Epidemiological profile of childhood cancer at the Lubumbashi University clinic in the Democratic Republic of Congo
Criss Koba Mjumbe
Department of Public Health, University of Lubumbashi, Lubumbashi, Democratic Republic of Congo.
School of Public Health, University of Lubumbashi, Lubumbashi, Democratic Republic of Congo.
Desiré Mashinda Kulimba
School of Public Health, University of Kinshasa, Kinshasa, Democratic Republic of Congo.
Oscar Luboya Numbi
Department of Public Health, University of Lubumbashi, Lubumbashi, Democratic Republic of Congo.
School of Public Health, University of Lubumbashi, Lubumbashi, Democratic Republic of Congo.
Department of Paediatrics, University of Lubumbashi, Lubumbashi, Democratic Republic of Congo.
Diane Balimo Muantama
Rosalind Franklin Laboratory, Leamington Spa, United Kingdom
Robert Lukamba Mbouli
Department of Paediatrics, University of Lubumbashi, Lubumbashi, Democratic Republic of Congo.
Chadrack Kabeya Diyoka
School of Public Health, University of Lubumbashi, Lubumbashi, Democratic Republic of Congo.
Benjamin Kabyla Ilunga
School of Public Health, University of Lubumbashi, Lubumbashi, Democratic Republic of Congo.
DOI: https://doi.org/10.55320/mjz.51.1.465
Keywords:Cancer, Children; profile, epidemiology, Lubumbashi
ABSTRACT
Background: Cancers in children under 17 years of age have specific epidemiological and management characteristics. The objective of this study was to determine the epidemiological profile of childhood cancers in Lubumbashi.
Methodology: A cross-sectional descriptive study was conducted in the University Clinics of Lubumbashi from 2018-2019. Data collection was carried using a statistical form with a number of parameters.
Results: In this study, 99 of the 3024 cases of children who visited the paediatric ward during the study period were diagnosed with cancer, a prevalence rate of 3.27%. Only (71.7%) of the cases had consulted a general practitioner at the first sign of illness. Retinoblastoma being the first childhood cancer with 29.3%, followed by kidney tumours (23.2%), lymphomas (13.1%) and leukaemias (12.1%) all combined forms. 87.9% had easy access to chemotherapy. Among these, (28.7 %) had chemotherapy and surgery with a curative aim. Childhood tumours show a remission in (20.7 %), 35.6 % of deaths and almost (27.6 %) remain under background treatment.
Conclusion: Diagnosis and early treatment continue to be crucial in reducing mortality among children suffering from cancers.
INTRODUCTION
Cancer is a real health problem worldwide.[1,2] It is one of the most common causes of death in adults.[3] However, it is relatively rare in children under the age of 15[4] and accounts for only 1 to 4% of tumours in the population.[5] Cancer accounts for one in ten deaths around the world.[6,7] Cancer has become a public health problem in the developing world, having long been considered a scourge in the first world countries. According to the International Classification of Childhood Cancer the most common diagnosis in children under the age of 15 are leukaemia (34 %), brain tumours (23 %) and lymphoma (12 %).[6] Acute lymphoblastic leukaemia, astrocytoma, neuroblastoma, Non-Hodgkin's lymphoma and nephroblastoma are the most common single diagnosis.[8] The forecasts for 2030 indicate a 50% increase in cancer rates, with 15 million new cases per year and an annual fatality rate of 10 million in all age groups.[5] In 2022, China had approximately 4.82 million cases with 3.21 million deaths, whilst United States recorded 2.37 million cancer cases with 640 thousand deaths.[9] Ghana recorded a 1.4% increase in new cases whilst Rwanda had 10% rise.[10] Mortality decreases significantly in developed countries and remains high in developing countries.[7] In the coming decades, cancer will surpass infections and parasitic diseases as the leading cause of morbidity and mortality.[11] ful to determine in the years to come the prevalence of cancers in Lubumbashi, the risk factors, the mode of treatment and the survival in particular for the most frequently encountered cancers. This requires systematic and prospective data collection. This study was designed to determine the epidemiological profile of hospitalised paediatric cancers and to propose the re-launch of a national cancer registry at the Lubumbashi University Clinics (CUL).
