An Evaluation of the Consequences of Covid-19 On Immunisation Programme Financing and Service Delivery in a Lower Middle Income Country: The Case of Zambia
Moses C Simuyemba
Department of Community and Family Medicine, University of Zambia School of Public Health, Lusaka, Zambia
Chitalu Chama-Chiliba
Department of Economics, University of Zambia School of Humanities and Social Sciences, Lusaka, Zambia
Abson Chompola
Department of Economics, University of Zambia School of Humanities and Social Sciences, Lusaka, Zambia
Aaron Sinyangwe
Department of Economics, University of Zambia School of Humanities and Social Sciences, Lusaka, Zambia
Abdallah Bchir
Monastir Medical School, University of Monastir, Tunisia
Gilbert Asiimwe
Gilbert Asiimwe
Felix Masiye
Department of Economics, University of Zambia School of Humanities and Social Sciences, Lusaka, Zambia
DOI: https://doi.org/10.55320/mjz.51.1.466
Keywords:Immunisation, Covid-19, Zambia
ABSTRACT
Background: The COVID-19 pandemic has disrupted health systems globally, affecting various services, including immunization programs. This study evaluates the impact of COVID-19 on immunization program financing and service delivery in zambia, a lower-middle-income country, to understand how such disruptions could reshape future healthcare priorities and funding.
Methods: The study employed a mixed-methods approach, integrating both qualitative and quantitative data collection. Data were gathered at national and sub-national levels, including in-depth interviews with 36 healthcare workers and an online survey completed by 44 staff members. The evaluation focused on the changes in government funding, the effect on static and outreach immunization activities, vaccine supply distribution, and the impact on human resources within the Expanded Programme on Immunisation(EPI).
Results: Findings indicated that while regular disbursements to districts improved in 2020, there was heightened competition for limited resources due to COVID-19, leading to a redirection of funds from routine immunization to pandemic-related activities. The study revealed a significant decline in immunization coverage, attributed to reduced health facility visits and outreach sessions. Additionally, financial constraints heightened by the pandemic made it challenging for districts to accomodate the extra costs associated with implementing COVID-19-compliant immunization services. Human resources for immunization were also impacted, with staff being reallocated to COVID-19 response activities, thus increasing workload and stress levels among remaining personnel.
Conclusion: COVID-19 has substantially affected the funding, delivery, and human resource components of Zambia's immunization program. Despite an increase in regular funding disbursements, the rediection of funds to COVID-19 activities has strained routine immunization services. The pandemic has highlighted the need for robust health systems that can withstand global health crises without compromising essential services like immunization. Recommendations include closer monitoring of immunization service delivery impacts, assessment of COVID-19's financial implications on immunization, development of clear protocols for service delivery under pandemic conditions, and a re-investment in community engagement and education post-pandemic.
INTRODUCTION
Since its emergence in late 2019, Covid-19 has spread globally and has affected all facets of human life, including health systems. There is some evidence that disruptions to providing health services has effected all areas including immunisation services,HIV & AIDS and other routine health services. Zambia has not been spared in this regard and we use this case study to highlight how lower middle income countries in Africa have been affected by Covid-19 in the area of immunisation service delivery. Zambia, in Southern Africa, has an estimated population of 18 million people in 2021 according to the Zambia Statistics Agency and a high poverty burden with under-five mortality rate at 61 per 1000 live births, a decline from 75 in the preceding survey.[1] The Expanded Programme On Immunisation (EPI) has been running in the country and in the last two decades, it has been mainly funded by the government and Gavi, with support from other partners. It targets mainly under-five children and more recently girls up to the age of 14 for HPV Vaccination.[2] Various vaccines are delivered by the programme and this includes vaccines for diphtheria, pertussis, tetanus, hepatitis B, Haemophilus influenza type B, rotavirus, polio, pneumococcus, measles, rubella and tuberculosis.[3]
The Gavi Full Country Evaluation (Gavi FCE) has been ongoing in Zambia since 2014 and this phase of the evaluation between 2019 and 2020 focused on identifying opportunities and obstacles to sustainable financing and programmatic performance of the Zambian immunisation programme.[2] The effects of Covid-19 on the immunisation service delivery was one of the components of the evaluation and is the focus of this paper.
