The Practice of informed consent among patients undergoing major surgeries at a regional referral hospital in Dar es Salaam Tanzania
Mary Mathias
Department of Otorhinolaryngology, Temeke Regional Referral Hospital, Dar es Salaam, Tanzania
Zephania Saitabau Abraham
Department of Surgery, School of Medicine and Destiny, University of Dodoma, Dodoma, Tanzania
DOI: https://doi.org/10.55320/mjz.51.1.457
Keywords:Informed consent, major surgery, medicolegal, National Guideline for Safe Care Standards
ABSTRACT
Background: Informed consent for surgery has become a critical component in surgical practice. Patients learn about the diagnosis (disease condition), management options, surgical interventions (indications, risks, and benefits) and then agree to receive treatment through a well-prepared informed consent. In Tanzania, the National Guideline for Safe Care Standards explains that health facilities should have a clearly defined process of getting informed consent and in surgical procedures, it directs that the consent form should state the type of anesthesia and procedure to be performed on the patient. Increased medico-legal litigation and the desire to provide patients with more say concerning their own treatment has highlighted the need to strengthen quality of informed consent in surgical procedures. This study was designed to determine the practice of informed consent among patients undergoing major surgery in the surgical department at a regional referral hospital in Dar es Salaam, Tanzania.
Methods: A hospital based descriptive cross-sectional study was conducted at Temeke Regional Referral Hospital in Dar es Salaam Tanzania involving seventy-one patients aged above 18 years who were admitted in surgical wards and had undergone major surgical procedure from July to August 2022. Convenient sampling technique was utilized to recruit the study participants. Data collection was done by using a questionnaire in Swahili and analyzed using the statistical package for the social sciences (SPSS) computer software version 23.0.
Results: A total of 71 patients were enrolled; 53 (74.6 %) were male and 18 (25.4%) were female. There were more emergency surgeries 37(52.1%) than elective surgeries 34 (47.9%). Most participants (69%) had their consent being taken few hours before surgery and on the operating table. Majority received pre-anesthetic evaluation while at the operating table (56.3%). Information about surgery was delivered by surgeons who performed surgery in 39.4 % of the participants. On the other hand, 84.5% of the participants knew the diagnosis prior surgery, 60.6% reported to have been informed about the benefits of the intended surgery while only 1.4% were informed about the alternative of the surgery. Only 26.9% were informed on the consequences of not undergoing surgery; 38% were given time to ask questions, but only 40.8% were involved in making decisions for the intended surgery. Majority of the study participants (84.5%) knew the type of anesthesia to be used and only 8.5% were informed about possible risks for the intended anesthesia and surgery.
Conclusion: This study highlighted areas of inadequacy in surgical informed consent practice at Temeke Regional Referral Hospital. Informed consent for surgery was mostly taken few hours before surgery and while on the operating table, pre-operative evaluation mostly was done while patients were on the operating table, surgery risks and alternative to treatment options were poorly communicated. Therefore, every aspect of surgical informed consent should be well communicated to patients and given adequate time for decision making. Also, for elective cases surgical informed consent should be taken a day before surgery to allow patients make their own decisions without undue coercion.