METHODOLOGY
From January 2018 to December 31, 2019, a transversal descriptive study was conducted at CUL. The study focused on 99 patients with childhood cancer who visited the paediatric oncology unit. We prospectively evaluated the selected patients from our cohort of 99 cancer children who met the inclusion criteria following: a diagnosis retained at the level of the oncology unit after paraclinical or histological examinations, the informed consent of the parents or guardians who signed for them to participate in the study.
The data was collected using a study form with several elements: age, sex, age at the onset of the first signs of the disease and family history. The socio-economic level has been categorized into three levels: low, medium and high according to the classification of Traissac et al.[12] In order to define coherent entities, a grouping of the different types of cancers was carried out according to the location of the tumour as defined by the International Classification of Childhood Cancer, 3rd Revision (ICC3).[6] The paraclinical diagnosis of the tumour has established based on the operational definition of the CUL Anatomy Pathology Unit. We calculated crude incidence rates (CRIs) in the two age groups of young children (0-9 years) and adolescents (9-17 years), estimated by relating observed cases to person-years calculated from approximate annual demographic data for Haut-Katanga provided by the Lubumbashi Bio Statistical Institute. The data were entered using Excel software and analysis was performed using STATA software version 12.1 (STATACORP LP, TX, USA).
Ethical considerations The study was approved by the Lubumbashi University Medical Ethics Committee (UNILU/CEM/135/2018). The data used in this study do not contain personal information. All parents of children with cancer have been given an explanation of study aims and principles. They were informed in writing of their consent for participation in the trial. The Declaration of Helsinki was followed during the study.
RESULTS
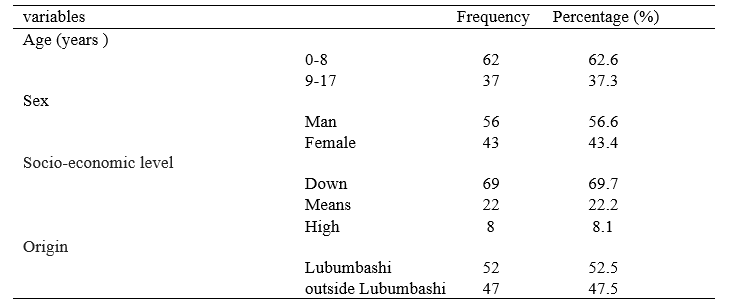
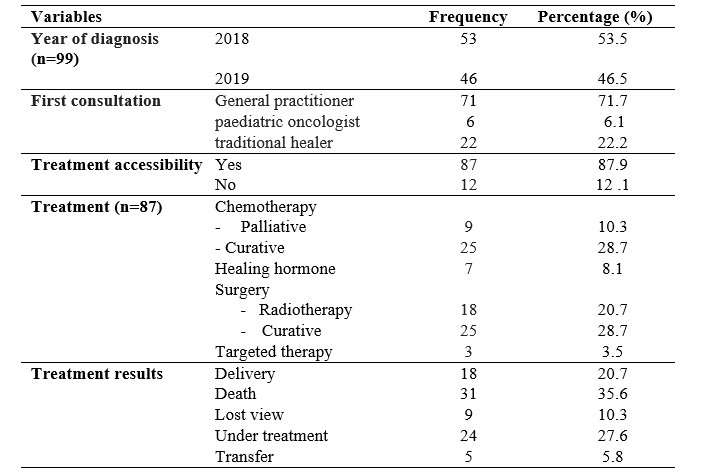
Sociodemographic Characteristics Of a total of 3,024 cases of children who had consulted the paediatric department during the study period, we recorded 99 cases of childhood cancers combined that is 3.72 % of total hospitalizations, males accounting to 56.6% against 43.4% females. In 2018, there were slightly more cases than in 2019 with 53 cases (53.5%) and 46 cases (46.5%) respectively the mean age was 5.67 ± 3.85 years, varying between 8 months - 17 years.