Covid -19 began in Late 2019 and by March 2020, Zambia had recorded its first case. At the time of the data collection for this evaluation around August 2020, the country had recorded over 10,000 cases and almost 300 deaths.[4] The chart in the supplemental material provides a summary of trend in cases, deaths, and case fatality rate in Zambia between March and September, 2020. Covid -19 vaccination in Zambia began in April 2020, so at the time of this study no Covid -19 vaccines had been administered.[2]
The evaluation sought to answer the following questions: (i) To what extent has the outbreak of Covid -19 affected government funding to key immunisation programme activities for EPI? (ii)How are both the static and outreach immunisation activities affected by Government’s |Covid-19 measures? (iii)To what extent has Covid -19 affected the supply of vaccines to the country and distribution of vaccines sub-nationally? (iv) How has Covid -19 affected immunisation human resources?
METHODS
Data was collected at both national and subnational levels for the evaluation. The sample for the subnational level built on the EPIC sample of 2011, which included nine districts in three provinces [5] with inclusion of an additional province in consultation with the Ministry of Health. These were Lusaka province (Lusaka, Kafue and Chongwe districts); Copperbelt province (Ndola, Masaiti and Lufwanyama districts); Central province (Kabwe, Serenje and Mkushi districts) and Muchinga province as the addition (Mpika, Shiwang’andu and Chinsali districts).
Both qualitative and quantitative methods of data collection and analysis were used to address the key questions that describe the impacts of Covid -19 on the immunisation programme. These were: - In-depth qualitative interviews with 36 health care workers (at national, provincial and district levels) involved in planning and implementing immunisation activities. These focused on assessing the observed impacts on the immunisation programme since Covid -19 using a thematic framework based on four domains of health system building blocks, namely human resources, service delivery, financing and vaccine supplies and logistics[6] . - An online survey was conducted with 44 staff (100% response rate) on perceptions of the effect of Covid -19 in sampled districts using SurveyMonkey. - Analysis of adminsitartive data on administered immunisation doses (HMIS database) for each district for the period January 2018 through to June 2020. - Finally, we conducted a costing exercise using activity ingredients approach. Data on cost itemswas collected from the sampled districts. We estimated the added costs of implementing immunisation sessions at facilities and outreach while observing Covid -19 guidelines. Major costs included Personal Protective Equipment (PPEs), sanitary supplies and outreach service delivery costs.
Patient and Public Involvement No patients were involved in the study and thus the development of the research question and outcome measures was not informed by patients’ priorities, experience, and preferences. Key informants were involved at national and district levels and they were consulted in the development of the evaluation questions through the EPI Technical Working Group (TWG) and several meetings that were held with EPI stakeholders. Findings were shared with these stakeholders through the EPI TWG, through the evaluation report and various publications, including this one.
Ethical considerations Ethical approval was obtained from the University of Zambia ethics board and national clearance from the National Health Research Authority and the Ministry of Health. Participation in survey and interviews was voluntary. The purpose of the evaluation was explained to the participants and informed consent was obtained. All data collected, including audio recordings, was securely stored and only researchers participating in the evaluation had access to the data.
FINDINGS AND DISCUSSION
The findings and discussion are presented together, in conformity to the Gavi Full Country Evaluation reporting style [2,3,7,8] . Each finding is based on multiple data sources, as described in the methods section, and relies on triangulation across these data sources. Findings are framed in a manner that summarises the main issues from such triangulation and that would be most useful to country stakeholders and Gavi for decision-making.