INTRODUCTION
Informed consent for surgery has become a critical component in surgical practice. It is an essential step in helping patients be aware of the disease condition, possible management options and the associated consequences of the treatment options.[1] Patients learns about and understand the purpose, benefits and potential risks of a medical or surgical intervention and then agree to receive the intended treatment.[2,3] There are specific requirements for what has to be disclosed to patients and for the accompanying documentation. Informed consent may be used for different purposes in different contexts: legal, ethical, or administrative.[3] Informed consent forms the ethical foundation for the modern practice of shared decision making and patient-centered care. Although consent can be implied or expressed orally, consent for surgical procedures requires recorded documentation.[4-8]
For an informed consent to be valid the patient must be competent to take the decision; have received sufficient information to decide without coercion. Consent should begin with a brief explanation of the clinical diagnosis, planned operation, including the anesthetic agent involved. It is wise to describe what the patient may expect to experience during surgery, if under a local, regional, or general anesthetic agent. Sufficient information to make a decision should also include an explanation of the risks and benefits involved, any alternative treatments, the risks and benefits of non-operative management. The goal is to inform patients well enough to allow them to make balanced decisions. The information must be basic and in a language the patient is familiar with. Little information fails to inform, while too much information may be counter-productive and only lead to confusion.[4-5] When physicians and patients take medical informed consent seriously, the patient-physician relationship becomes a true partnership with shared decision-making authority and responsibility for outcomes. [8-11]
In Tanzania, the National Guideline for Safe Care Standards explains that health facilities should have a clearly defined process of getting an informed consent. It goes further explaining all parts, and how consent should be attained. In surgical procedures, it directs that the consent form should state the type of anesthesia and procedure to be performed to a specific patient. Current guideline states that the person obtaining a consent must either be capable of performing the procedure himself or herself; or have received specialist training in advising patients about the procedure.[12]
It is prudent to obtain informed consent for surgery at the time of listing in clinic when the risks and benefits are often explained. The patient will feel comfortable to proceed, and hence will not be acting under coercion.[9]
The study done in Italy to ascertain whether written informed consent inform surgical patients, found that 90.9% of those who reported to have read the written informed consent provided, judged it to be clear, 52.0% had it a day before the surgery at the earliest and 41.1% received it some hours or immediately before the procedure. Most attention was given to the diagnosis and the type of surgical procedure, which was communicated respectively to 92.8% and 88.2% of the patients.[1]
A study done in Greece on patients’ perception of quality of pre-operative Informed consent found all patients to be aware of their underlying diagnosis and the reason for surgery and 58.4% of the patients stated that they had not been informed about other possible therapeutic choices.[13]
Siddiqui et al in Pakistan condcuted an audit of informed consent in surgical patients at a university teaching hospital that found that 8.5% cases had their consent not taken, 38% of the surveyed patients acknowledged that they understood the information given to them while 66% were informed about the type of anesthesia.[14]
Decision making is a very important aspect of informed consent. A study in Nigeria on the attitude towards informed consent found that more than 70% of the respondents irrespective of educational status would not leave all decisions about their healthcare to the doctor. More than 85% of those with tertiary education would prefer an informed consent to be obtained by the operating surgeon while only 33.8% of those with no formal education would prefer the informed consent to be taken by the operating surgeon.[16]
The study done in a teaching hospital in Southern Ethiopia on surgical informed consent (SIC) found: 18.4% of the respondents to have reported that the surgeon performing the operation had offered SIC, while 36.6% of respondents could not recall who had offered SIC. However, 8.3% of respondents received SIC service while already on the operation table for their procedure. Majority of the respondents (73.9%) were informed about the availability of alternative treatment options.
Additionally, 88.3% of the respondents were not informed about the type of anesthesia to be used during surgery and related complications.[17]
A study done in Uganda showed that 80% of the participants knew the indication for their surgery and only 23.7 % were able to identify the person who obtained their consent.[18]
Increased medico-legal litigation and the desire to provide patients with more say concerning their own health has highlighted the need to strengthen quality of informed consent in surgical procedures. In low income developing countries, a few researchers have explored the practice of surgical consent pre-operatively.[9,19]
The aim of this study was to evaluate the practice of informed consent among patients undergoing major surgery in surgical department at a regional referral hospital in Dar es Salaam Tanzania.
METHODS
The study was a hospital based prospective descriptive cross-sectional study conducted at Temeke regional referral hospital in Dar es Salaam, Tanzania. It involved patients admitted to the surgical ward for major surgical procedures from 1st July to 31st August 2022. Convenient sampling technique was used to recruit study participants. All surgical patients who were 18 years or above and underwent major surgeries and consented to participate in the study. Data collection was done by using a questionnaire in Swahili. The study protocol followed the ethical guidelines of the 1975 Helsinki Declaration. Approval of the study was given by hospital ethical clearance committee (ethical approval number; TRRH/RSC/9/8/52). Data was processed using the statistical package for social sciences computer software version 23.0.