52.2% of the patients resided in Lubumbashi and the remainder of the cases came from other provinces and other countries. 71 children (71.7 %) had consulted a general practitioner at first contact and among them, twenty-two (22.22%) had also consulted a traditional healer or seen before the medical consultation (Table 1).
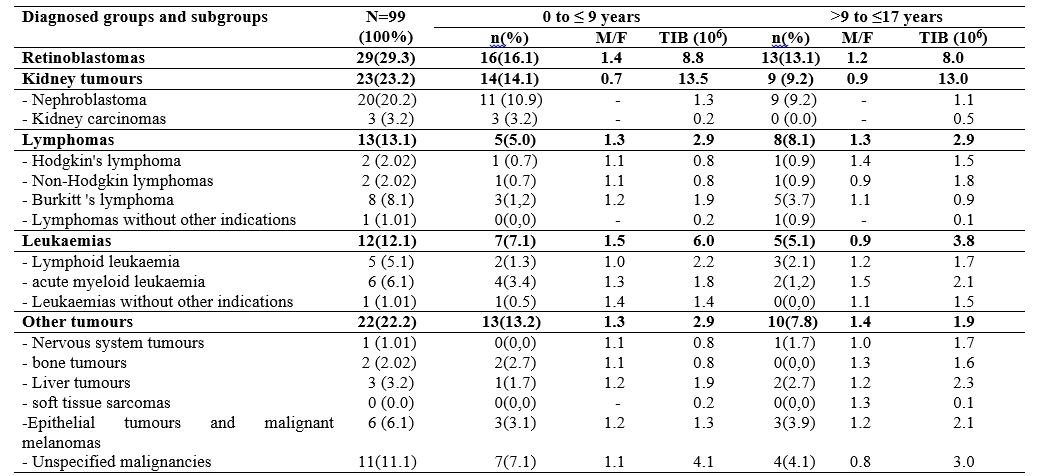
It is time to diagnose and extend the disease In both age groups, the most common tumours were retinoblastoma found in 29 cases (29.3%). Kidney tumours take second place with 23 cases (23.2%) followed by lymphomas and leukaemia of all forms with 13 cases (13.1%) and 12 cases (12.1%), respectively, as well as the other types of cancer observed in 22 cases (22.2%) (Table 2).
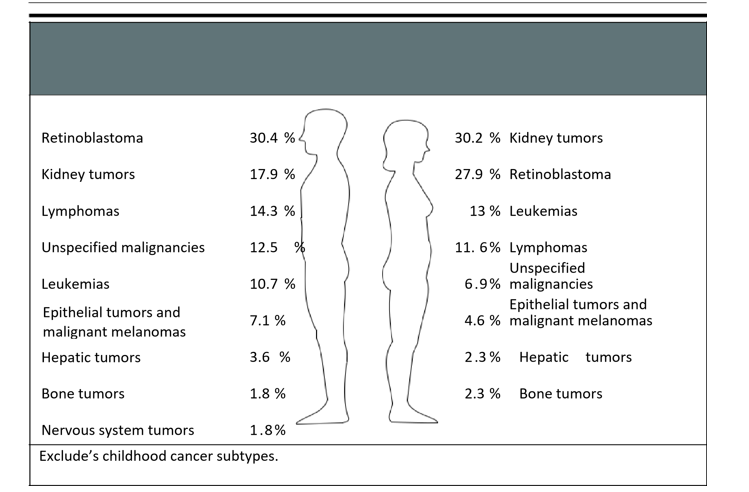
In male children the most common cancers were Retinoblastoma (30.4%), Kidney tumours (17.9%) and lymphomas (14.3%). On the other hand, among girls, the most frequent cancers were kidney tumours (30.2%), retinoblastoma (27.9%), and leukaemia (13%) (Figure 1).
12.1% of patients did not have easy access to treatment, whilst (87.9%) had easy access to chemotherapy. Among these (28.7 %) chemotherapy and surgery with a curative aim and (3.5 %) targeted therapy. In their evolution after starting treatment during the period of our study, childhood tumours show a remission in (20.7 %) and almost (27.6 %) remain under background treatment. It was noted that a significant number of patients (10.3%) lost sight of and discontinued treatment. The number of deaths recorded were 35.6 % (Table 3).