Immunisation Financing Finding: There was more regular disbursements of the monthly operational grant to districts in 2020 but there was also increased competition over scarce resources as districts had to prioritize Covid-19 related operations.
Provinces, districts and facilities are supposed to receive monthly disbursements of the operational grant from the Ministry of Health to meet costs of running primary health care services at subnational level. For immunisation, the grant is used for costs such as fuel and lubricants (for outreach and supervisory visits), cold chain maintenance, field staff allowances and per diem, administration (stationery, insurance, utilities, etc.), supplies, and so on. These grants are however not always disbursed on a monthly basis as planned and are often unpredictable with recent reports of declining funding.[9,10] Supportive supervision and mentorship, as well as community mobilisation activities, are often the areas that suffer when funding is short and these have been reported to be inadequate for many years.[2,9,11,12,13] Irregular and diminishing funding has the additional effect of making staff demotivated to plan and manage resources efficiently.[9]
In all the twelve sampled districts in this evaluation, it was learned that government funding for general operations had improved in 2020 compared with 2019 and 2018 in terms of being more regular, partly attributable to the Covid-19 situation that necessitated action by MOH.[8] However, the amount of resources available for immunisation programme activities had effectively reduced, as districts had had to meet new costs of addressing Covid -19 and they had not received any additional funding specifically meant to cover Covid-19 related costs, such as for personalprotective equioment (PPEs). Both key informant interviews and the survey conducted supported this with 78% of survey respondents indicating that Covid-19 had reduced the level of funding available for immunisation as Covid-19-related activities took precedence over routine health services, although in the annual planning cycle Covid-19 had not been considered as it had not arisen yet.
“I can say yes to some extent, there are has been funds diverted to Covid-19…This year 2020, the grant has been consistent…and I can say that out of eight, we have received six grants, which is almost 80 percent. But most of that money is going to issues of Covid-19. There is need to take samples, do contact tracing for Covid patients, do referral of patients, and all those things…Now you move funds where there is a need. Some funds are moving from immunisation towards Covid-19 fight.” District level Key Informant.
The EPI programme in Zambia also relies a lot on partners who often pitch in to meet shortfalls in funding for various activities.[11,14,15] With the Covid-19 situation, this support became uncertain as some partners channelled support to Covid-19 activities instead.
“Yes, there are some donor funds…which were supposed to go for immunisation to the facilities… this funding was suspended, it should be, in February. We were told that the funding has been directed to support Covid-19 [activities].” District level Key Informant
As a result of the scarcity of funding, some districts gave priority to high-density areas or high volume facilities for immunisation activities in order to be more efficient in the use of available resources and to vaccinate more children. This way, apart from lowering the financial cost per child immunised, vaccine wastage was also minimised. Inevitably, this comes with a downside of inequitable coverage, as children in remote places were less likely to get vaccinated. These areas were already disadvantaged in many ways in terms of equity and coverage[10,16] and thus Covid-19 exacerbated the situation.
Finding: The additional financial cost of implementing Covid-19 compliant immunisation service delivery was beyond the budgets of most districts.
