It constitutes < 0.1 % of all breast pathology in developed countries and <2 % of all tuberculous cases globally.
It’s an infrequent manifestation of extra-pulmonary tuberculosis. It is characterized by diagnostic challenges with majority of preliminary clinical diagnosis being breast carcinoma or pyogenic breast abscess. The diagnosis is challenging due to the non-specific clinical and radiological findings, in addition to insufficient specimen with often negative microscopy and culture results.
We report the case of tuberculosis of the right breast in a young multiparous woman, a healthcare worker who presented with clinical features suspected to be breast tuberculosis in whom diagnosis was made based on clinical, haematological parameters and tuberculin skin test only. She was commenced on anti-tuberculous medications with excellent clinical response after 6 months of therapy.
This report highlights the importance of considering tuberculosis as a differential diagnosis in women with breast lumps and sinuses. In addition, this report also highlights the diagnostic challenges in breast tuberculosis and how a high index of suspicion and non-bacteriological investigation could be relied upon for its diagnosis.
INTRODUCTION
Tuberculosis is a chronic granulomatous infection caused by Mycobacterium tuberculosis. It is a disease that is common in low and middle-income countries of the world.[1] Tuberculosis (TB) primarily affects the lungs but has the ability to affect other organs (extra-pulmonary) such as the lymph nodes, genitourinary system, bones and joints, gastrointestinal system, central nervous system and spine.
Tuberculosis of the breast is an infrequent form of extra-pulmonary TB. It is classified into 2 sub-types, primary and secondary breast TB. Primary breast TB occurs via infection through skin abrasions or openings of the lacrimal ducts at the nipple without any extra-mammary focus. The secondary variety is more common and develops by either direct extension, haematogenous spread or lymphatic route which is the most common route of spread from an extra-mammary focus such as the lungs .[2,3]
The young, multiparous, lactating and immunocompromised women are at increased risk for breast TB.3 It often mimics a cancer in having a lump in the upper outer quadrant or central aspect of the breast that is fixed to the skin and underlying tissue, in addition to having ill-defined margins. A histopathologic report of the presence of neoplastic cell is need to confirm a diagnosis of cancer. Although culture-based diagnosis is recommended as the Gold-standard in TB care, lack of resources and technical expertise poses a major limitation in most of the high prevalence countries regarding the diagnosis of TB.[4]
The diagnosis of extra-pulmonary TB is a major challenge for two reasons, first is the difficulty in obtaining appropriate clinical sample, especially from the non-reachable sites and second is the poor sensitivity of diagnostic tests.[5]
CASE PRESENTATION
A 36-year-old female health care worker was referred from a peripheral hospital on account of a right breast lump of 12 months duration. There was associated right axillary swelling and multiple discharging sinuses that extended to the breast. This suggest possible initial lymph node affectation before extension into the breast tissue from lymphatic route. She had anorexia, occasional low-grade fever and drenching night sweats but no weight loss or history suggestive of anaemia. There was history of contact with a known TB patient on medication. She had no bloody nipple discharge, identifiable risk factor for or family history of malignancy. Prior to being referred, she had been on several antibiotics and analgesics without improvement.
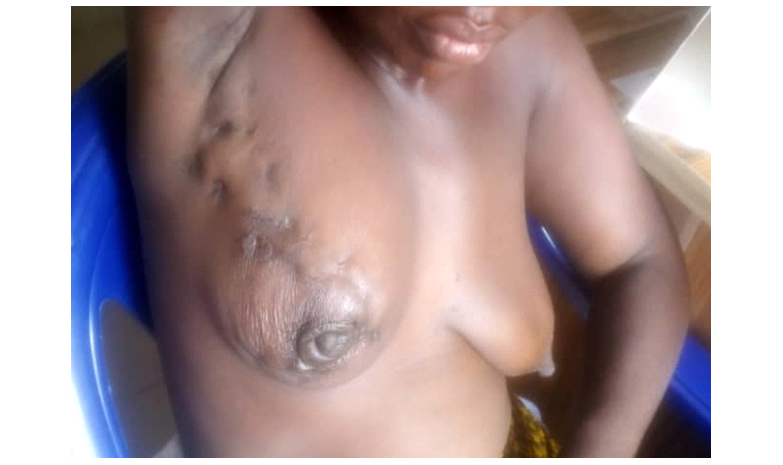
Breast examination revealed a shrunken right breast with preserved nipple-areolar complex but retracted nipple. There were multiple non-discharging sinuses that extended into the ipsilateral axilla. The right breast also harboured an ill-defined mass in the upper outer quadrant measuring 3cm x 3cm. It had no differential warmth, non-tender, firm and attached to overlying skin and underlying structure. She also had matted ipsilateral groups of lymph nodes. Other examination findings were unremarkable. (Figures: 1 and 2)
A provisional diagnosis of right breast TB with a differential diagnosis of breast malignancy was entertained.