RESULTS
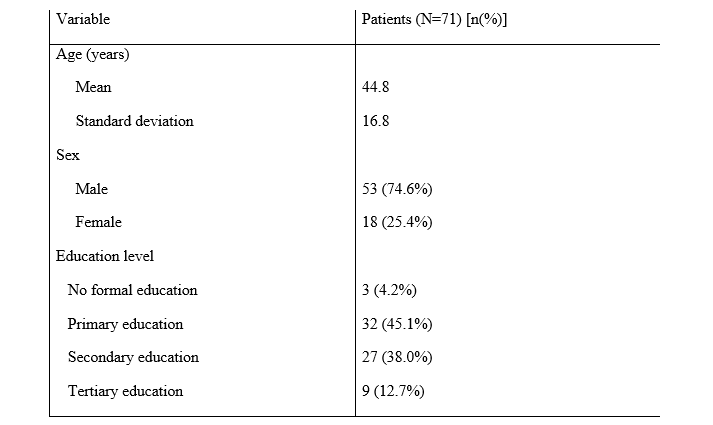
A total of 71 patients were enrolled: 53 (74.6 %) were male and 18 (25.4%) were female. The mean age was 44.8 years with standard deviation of 16.8. All patients were interviewed, and their hospital record card observed for presence of written informed consent. One participant could not remember whether or not consent was taken and his file was also observed not to have a written informed consent (Table 1).
Majority of the participants were from Temeke district (71.8%) while only 5.6% were from outside Dar es Salaam. Moreover, 45.1% of the study the participants had primary educational level (Table 1).
Regarding the nature of surgery, 37 (52.1%) were emergency and 34 (47.9%) were elective cases. Also 69% of the respondents reported their consent to have been taken few hours before the surgery and on the operating table while 16.9% reported their consent to be taken day before surgery.
About the venue for pre-anesthetic evaluation, 23% was done at anesthesia clinic before admission, 12.7% was done in the ward, 4.2% in both anesthesia clinic and in the ward, 56.3% in the operation table and 2.8% were not sure about the venue where pre-anesthetic evaluation was done.
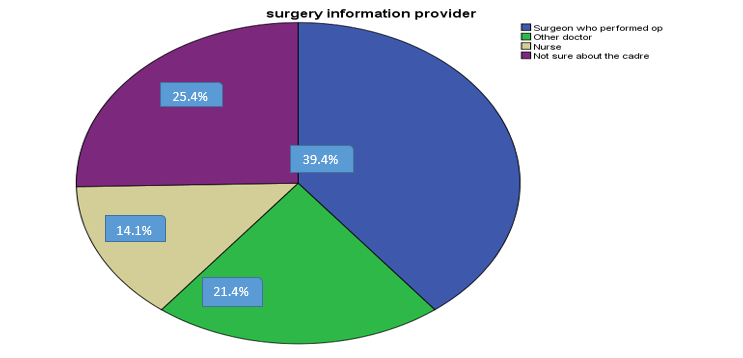
The surgeon who performed the operation provided information about the surgery in 39.4% of the patients while 25.4% were not sure about the cadre of the person who provided information about surgery, and the rest received information from other health cadres (Figure 1).
Majority of the patients knew the diagnosis prior surgery (84.5%). Majority of the study participants (60.6%) reported to have been informed on the benefits of the intended surgery while 1.4% was given alternative to surgery and only 26.9% were told about consequences of not undergoing surgery.
On the other hand, 38.0 % of the respondents reported to have been given time to ask questions, while 40.8% were involved in making decisions for the intended surgery. Majority of the study participants (84.5%) knew the type of anesthesia used while only 8.5% were told about accompanied surgery risks.