The evaluation sought to establish the financial cost to health facilities of catering for the extra demands of Covid-19 and these are presented in Table 1. These are incremental costs per health facility per month. Cost calculations showed that the financial implications of Covid-19 were considerable and beyond the budgets of health facilities. We estimated that a typical facility would need an additional ZMW 4, 330.16 (US$246.45) per month to safely implement immunisation outreach and facility-based sessions under prevailing Covid-19 measures in Zambia. This additional amount was approximately equal to the total operational grant that a typical health facility received per month. The largest cost items related to supplies for PPEs and sanitization, and fuel for outreach visits. This situation was compounded by the fact that many facilities did not have adequate PPEs even before the Covid-19 pandemic.[17]
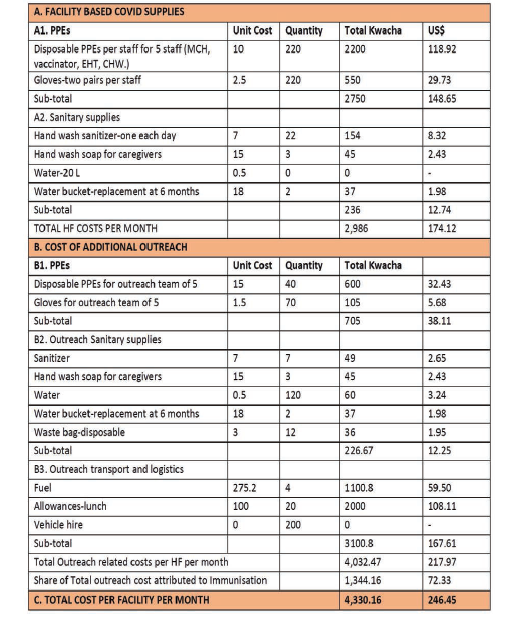
In relation to the financial resources available for immunisation activities, we argue that these resources were unlikely to increase to meet the added costs on the programme due to Covid-19. Key informant interviews revealed that health staff were going without adequate PPEs while outreach sessions were suspended because the government was simply failing to meet these additional costs.
Immunisation Service Delivery Finding: There was a decline in both facility and outreach based immunisation coverage in most districts during the period of restrictions imposed by Covid-19 prevention measures.
Immunisation planners and implementers in most districts reported in interviews that their districts were experiencing a significant drop in immunisation attendance at health facilities as well as decreased immunisation outreach sessions since Covid -19 broke out, as shown in figures 1 and 2. This is in the background of already inadequate outreach session in most districts due to funding challenges.[13,18,19]
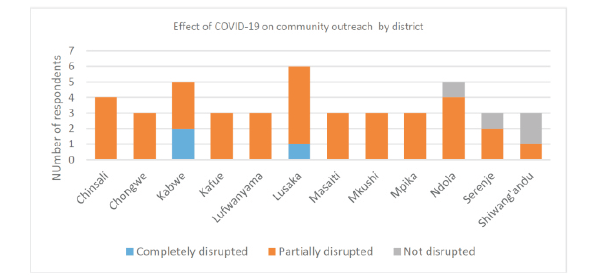
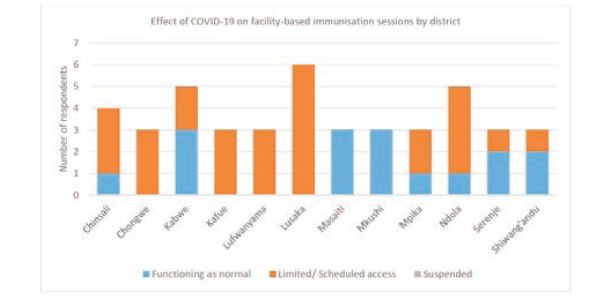
Many districts suspended immunisation outreach and put restrictions on facility-based sessions as a result of trying to interpret and implement initial government guidance on restricting gatherings. Although the MOH had not issued any guidelines to cancel outreach sessions, districts in Covid-19 affected areas found it was not feasible to conduct outreach.
In addition, some care-givers were shunning both outreach and facility-based sessions for fear of contracting Covid-19. They believed that contact with health care workers would expose them to Covid -19. Some care-givers also harboured the myth that Covid-19 was not a real disease and thought that these outreach sessions were methods for health workers to go around communities to gather fictitious Covid-19 statistics in order to get donor funding. Another reason was that care-giver were discouraged by the long time it took to get their children vaccinated. As facilities ensured social distancing at vaccination sites, the pace of immunisation service delivery had slowed. Facilities also reported longer waiting hours as some immunisation staff were deployed to screening patients for Covid-19 and triaging patients at the outpatient department. Some staff were also involved in ensuring social distancing among care-givers.