Laboratory investigation revealed elevated total White Blood Cell [WBC] count with differential lymphocytosis [WBC –11.3 x 109/L , Neutrophils –28%( 3.1 x 109/L ) , Lymphocytes –50%( 5.6 X 109/L ) , Monocytes –12%( 1.3 X 109/L )] ,raised Erythrocyte sedimentation rate (ESR) - 61mm/hr and Mantoux test ( 10.0 mm). Report of chest x-ray was unremarkable. Her Fasting Blood Glucose level was within normal limits while her retroviral screening was seronegative. Tissue stain for acid fast bacilli and Gene- Xpert were unremarkable. Core tissue biopsy of the breast lump was done with a report showing fibro-adipocytic tissue with marked infiltration by mononuclear inflammatory cells. No neoplastic cell was seen. A histologic diagnosis of chronic non-specific Inflammation was made.
A diagnosis of breast TB was eventually made based on the clinical history and signs, Lymphocytosis, elevated ESR and Mantoux test. She was referred to the infectious disease unit and was placed on anti-tuberculous medication consisting of Rifampicin, Isoniazid, Pyrazinamide and Ethambutol for 6months duration.
After 6 months of treatment, she had a remarkable resolution of symptoms with improved quality of life. (Figure: 3)
She has been on follow-up for 2 years without recurrence.


DISCUSSION
Tuberculosis is the principal cause of mortality from a single infectious agent and is among the leading 10 causes of mortality globally.6It is a communicable but preventable infectious disease caused by Mycobacterium tuberculosis. The prevalence of this condition is high in the low- and medium-income countries, thus, reflecting the low socio-economic status of the population.[6]
The lung is the principal site of TB with other sites (extra-pulmonary) constituting 15-20 % of cases. The extra-pulmonary sites include the lymph nodes, abdomen, spine, pericardium, kidneys and rarely the breast. Breast TB is an uncommon disease with an incidence of < 0.1 % of all breast pathology in western countries and between 3 % and 4 % in India and Africa.[7]
The clinical presentation of breast TB has been categorized into three: sclerosing, nodular and diffuse. The sclerosing type (1.4 %) presents with nipple changes resulting from fibrosis. The diffuse type (11.2 %) is characterized by ulcerations and sinuses whilst the nodular type is represented by a focal mass lesion.8Our patient had a mixture of the three types of clinical presentation of breast TB.
While breast TB are unilateral in majority of their presentations, Mac Gregor and Wilson demonstrated bilateralism in 3% of cases.[9]
The diagnosis of breast TB can be elusive, necessitating a high index of suspicion. The tuberculin skin test developed by Koch in 1890 and subsequently modified by Charles Mantoux in1912 is still widely used as a vital test for the diagnosis of tuberculosis. Several factors influence its outcome and interpretation as described below: [10]
Five [5] mm or more is positive in
• HIV-Positive person • Recent contacts of active tuberculosis cases • Persons with nodular or fibrotic changes on Chest X-ray consistent with old healed TB • Patients on cytotoxic/ immunosuppressive agents • Patients on long term systemic steroids • Patients with end stage renal disease
Ten [10] mm or more is positive in
• Recent arrivals [ less than 5 years] from high-prevalence countries • Injectable drug users • Residents and employees of high-risk congregate settings [e.g., prisons, nursing homes, hospitals, homeless shelters, etc] • Mycobacteriology laboratory personnel • Persons with clinical conditions that place them at high risk [e.g., diabetes, prolonged corticosteroid therapy, leukaemia, end-stage renal disease, chronic malabsorption syndromes etc.] • Children less than 4 years of age, or children and adolescents exposed to adults in high-risk categories • Infants, children, and adolescent exposed to adults in high-risk categories
Fifteen [15] mm or more is positive in
• Persons with no known risk factors for TB. Reactions larger than 15mm are unlikely to be due to previous BCG Vaccination or exposure to environmental mycobacteria.
Our patient was considered to have a positive Mantoux due to her induration size of 10mm in addition to having recent contact with active tuberculosis patient.
A negative smear for acid-fast bacillus, a lack of granulomas on histopathology, and failure to culture mycobacterium tuberculosis do not exclude the diagnosis.[11] Giovanni et al in their report, made a diagnosis of Breast tuberculosis following a positive QuantiFERON –TB Gold assay.[12] This assay shows the presence of cell mediated immune response to antigens ESAT-6 [early – secreted antigenic target] and CFP-10[culture filtrate protein] of Mycobacterium tuberculosis.
The traditional diagnostic methods for TB relied on medical history, tuberculin skin test, chest x-ray, haematological parameters like lymphocyte count and Erythrocyte sedimentation rate as well as bacteriological examination.[5] The diagnosis of our index patient was made based on the non-bacteriological diagnostic methods.