DISCUSSION
Cancer is an abnormal cell proliferation that escapes regulatory mechanisms, invading and destroying the tissues in which they develop, capable of early dissemination in the body in children, and likely to recur after treatment.[13] Due to the lack of national cancer registration in most developing countries, data on cancer epidemiology and mortality are only expressed as relative frequencies.[14] We found a prevalence 3.27 % (99 cases) of childhood cancer in Lubumbashi. The number of cases per year (53.5 % in 2018 and 46.5% in 2019) in our study was lower than in the literature in general and particularly in the capital of the DRC.[15]
In fact, our hospital is a hospital-university structure of the Province of Haut Katanga. The average age reported was (3.41-5.47years). In Africa, South of the Sahara, the mean age is 4.3- 6.7slightly higher than the age in our region.[16,17] The highest prevalence is among children aged 0-8 years, accounting for 55.6% of cases. They're about 10 years younger than patients in the developed world, but about the same age as patients in the developing world. A young population could foster this. Factors such as infection and poor hygiene predominate. The prevalence reported in this study does not represent all cases of childhood cancer.
We observed a male predominance with a sex ratio of 1.3. According to Steliarova-Foucher et al.[4] , this strong masculine representation is explained by the social impact of cancer on the male subject in an African environment, who should be responsible for the family rather than the girl. This study found a slightly lower male/female sex ratio than those found in Algeria and France[14,15] but was consistent with that found by Robert et al. in Kinshasa.[18]
In Africa, childhood cancer is still too often stigmatized due to ignorance of the disease or often late diagnosis and beliefs surrounding the disease. Childhood cancer is often viewed as mystical, and a significant number of households in our community first brought children to traditional practitioners.
In our study, the cancers commonly encountered in our environment were retinoblastoma, which alone accounted for 29 (29.3%), kidney tumours of 23 (23.2%) in the second position, lymphomas and leukaemias of all forms combined had a total of 13 (13.2%) and 12 (12.1%) respectively. Studies in the Congo Brazzaville and Kinshasa have shown a predominance of retinoblastoma (approximately 30%) [10]. Looking at the distribution of childhood cancers according to sex in our study, males had retinoblastoma as the most common type of cancer (30.4 %) followed by kidney tumours (17.9%) and lymphomas (14.3%). On the other hand, females, suffered from Kidney tumours (30.2 %), Retinoblastoma (27.9%) and leukaemias (13%). There are cancers associated with factors other than the most incriminated factor in embryonic development by comparing it to developed countries. Other tumours may be related to lifestyle. Nervous system cancers are also relatively less common. This can be explained by a lack of state-of-the-art equipment (brain imaging) in our environment and also by a very small number of qualified personnel for the identification of an early and certain diagnosis. These results are similar to those of other developing countries[19] like Abidjan (Côte d'Ivoire), Niamey (Niger), Ibadan (Nigeria), and Gambia.[15,20,21]
The lymphomas prevalent in Lubumbashi are in third place with a significant number of Burkitt lymphomas (8.8 % of NLL), which occupies the 1st rank among the different types of lymphoma. Uwizeye et al in Rwanda found that Burkitt's lymphoma was rare in Rwanda.[22] The most common childhood cancers are non-Hodgkin's lymphoma (33.15 %) and nephroblastoma (9.84%).[23] This situation is different from our series. It is probably because in our community the families consulted more for Burkitt than for the case observed in Rwanda.
A good number of children (28.7 %) had received chemotherapy and surgery with a curative aim during the period of our study. We recorded (35.6 %) a number of deaths. These results are almost similar to studies carried out in Africa[20] , but stay very different from studies conducted in developed countries where mortality rates for childhood cancers are falling significantly.[23]
This could be due to a delay in diagnosis, a lack of qualified personnel for care, a lack of specialized oncology units, and also to the lack of access to care which remains a heavy burden for most households.
Study Limitation The results of this epidemiological study of cancer in children only include data from children who visited the cancer unit at the University Children's Hospital in Lubumbashi during the period of our study, but do not represent all children with cancer in the community. Future research, including data from the DRC National Registry of Paediatric Cancer will provide a more complete and accurate picture of the burden of this disease in the population and a better understanding of the prevention or delay of morbidity, disability and death.