“We know that there was a directive …..that community activities should reduce. Even if you send the volunteers that we work with into the communities, those that are trained in RED [Reach Every District] strategy, the response hasn’t been very good from members of the public. Sometimes people fear that health workers are carriers of the virus. So when you go that side you spread the disease. The activities are there, but the numbers are not good.” District level Key Informant
It is also important to acknowledge that there was costs of PPEs that fell on care-givers. Qualitative interviews with health staff indicated that the cost of PPEs presented a barrier to the poorest as health workers did not allow anyone without a mask to enter a facility. Many of the poor in communities could not afford masks and hand sanitiser, for example. It was also conceivable that in remote areas, even finding a mask in a shop could have been a challenge. With such conditions, caregivers in many communities were unable or reluctant to go to facilities.
“Mothers do not come to the facility because some of them cannot afford to buy masks. These masks cost ZMW10 to ZMW20 (US$0.50-US$1). The mother must buy her mask and that of the child or children. For poor people that is a lot of money in these difficult times. In some facilities they put a guard to chase away anyone who is not wearing a mask.” District level Key Informant
Global estimates using DPT3 coverage were that infant immunization coverage dropped to 83% in 2020, leaving 3.7 million more children un-or under vaccinated than in 2019 as a result of Covid-19.[4] In Zambia, data from facility immunisation registers, which included children immunised during outreach, demonstrated that DPT3 coverage figures show that the number of vaccines administered since March 2020 dropped in comparison to the numbers given during the same period in previous years in most of the 12 districts sampled. This drop was not explained by stock-outs or any other factors. Vaccine delivery data also showed that districts did not face any stock-out of vaccines during this period. Plausibly, the drop in the number of doses given reflects the reduction in facility visits by caregivers as well as the reduced number of outreach sessions.
Human Resources For Immunisation Finding: The effect of Covid-19 on immunisation system human resources was mixed. Generally, adverse effects were more severe in areas where the disease incidence was high.
Under this finding, we present evidence from a survey of immunisation planners at the provincial and district levels. The respondents were asked questions on the effects of Covid-19 focusing on four specific dimensions of human resource impacts, namely: (i) availability of staff to conduct immunisation service delivery; (ii) workload of immunisation staff; (iii) stress among immunisation staff; and (iv) the volume of reporting that immunisation staff had to do. This was further triangulated with evidence gathered from interviews with immunisation planners and implementers in the three provinces and 12 districts.
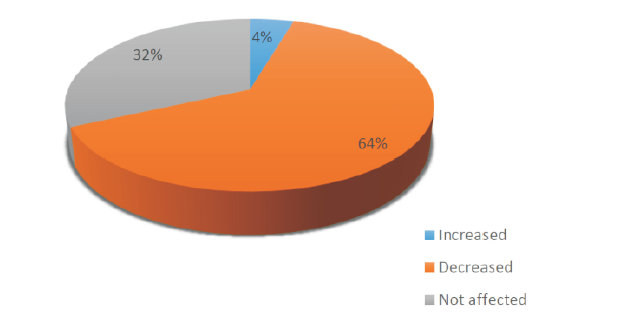
Figure 3 shows that nearly two-thirds of districts reported experiencing a reduction in the number of staff that were available to work in immunisation service delivery. About one-third stated that there was an increase in the number of immunisation staff working since Covid-19 emerged. The rest reported no change in the number of staff working in immunisation. These staffing challenges grow in magnitude when one considers that staffing is generally inadequate, without the exacerbating factor of Covid-19. [20]
Reductions in the number of staff working in immunisation could have occurred due to the re-deployment of staff to support Covid-19 efforts. These activities included contact tracing, taking samples, screening patients at facilities, sensitizing people in communities, and supervising health facilities about adherence to Covid-19 measures. There were districts which reported that some staff had been mobilised away from immunisation towards Covid-19 related activities.