DISCUSSION
This study showed that majority of the patients (84.5%) knew the diagnosis or nature of their illness prior surgery. This corresponds to other studies in which majority of patients received explanation of the indications for their surgery prior their procedures as shown in the study done in Ethiopia where 85.9% of the study participants were told about the diagnosis [2] and the study in Greece where all patients knew their underlying diagnosis and reason for surgery [13] . Similarly, the study in Uganda found 80% of the patients to have been given explanations on the indication of their surgery[18] , and the study done in Ethiopia found 87.3% of the study participants to have known the reason why they had to undergo surgery.[20]
Current guideline states that the people obtaining consent must either be capable of performing the procedure themselves; or have received specialist training in advising patients about the procedure. This study revealed that 39.4 % of the study participants received the explanation of surgery indication from the surgeons. This is higher than the number of patients informed by surgeons in the study done by Million in Southern Ethiopia where only 18.4% received information from surgeon and 36.6% could not recall.[17] Despite the fact that there were more number of elective surgeries than elective in both studies, the differences in the findings can be due to the fact that the other study had gynecology and obstetrics participants who are mostly under care of nurses. Another study by M. Asharib et.al also revealed the number of informed consents taken by consulting surgeon to be lower (40.6%) than that was taken by residents/house officers 59.4%).[21] On the other hand, 23% of the study participants could not identify the person giving informed consent to surgery as explained in the study done by Joseph Ochieng et al.[18]
Time and venue for taking informed consent raised concern in this study, in which it revealed that 69% of the respondents gave their consent few hours before surgery and while on operation table. This number is higher compared to other studies where 41.1% of participants received the informed consent some hours or immediately before the procedure in the study done by Erminia et.al in Italy[1] while only 8.3% of the respondents received their informed consent while already in operating table in study done by Million et.al in Southern Ethiopia[17] . The difference in the findings may be contributed by variety of study population where it included clients from nine hospitals in the study by Erminia et al. However, the study by Million et al could have more higher number of patients having their consent taken few hours prior surgery and in operating table due to the nature of clients who were only obstetrics and gynecology cases and having more emergency cases than elective but has not been the case. Taking consent few hours prior surgery and when the patient is already on the operating table may affect patient decision-making as well as creating anxiety.[9]
Type of anesthesia used is also a very important component of an informed consent. In this study 84.5% of the respondents knew the type of anesthesia to be used while only 8.5% were aware about the risks related to the intended surgery. Other studies also show majority of patients knew the type of anesthesia to be used. Siddiqui Faisal et.al in Pakistan found 66 % of the participants knew the type of anesthesia used [14] and the study done by Tamire in Ethiopia where 56.1% of the patients were informed about type of anesthesia used.[22] These studies recruited both elective and emergency participants who had already undergone surgery with similar age groups. This can be the reason for similarities in the findings. However, these findings differ from the study done by Million et.al where majority of the patients (88.3%) were not informed about type of anesthesia to be used.[17] The number of patients knowing the risks related to surgery and anesthesia is much higher in other studies.[2,23] Most procedures for obstetrics and gynecology are done under spinal anesthesia and most patients are aware of it. It can be the reason for this high number who were not informed about type of anesthesia to be used since some practitioners tend to practice routinely.
In this study only 1.4% of the study participants were given alternative treatment options, 60.6% knew about surgery benefits and 26.9% were aware about the consequences of not undergoing surgery. This is different from the study done by Chane et.al in which a good number of patients were given information about alternative treatment options, benefits of surgery and consequences of not undergoing surgery.[2] The differences in these findings may be caused by differences in study settings; where one was conducted at a tertiary hospital where quality and accountability is higher compared to that of a regional hospital. Regarding the recall of the nature of disease condition and the nature of planned procedure versus recall of risks involved in the planned procedure and alternative treatment options, the former was found to be well recalled than the latter in some studies.[24,25]
Moreover, 38% of the study participants in our study were given time to ask questions and 40.1% were involved in decision making. This number is slightly lower than in the study done by Ochieng et al where 56.1% of participants had their questions being answered prior surgery.[18] The study settings and differences in sample size can contribute to the discrepancy in these two studies, where one was done in three different university teaching hospitals with large sample size (371 participants) while our study was done at a regional referral hospital with small sample size (71 participants).
The limitation of this study was the presence of only one reliable theatre room during the study period hence prioritized surgeries to be conducted were obstetric cases and emergency surgical procedures at the regional referral hospital.
CONCLUSION
This study highlighted areas of inadequacy in surgical informed consent practice at Temeke regional referral hospital. Informed consent for surgery was mostly taken few hours prior surgery and while on operating table, pre-operative evaluation mostly was done while patients were on operating table, surgery risks and alternative to treatment options were poorly communicated. Every aspect of surgical informed consent should be well communicated to patients and given adequate time for decision making and the consent should be taken a day before surgery to allow patients to make their own decisions without coercion.
DECLARATIONS
Funding source: None
Conflicts of interests: We declare no conflicts of interests.
REFERENCES
- Agozzino E, Borrelli S, Cancellieri M, Carfora FM, Di Lorenzo T, Attena F. Does written informed consent adequately inform surgical patients? A cross sectional study. BMC medical ethics. 2019 Dec;20(1):1-8.
- Chane W, Birhanu B, Suga Y. Quality of informed consent among patients who underwent major surgical procedure in a Tertiary Care Hospital, Addis Ababa, Ethiopia. Open Access Surgery. 2020 May 6:27-33.