CONCLUSION
This study established the hospital epidemiological profile of childhood cancer in Lubumbashi. Early diagnosis and early treatment continue to be crucial in reducing mortality among children with these diseases. As the majority of other cases are underdiagnosed, the prevalence reported in this study does not represent all cases of childhood cancer. The mortality rate is still very high and many children have lost sight. The study also highlights the need to properly manage the registration of cases in a specific cancer registry, which is lacking in the DR Congo for good epidemiological monitoring. Detailed research is needed to better understand the epidemiology of cancer in Lubumbashi town.
Abbreviations
CUL Lubumbashi University Clinics ICCC3 International Classification of childhood cancers 3rd Edition CRI crude incidence rates CEM Medical Ethics Committee UNILU University of Lubumbashi DRCongo Democratic Republic of the Congo
DECLARATIONS
Acknowledgements Thanks to the ENAGO agency for the English translation.
Funding There were no external funds for this research.
Getting the data and materials The datasets produced/analysed in this study can be found in the [Epidemiological profile of childhood cancer] repository, [10.6084/m9.figshare.22121360]
Ethics approval and consent to participate None.
Competing interests Authors report having no competing interests. But the abstract of this paper was presented at the 55th Congress of the international society of paediatric oncology as a publication topic: AS05SIOP Scientifc Program/AS05.r with interim findings. The poster’s abstract was published in “Poster Abstracts” Paediatric Blood & Cancer in the Wiley Online Library : DOI: 10.1002/pbc.30748. Volume 70, Supplement 8, November 2023.
Consent for publication None.
Authors’ contributions All authors read and approved the final manuscript to supervision. CKM, CKD, RLM and MN. study concept and design, CKM, CKD, MN and BKI. data collection, CKM, DB and CKD. contributed to data analysis, data interpretation, and drafting of the original manuscript, CKM and CKD.contributed to data curation, CKM, DB and CKD. contributed to writing-review and editing, BKI, DMK and OLN. final manuscript for critical revision and approval.
REFERENCES
- Kaatsch P, Haaf G, Michaelis J. Childhood malignancies in Germany: methods and results from a national register. Eur J Cancer 1995; 31A:993-9.
- Kaatsch P, Rickert CH, Kohl J, Schz J, Michaelis J. Data epidemiological based on the population on the tumors brain in children Germans. Cancer 2001; 92:3155–64.
- Steliarova-Foucher E, Kaatsch P, Lacour B, et al. Quality, comparability and methods of analysis of childhood cancer data in Europe (1978-1997): report of the automated childhood cancer information system project. Eur J Cancer 2006; 42:1915–51.
- Steliarova-Foucher E, Coebergh JW, Kaatsch P, Pritchard-Jones K, Stiller C, editors. Cancer in children and adolescents in Europe. Eur J Cancer 2006; 42:1913–2190.
- Parkin DM, Kramarova E, Draper GI, et al. International incidence of childhood cancer. IARC Scientific Publication, vol. II. Lyon: International Agency for Research on Cancer; 1998. 144.
- Kramárová, E., Stiller, C.A., 1996. The international classification of childhood cancer. Int. J. Cancer 68, 759–765.
- Capocaccia R, Gatta G, Magnani C, Stiller C, Coebergh JW. Childhood cancer survival in Europe 1978-1992: the study EUROCARE. Eur J Cancer 2001; 37:671–816.