“Most of our EHTs and nurses whom we reply on for immunisation outreach, are now doing Covid rapid response teams. They are the ones going around wherever there is a suspected case. That has affected our staffing. They have taken almost everyone from (21) district. So we are actually hit by shortage of staff. ”District level Key Informant
With limited human resources, some facilities remained with no staff to attend to general routine health services.
“So we are actually hit by shortage of staff, and who are not even paid for the services, no motivation at all. And also workload, and also knocking off late. Sometimes even the protective clothing is not enough, others are even being infected.” District level Key Informant
Outreach immunisation taps into freely available community volunteer labour to provide more than 60% of the human resource required to implement immunisation service delivery. This allows the Ministry to not only reach more children but does so at costs which are substantially less than those that would be incurred if immunisation is delivered at the health facility. In general, districts which reported Covid-19 cases had experienced a significant effect in terms of operating with severely limited staff as some of its vital human resources such as Environmental Health Technicians who conduct community-based mobilisation and vaccinations were re-dedicated to do contact tracing for Covid-19.
With regard to workload, we report two divergent experiences. The results show that half of the respondents reported an increase in workload. However, there was also one-third of staff who reported a reduction in workload, i.e. the volume of daily routine work that they were involved in. About 15% of staff surveyed saw no change in the volume of their daily routine work. In the qualitative interviews, we explored whether the increase in workload was necessarily overwhelming or undermining performance and quality. Evidence from the qualitative interviews showed some clear indications of staff demotivation due to their involvement in the fight against Covid-19, leading to increased workload.
“There is no motivation. Sometimes even protective clothing is not enough. They are not being paid. They are working long hours. Others are getting sick. There are some of our staff who are facing more hours of work. Sometimes we receive calls in the night, we have to go everywhere at short notice. ” District level Key Informant
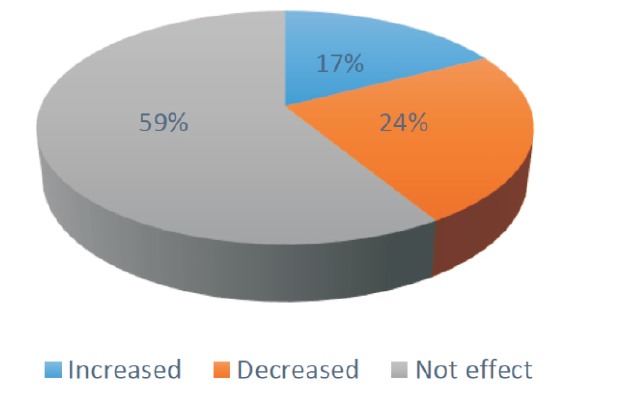
Finally, there was limited evidence that Covid-19 had adversely affected immunisation reporting. Immunisation staff spent a significant amount of time recording the number of visits, tallying children, and doses dispensed and so on. About 18% of respondents in the survey reported having experienced an increase in reporting requirements associated with Covid-19, 24% reported a decrease and 59% reported no effect as illustrated in figure 4.
More than half of the respondents stated that they had experienced significantly higher levels of stress attributed to Covid-19. A significant 40% stated that they had experienced a moderate impact on job-related stress. Although the survey did not report baseline stress levels, these findings do indicate that Covid-19 had resulted in increased stress among immunisation workers. Districts and health facilities normally operate with a shortage of health personnel. It is not surprising that shifting staff to fight a new major epidemic would put more workload on the few staff available, thereby leading to increased stress. There are quality implications from such levels of stress. Key informants indicated that health workers lacked sufficient guidance on how to offer immunisation services under Covid-19 conditions while fear among immunisation staff to deliver services:
“The lack of protocol and service delivery for the staff has been our biggest challenge. Them not knowing how to respond to this. So now someone comes with a cough and all those signs, there is a temperature. I don’t know, I can only suspect it’s a Covid case. But then if everything becomes Covid. So clear guidance is what has been the greatest challenge. And it also breeds fear among our staff. If people cannot offer a service because of inadequate protocol and knowledge there, then you know that quality of service is compromised. And I also think that facility-based immunisation has been affected because there are no people.” District level Key Informant
Vaccine Supplies and Logistics Finding: Although vaccines and related supplies were generally available, BCG and OPV had either stocked-out or were on the verge of stocking-out as a result of global supply chain disruptions due to Covid-19.
