Rehabilitation outcome following pericardiectomy in pericarditis complicated by recurrent pericardial effusion and cardiac tamponade: a case report from Zambia
Sporah Chisha
National Heart Hospital, Lusaka, Zambia.
Stanely Zulu
National Heart Hospital, Lusaka, Zambia.
Benson Kazembe
National Heart Hospital, Lusaka, Zambia.
Jane Kabwe
National Heart Hospital, Lusaka, Zambia.
DOI: https://doi.org/10.55320/mjz.51.1.456
Keywords:Cardiac Rehabilitation, Recurrent pericarditis, Pericardiectomy.
ABSTRACT
Background: Recurrent pericarditis is the most problematic complication following acute pericarditis and occurs in 20–50% patients of all age groups. Clinical manifestations vary and range from asymptomatic to life-threatening. Despite normally good prognoses, it ensues a negative impact on patients. Cardiac rehabilitation (CR) has demonstrated the cardinal role in the management of patients who undergo pericardiectomy, yet no specific rehabilitation protocols are available for reference.
Case Presentation: A 27-year-old man presented with pericardial effusion and cardiac tamponade in recurrent pericarditis. His prior admission history included chest pains for 3 months. He was diagnosed with tuberculous pericarditis (TBP) and commenced Anti-tuberculosis Treatment (ATT) before referral. The patient complained of worsening difficulties in breathing, orthopnoea, cough, chest pains and had a significant history of spear-positive Pulmonary Tuberculosis (PTB) contact during childhood but was HIV-negative.
His physical examination revealed tenderness on the left chest and disuse atrophy in the left upper limb. Patient generally looked healthy with an average body build. His baseline spirometry and 6MWT scores were 68% and 250 meters. Patient had right lower lobe atelectasis associated with reduced air entry. He received a pre-operative regimen of chest physiotherapy and resistance exercises. Radical pericardiectomy was performed via midline sternotomy three weeks later. Post-operative physiotherapy commenced in the Intensive Care Unit (ICU) within 24 hours. Patient was transferred to the ward and discharged on day 8 with a prescribed physiotherapy home programme. On follow-up, the patient made incredible progress on the three reviews at 2 weeks, 3 months, and 1 year.
Conclusion: Our case demonstrates the cardinal role of exercise-based CR in patients undergoing pericardiectomy hence the need to establish a standardized exercise protocol and identify means to transform post-hospital care for cardiac disease patients.
INTRODUCTION
The majority cases of recurrent pericarditis in developed countries are idiopathic, however, emerging evidence in Africa cited TB as the most common cause [2,10,11] . The rising incidence of TBP in sub-Saharan Africa is attributed to the Human Immunodeficiency Virus (HIV) epidemic however, there is a paucity of literature regarding the prevalence of pericardial diseases in Zambia [4,7,11] .
Pericardiectomy results in greater risks of post-operative pulmonary complications such as secretion retention, atelectasis, pneumonia and may impact on patient’s Quality of Life (QoL) and lead to death [2,9,10] . Modern studies have acknowledged the cardinal role of augmented physiotherapy in patients undergoing pericardiectomy, nonetheless, no specific rehabilitation guidelines are available posing a major rehabilitation challenge [1,5,6] .