Core tissue biopsy or Fine needle aspiration cytology represent surgical role in breast TB management in which tissues are obtained for the detection of the bacilli or the presence of granulomas or epithelioid cells. This was not the case of our patient as the histology revealed only features of chronic inflammation.
Gene-Xpert is a diagnostic tool introduced by the World Health Organisation in 2010 for the management of TB that simultaneously detects Mycobacterium tuberculosis and Rifampicin resistant variants.[13] In March 2017, the World Health Organisation, launched the second –generation Gene Xpert Ultra. It has a higher sensitivity, minimally invasive, requires no specialized equipment, and gives rapid result. Kohli et al, were able to demonstrate that the sensitivity of Gene Xpert Ultra on fine needle aspiration could be as high as 87.6%.[14]
Surgical intervention is also needed in the drainage of breast abscess, excision of sinuses and masses. In patients with large painful ulcerative lesions or lack of response to anti-tuberculous medications, mastectomy may be indicated.[15]
CONCLUSION
• A high index of suspicion is needed for the diagnosis of breast TB • This case highlights the importance of considering breast TB as a differential diagnosis in patients with multiple sinuses and mass involving the breast that is unresponsive to non-tubercular antibiotic therapy. • The finding of negative bacteriological test does not exclude breast TB • Lastly, this case demonstrates the need of considering non-bacteriological diagnostic methods in an attempt at overcoming the diagnostic challenges in patients with breast tuberculosis.
DECLARATIONS
Conflicts of Interest
Authors declared they have no conflicts of interest.
Patients Perspective
Patient was surprised and elated with her accelerated recovery just after 2 weeks of commencement of the anti-tuberculous medications.
Informed Consent
An informed consent for publication was obtained from the patient.
REFERENCES
- Dodiyi- Manuel ST, Dodiyi- Manuel A. Tuberculosis of the Breast. Niger J Med 2013; 22(1):72-74
- Giovanna R, Francesco C, Paolino D, Antonella B, Gabriella M, Gaspare G. An unusual presentation of breast tuberculosis; A case report. Clin Case Rep 2021;9: 210-212
- Ghalleb M, Seghaier S, Adoune O.Bouaziz H, Bouida A, Hassouna JB, Chargui R, Rahal K. Breast tuberculosis; A Case Series. J Med Case Reports 2021; 15: 73
- Hopewell PC, Pai M, Maher D, Uplekar M, Raviglione MC. International standards for tuberculosis Care. Lancet Infect Dis 2006; 6:710-725
- Sarman S, Bindu D, Sachdeva K, Kabra S, Chopra K, Vijay C, Pawan S, Katoch V. Challenges in Tuberculosis Diagnosis and Management; Recommendations of the Expert Panel. J Lab Physicians 2015;7(1): 1-3
- Diop M, Ba P, Tine J, Fall N, Youbong T, Ndiaye M et al. Factors Associated with Death among Tuberculosis Patients in Dakar. Advances in Infectious Disease .2021;11:122-139
- Ugbem TI, Adekanye AG, Udosen JE, Akpan S. Tuberculosis of the breast; A case report in a tertiary health institution, South-South Nigeria. Calabar J Health Sci 2023; 7; 47-49
- Toumi S, Chenguiti A, MoutaaI.Breast tuberculosis: a case report. PAMJ-Clinical Medicine 2022; 8:53
- Wilson TS, MacGregor JW. The Diagnosis and Treatment of Tuberculosis of the Breast. Can Med Assoc J 1963;89(22):1118-1124
- Surajit N, Basanti A. Mantoux test and its interpretation. Indian Dermatol Online J. 2012; 3(1):2-6
- Marjorie P, Golden M, Holenarasipur R, Vikram M. Extrapulmonary Tuberculosis: An overview. Am Fam Physician. 2005;72(9):1761-1768
- Giovanni Antonella M, Francesca C, Enza P, Simona P, Mauro C, Cristina M. Breast tuberculosis; A case report of primary type mammary tuberculosis. Clin Case Rep 2019;7(12):2346-2348
- Boehme CC, Nabeta, Hillemann, Nicol MP, Shenai S, Krapp F et al. Rapid molecular detection of tuberculosis and rifampin resistance. N Engl J Med. 2010;363(11):1005-1015
- Kohli M, Schiller I, Dendukun N. Gene Xpert, MTB/RIF assay for extrapulmonary tuberculosis and rifampicin resistance. Cochrane Database Syst Rev .2018; 8: CD 012768
- Tewari M, Shukla H. Breast tuberculosis: diagnosis, clinical features and management. Indian Journal of Medical Research. 2005; 122(2):103-110
Medical Journal of Zambia, Vol 51, 1
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.