Generally, there was no reported stock-out of vaccines in facilities in most parts of the country except for BCG. Facilities reported stock-outs of BCG, which was attributed to Covid-19. Ten of the twelve districts reported that they had been out of BCG since early May until the time of the survey (August 2020). Polio vaccine (bOPV) was also under threat of running out according to some interviews. The official position from the Ministry confirmed that this stock-out had been caused by Covid-19-induced delays in international cargo shipments and shutdowns in countries of origin of the vaccines. There were also concerns in some districts that if the Covid-19 situation persisted for much longer, other vaccines would start to run out:
“We are soon going to run out of OPV and PCV if we don’t get new consignments. We are told that the ship that is carrying vaccines is stuck on the ocean somewhere.” District level Key Informant
By the time of completion of this evaluation the situation had not changed much.
Generalisability of findings While the findings from our evaluation provide detailed insights into the immunization program's financing and service delivery in Zambia during the COVID-19 pandemic, there is a recognition that these findings might not directly translate to other contexts. The specific socio-economic conditions, health infrastructure, and governmental responses in Zambia create a unique scenario that may differ significantly from other regions. However, the lessons learned about the flexibility of health financing, the adaptability of service delivery in crisis situations, and the strategic redirection of resources are universally relevant. These insights can contribute to a broader understanding of managing health programs in low and middle-income countries facing public health crises, suggesting a framework for resilience and adaptability that could be tailored to different regional or global contexts.
Implications for Equity The prioritization of high-density areas over remote locations in the distribution of immunization services, as necessitated by limited resources and increased demands due to COVID-19, brings to light significant equity issues within health service delivery. This strategy, while efficient in terms of resource utilization and reaching large populations, potentially exacerbates existing disparities in health access. Children in remote and underserved areas, who are already disadvantaged, face greater risks of being unvaccinated or under-vaccinated. A more profound exploration of these equity considerations is crucial to understanding the full implications of crisis-induced service adaptations. It is essential to develop strategies that not only address immediate health threats but also ensure that equity in health care access is not further compromised. Future policy directions should aim to establish mechanisms that maintain an equitable distribution of health services, especially in crisis scenarios, ensuring that the most vulnerable populations are not neglected.
Limitations
Our study primarily focuses on the immediate impacts of the COVID-19 pandemic on immunization service delivery and financing within the specified timeframe. A significant limitation is the lack of longitudinal analysis that would allow for the tracking of the recovery of immunization services post-pandemic and the assessment of the long-term effectiveness of the recommendations implemented. Future research should consider conducting follow-up studies to monitor these aspects over an extended period, providing a more comprehensive understanding of the sustained impacts and recovery processes associated with such global health crises.
CONCLUSION
One of the fundamental concerns, when pandemics such as Covid -19 hit resource-poor health systems, is that routine services get overlooked, starved of resources and ultimately strained. In this paper, we provide evidence that the spread of Covid-19 in the country poses challenges on many aspects of the national immunisation programme. Although the pandemic has not claimed as many lives as originally predicted, its negative effects on aspects of the Zambia immunisation systems have been significant. The need to fight Covid-19 created a competition over scarce resources between Covid-19 and routine services, including immunisation. Immunisation service delivery has been affected by constrained demand and restrictions on the supply-side. Further, there is evidence that immunisation human resources have been significantly adversely affected by increased workload and resultant stress.