- Jahan F, Roshan R, Nanji K, Sajwani U, Warsani S, Jaffer S. Factors affecting the process of obtaining informed consent to surgery among patients and relatives in a developing country: results from Pakistan. EMHJ-Eastern Mediterranean Health Journal. 2014 Sep 1;20(9):569-77.
- Hall DE, Prochazka AV, Fink AS. Informed consent for clinical treatment. Cmaj. 2012 Mar 20;184(5):533-40.
- Hanson M, Pitt D. Informed consent for surgery: risk discussion and documentation. Canadian Journal of Surgery. 2017 Feb;60(1):69.
- Bernat JL, Peterson LM. Patient-centered informed consent in surgical practice. Archives of Surgery. 2006 Jan 1;141(1):86-92.
- Wood F, Martin SM, Carson‐Stevens A, Elwyn G, Precious E, Kinnersley P. Doctors’ perspectives of informed consent for Non‐Emergency surgical procedures: a qualitative interview study. Health Expectations. 2016 Jun;19(3):751-61.
- Lawal YZ, Garba ES, Ogirima MO, Dahiru IL, Maitama MI, Abubakar K. The doctrine of informed consent in surgical practice. Annals of African Medicine. 2011;10(1).
- Anderson OA, Wearne IM. Informed consent for elective surgery—what is best practice?. Journal of the Royal Society of Medicine. 2007 Feb;100(2):97-100.
- Joolaee S, Faghanipour S, Hajibabaee F. The quality of obtaining surgical informed consent: Case study in Iran. Nursing ethics. 2017 Mar;24(2):167-76.
- Paterick TJ, Carson GV, Allen MC, Paterick TE. Medical informed consent: general considerations for physicians. InMayo Clinic Proceedings 2008 Mar 1 (Vol. 83, No. 3, pp. 313-319). Elsevier.
- The United republic of Tanzania G. Guidelines N, Safecare FOR, For S, Hospitals HC. First Edition , Version 1 March 2014 THE UNITED REPUBLIC OF TANZANIA First Edition , Version 1 March 2014. 2014;(March):2014.
- Falagas ME, Akrivos PD, Alexiou VG, Saridakis V, Moutos T, Peppas G, Kondilis BK. Patients' perception of quality of pre-operative informed consent in Athens, Greece: a pilot study. PLoS One. 2009 Nov 26;4(11):e8073.
- Siddiqui FG, Shaikh JM, Memon MM. An audit of informed consent in surgical patients at a university hospital. Journal of Ayub Medical College Abbottabad. 2010 Mar 1;22(1):133-5.
- Jawaid M, Farhan M, Masood Z, Husnain SM. Preoperative informed consent: is it truly informed?. Iranian journal of public health. 2012;41(9):25.
- Agu KA, Obi EI, Eze BI, Okenwa WO. Attitude towards informed consent practice in a developing country: a community-based assessment of the role of educational status. BMC medical ethics. 2014 Dec;15:1-8.
- Teshome M, Wolde Z, Gedefaw A, Tariku M, Asefa A. Surgical informed consent in obstetric and gynecologic surgeries: experience from a comprehensive teaching hospital in Southern Ethiopia. BMC medical ethics. 2018 Dec;19:1-9.
- Ochieng J, Buwembo W, Munabi I, Ibingira C, Kiryowa H, Nzarubara G, Mwaka E. Informed consent in clinical practice: patients’ experiences and perspectives following surgery. BMC research notes. 2015 Dec;8:1-6.
- Wismayer R. Informed consent for surgical care in East Africa. Journal of Advances in Medicine and Medical Research. 2021 Dec 13;33(23):80-4.
- Lemmu B, Megersa A, Abebe E, Abebe K. Knowledge and perception of Ethiopian surgical patients to informed consent practice for surgical procedures. Open Access Surgery. 2020 Sep 7:65-70.
- Arshad MA, Omar N, Amjad Z, Bashir K, Irfan M, Ullah I. Perceptions and practices regarding the process of obtaining informed consent from surgical patients at a tertiary care hospital. Annals of Medicine and Surgery. 2022 Jan 1;73:103195.
- Tamire T, Tesfaw A. The practice of obtaining informed consent for elective surgery and anesthesia from patients’ perspective: An institutional based cross-sectional study. Clinical Ethics. 2022 Mar;17(1):57-62.