- Kaatsch, P., 2010. Childhood Cancer Epidemiology. Treat cancer. Rev Cancer in Childhood 36, 277–285. https://doi.org/10.1016/j.ctrv.2010.02.003
- Xia, C., Dong, X., Li, H., Cao, M., Sun, D., He, S., Yang, F., Yan, X., Zhang, S., Li, N., Chen, W., 2022. Cancer statistics in China and the United States, 2022: patterns, trends and determinants. Chin. Med. J. (Eng.) 135, 584–590. https://doi.org/10.1097/CM9.0000000000002108
- Stefan, DC, 2015. Childhood cancer distribution patterns in Africa. Paediatrician. 61, 165–173. https://doi.org/10.1093/tropej/fmv005
- Stefan, DC, 2015. Childhood cancer distribution patterns in Africa. Paediatrician. 61, 165–173. https://doi.org/10.1093/tropej/fmv005
- Traissac, P., Delpeuch, F., Maire, B., Martin-Prével, Y., Cornu, A., Trèche, S., 1997. Construction of a synthetic index of the economic level of households in nutritional surveys. Examples of application in the Congo. Epidemiol Public Health Tour 45, 114–15.
- Stiller CA, Marcos- Gragera R, Ardanaz E, et al. Geographical patterns of childhood cancer incidence in Europe, 1988-1997. Report of the Childhood Cancer Automated Information System Project. Eur J Cancer 2006; 42:1952–60.
- Coebergh JWW, Reedijk AMJ, de Vries E, et al. Incidence and survival of leukaemia in children and adolescents in Europe between 1978 and 1997. Report of the Childhood Cancer Automated Information System Project. Eur J Cancer 2006; 42:2019–36.
- Kaatsch P, Mergenthaler A. Incidence, trends temporal and regional variation of childhood leukaemia in Germany and Europe. Radiat Protection Dosim 2008;132 :107-13.
- Peris-Bonet R, Martinez-Garca C, Lacour B, et al. Tumours of the central nervous system in childhood- incidence and survival in Europe (1978-1997): report of the automated childhood cancer information system project. Eur J Cancer 2006; 42:2064–80.
- Mjumbe CK, Bora BK, Numbi OL, Mwenze PK, Tshamba HM, Ilunga BK, et al. Psychosocial lived experience of parents of children diagnosed with cancer in Lubumbashi. J Cancer Ther. 2020;11 (12):749.
- Robert, L.M., Ben, M.B., Atteby, Y., Théo, K.A., Aléine, B.N., Pierre, B., Gabrielle, C.B., Laurence, D., Alexia, S., Rokia, B.-C., 2020. Knowledge of Retinoblastoma by Healthcare Professionals in Sub-Saharan Africa: Survey Performed in the Republic of Côte d’Ivoire and the Democratic Republic of the Congo. Int. J. Clin. Oncol. Cancer Res. 5, 34.
- Kaatsch P, Steliarova-Foucher E, Crocetti E, Magnani C, Spix C, Zambon P. Temporal trends in cancer incidence in European children (1978-1997): report of the automated cancer information system project infant. Eur J Cancer 2006; 42:1961–71.
- Steliarova-Foucher E, Stiller C, Kaatsch P, et al. Geographical patterns and temporal trends in cancer incidence and survival in children and adolescents in Europe since the 1970s (the project ACCIS): a epidemiological study. Lancet 2004; 364:2097–105.
- Sankila R, Martos -Jiménez MC, Miljuis D, Pritchard-Jones K, Steliarova-Foucher C, Stiller C. Geographical comparison of cancer survival in European children (1988- 1997): report of the automated information system project on childhood cancer. Eur J Cancer 2006; 42:1972–80.
- Tapela , NM, Mpunga , T., Hedt- Gauthier, B., Moore, M., Mpanumusingo , E., Xu, MJ., Nzayisenga , I., Hategekimana , V., Umuhizi , DG., Pace, LE. , Bigirimana , JB ., Wang, J., Driscoll , C., Uwizeye , FR., Drobac , PC, Ngoga , G., Shyirambere , C., Muhayimana, C., Lehmann, L., Shulman , LN., 2016. Pursuing Equity in Cancer Care: implementation, challenges and preliminary conclusions of a public reference centre against cancer in rural areas of Rwanda. BMC Cancer 16, 237. https://doi.org/10.1186/s12885-016-2256-7
- Ndahindwa, V., Ngendahayo, L., Vyankandondera, J., 2012. Epidemiological and anatomopathological aspects of cancers in university hospital centres (CHU) in Rwanda. Rwanda Med. J. 69, 40–49.
Medical Journal of Zambia, Vol 51, 1
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.