RECOMMENDATIONS
Using routine data through the HMIS, the programme should closely monitor how Covid-19 is affecting immunisation service delivery, especially in remote areas. Government should assess the cost implication of Covid -19 on immunisation service delivery at subnational level. Government should develop clear protocols and provide associated technical support to districts and facilities for how to deliver immunisation services under Covid-19 conditions. An expenditure review is recommended to examine the financial impact of Covid-19 on the immunisation programme. Even after Covid-19 has subsided, the immunisation programme will need to re-invest into information, education and communication (IEC), and social mobilisation in order to re-engage with communities about Covid-19 and immunisation.
DECLARATION OF CONFLICTING INTERESTS
The Authors declare that there is no conflict of interest.
REFERENCES
- CSA. Zambia Demographic and Health Survey 2018. Central Statistics Agency; 2018.
- Gavi. Evaluation of the Zambia Immunisation Programme - Second Report.pdf>. https://www.gavi.org/our-impact/evaluation-studies/full-country-evaluations: Gavi; 2021.
- Gavi. Zambia Gavi Full Country Evaluation Report 2017-2018. https://www.gavi.org/our-impact/evaluation-studies/full-country-evaluations: Gavi; 2018.
- WHO, UNICEF. Progress and challenges with sustaining and advancing immunisation coverage duiring the Covid-19 pandemic. 2020.
- Brenzel L, Young D, Walker DG. Costs and financing of routine immunization: Approach and selected findings of a multi-country study (EPIC). Vaccine. 2015;33 Suppl 1:A13-20.
- WHO. World Health Organisation EPI Review Guidlines 2017.
- Gavi. Gavi Zambia Full Country Evaluation Report 2016. https://www.gavi.org/our-impact/evaluation-studies/full-country-evaluations: Gavi; 2016.
- Gavi. Evaluation of the Zambia Immunisation Programme - First Report, 2019. https://www.gavi.org/our-impact/evaluation-studies/full-country-evaluations: Gavi; 2019
- Feldhaus I, Schutte C, Mwansa FD, Undi M, Banda S, Suharlim C, et al. Incorporating costing study results into district and service planning to enhance immunization programme performance: a Zambian case study. Health Policy Plan. 2019;34(5):327-36.
- Gavi. Zambia Gavi Full Country Evaluation Report 2015. https://www.gavi.org/our-impact/evaluation-studies/full-country-evaluations. : Gavi; 2015.
- Dolan SB, Alao ME, Mwansa FD, Lymo DC, Bulula N, Carnahan E, et al. Perceptions of factors influencing the introduction and adoption of electronic immunization registries in Tanzania and Zambia: a mixed methods study. Implement Sci Commun. 2020;1:38.
- MOH. Zambia Joint Appraisal 2014. 2014.
- MOH. Zambia Joint Appraisal 2017. 2017.
- Gavi. Final Gavi Health Systems Strengthening Baseline Report_Final_20 March 2020.pdf. 2020.
- Griffiths UK, Bozzani FM, Chansa C, Kinghorn A, Kalesha-Masumbu P, Rudd C, et al. Costs of introducing pneumococcal, rotavirus and a second dose of measles vaccine into the Zambian immunisation programme: Are expansions sustainable? Vaccine. 2016;34(35):4213-20.
- MOH. EPI, PIE, and Surveillance ReviewRepor, Zambia 2014. 2014.
- MOH. Zambia_2015 EVM_Final Report. 2015
- MOH. Zambia Joint Appraisal 2016. 2016.
- MoH. Zambia EPI-Optimisation Initiative. 2017
- Schütte C, Kinghorn A, Chansa C, Marinda E, Teresa Guthrie, Banda S, et al. Costing and Financing Analyses of Routine Immunization in Zambia. 2014.
- Abakporo U, Hussein A, Begun JW, Shippee T. Knowledge, Beliefs and Attitudes of Somali Men in Olmsted County, Minnesota, U.S., on the Human Papillomavirus Vaccine and Cervical Cancer Screening: January 17, 2015. J Immigr Minor Health. 2018;20(5):1230-5.
Medical Journal of Zambia, Vol 51, 1
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.