- Osime OC, Okojie O, Osadolor F, Mohammed S. Current practices and medico-legal aspects of pre-operative consent. East African medical journal. 2004 Oct 22;81(7):331-5.
- Brezis M, Israel S, Weinstein-Birenshtock A, Pogoda P, Sharon A, Tauber R. Quality of informed consent for invasive procedures. International Journal for Quality in Health Care. 2008 Oct 1;20(5):352-7.
- Nnabugwu II, Ugwumba FO, Udeh EI, Anyimba SK, Ozoemena OF. Informed consent for clinical treatment in low-income setting: evaluating the relationship between satisfying consent and extent of recall of consent information. BMC Medical Ethics. 2017 Dec;18:1-8.
APPENDIX I:
INFORMED CONSENT AT TEMEKE REGIONAL REFERRAL HOSPITAL
Greetings! We are Dr. Mary Mathias and Dr Zephania Saitabau Abraham working on this study with the aim of assessing the practice of informed consent among patients undergoing major surgeries at Temeke regional referral hospital.
Purpose of the study
This study aims at assessing the practice of informed consent among patients who undergo major surgery in surgical department in this hospital. We need this information to identify the gaps between ideal practice and current practice at our hospital so that we can improve the quality of care.
How to participate
The interviewer will be asking you questions while and she/he will be filling the questionnaire on voluntary basis
Risks
We do not more than minimal risk by participating in this study.
Confidentiality
We would like to assure you that all the information that you will provide will remain confidential and will be used for study purpose only. No one will be allowed to see or go through your answers except the principal investigator only.
Right to withdraw and alternatives
Taking part in this study is purely voluntary. You can stop participating at any time even if you have already given your consent. Refusal to participate or withdrawal will neither affect the quality of your current treatment nor involve a penalty.
Consent
I have read and understood the explanation of the study. I accept to participate in the study. Name and signature of the patient/guardian.......................................... Date...................................... For more information or clarification, you may contact Dr. Mary Mathias (0714911414) or Dr Zephania Saitabau Abraham (0765878209)
APPENDIX II:
Title: The practice of informed consent among patients undergoing major surgeries at a regional referral hospital in Dar es Salaam Tanzania
Serial no..................... 1. Age ......... 2. Sex a) male b) female 3. Address a) Temeke b) Other districts in Dar es Salaam c) Outside Dar es Salaam 4. Marital status a) Single b) Married c) Divorced 5. Occupation a) Employed/self-employed (b) Farmer (c) Business 6. Education level a) no formal education b) primary education c) secondary education d) college/university 7. Type/nature of surgery a) Emergency b) Elective 8. Who provided you information about surgery? ( a) Surgeon who performed the operation (b) Other Doctor ( c) Nurse d) Not sure about the cadre 9. When was the consent taken a) On the surgery day b) Days before surgery (c) Few hours before surgery/on operation table 10. Where did you have anesthesia pre-operative evaluation? (a) At anesthesia clinic before admission (b) In the ward after admission (c) In anesthesia clinic and in the ward (d) In operating table (e) Not sure 11. Did you know the diagnosis or nature of illness prior surgery? (a) Yes (b) No 12. Did you know who was going to performed surgery? (a) Yes (b) No 13. Do you know type of anesthesia used? (a) Yes (b) No 14. Do you know/were you told about benefits of surgery? (a) Yes (b) No 15. Do you know/told any risk related to your surgery (a) Yes (b) No 16. Were you told consequences of not undergoing surgery? (a) Yes (b)No 17. Were you given adequate time for making decision about surgery? (a)Yes (b) No 18. Were you given adequate time to ask questions? (a) Yes (b) No 19. Were you told any alternatives to surgery? (a) Yes (b) No Observation (for researcher) 20. Check for written informed consent in patient file (a) Present (b) improvised (c) absent 21. Check the contents of the informed consent i. Diagnosis a) Yes b) No c) NA ii. Who will perform surgery a) Yes b) No c) NA iii. Nature of surgery a) Yes b) No c) NA iv. Type of anesthesia a) Yes b) No c) NA v. Benefits of surgery a) Yes b) No c) NA vi. Risks of surgery a) Yes b) No c) NA vii. Alternatives to surgery a) Yes b) No c) NA viii. Consequences of not undergoing surgery a) Yes b) No c) NA
Medical Journal of Zambia, Vol 51, 1
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.