CASE PRESENTATION
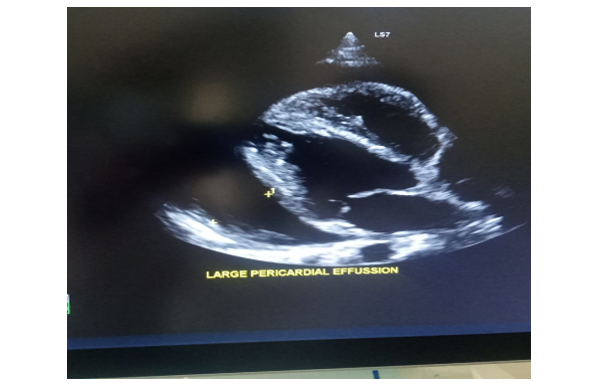
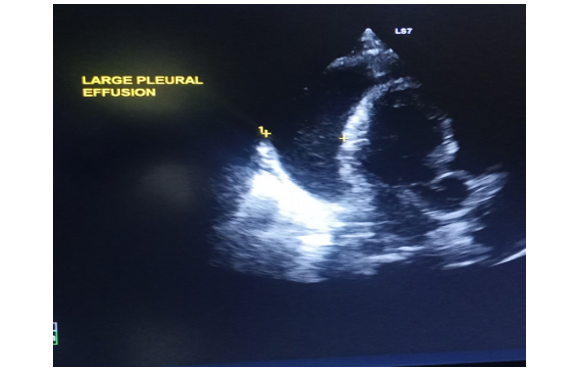
A 27-year-old man was referred to our hospital with recurrent tuberculous pericarditis, complicated by effusion and cardiac tamponade. He presented with breathing difficulties, cough, and chest pains among other symptoms. He had a significant history of spear-positive PTB contact as a child but was HIV-negative. Patient elicited tenderness on the left chest and disuse muscle atrophy in the left arm. His baseline spirometry test was below average with an FEV1/FVC ratio of 68% and his 6MWT score was 250 meters. Pre-intervention Chest X-ray (figure 1) and Echocardiogram (figure 2) revealed a large pericardial effusion. We administered a pre-operative physiotherapy regimen which included, deep breathing exercises coupled with a dynamic exercise of standing on toes and sitting on a chair, respiratory muscle training using incentivized breathing exercises, stair climbing, stationary bicycle riding, and resistance exercises to the left arm with progressive incremental load. Patient underwent radical pericardiectomy three weeks later after several attempts of pericardiocentesis.
Post-operative physiotherapy treatment began in the ICU within 24 hours of extubation. Day 0 to 1 regimen included; ankle pumps, hand grip exercises, facilitated long sitting using a rope tied to the foot of the bed while supporting the incision site with a small pillow, percussions, coughing, huffing, and incentivized breathing exercises. We progressed to placing the patient in high sitting on the bed and performed active knee flexion and extension exercises on day 2. Progressive ambulation was also commenced beginning with standing, marching on the spot, and walking around the bed. The patient was very stable by day 4, he was able to walk independently and hence was transferred to the ward where rehabilitation continued. He was introduced to stair climbing and stationary bicycle riding to build his cardiopulmonary endurance on the fifth day and discharged on day 8.

DISCUSSION
Pericardiectomy risks secretion retention, atelectasis, and pneumonia. Recent evidence has shown significant benefits of exercise-based CR as it targets respiratory muscles, endurance, and overall physical function [3,8,12] . Despite inadequacies in data on the prevalence of tuberculous pericardial diseases in Africa, modern literature shows an increase in the disease due to the HIV pandemic. A case series from the Western Cape in South Africa, found a prevalence of tuberculous pericarditis (TBP) at 69.5% among cases referred for diagnostic pericardiocentesis, giving enough evidence to support the rising incidence of TBP [4,9,11] . Our patient, however, was HIV-negative contrasting the findings.
The patient did not develop any pulmonary complications following a prescribed regimen despite presenting with an atelectatic area and moderate pulmonary function. The findings concur with studies that postulated deep breathing to have reduced atelectatic area and improved lung function [3,6,12] . Our patient presented with poor physical function and disuse atrophy in the left arm, therefore, we incorporated resistance exercises into the regimen [1,5,8] . This was the first case we managed using an improvised exercise-based CR programme. Our patient tolerated the newly established exercise regimen well and showed notable improvement.
We noted a meaningful difference in the distance covered during the 6 MWT and spirometry test scores on the three follow-up stages suggesting that our patient benefitted from the exercise program outlined for him. Patient covered 350, 430, and 500 meters on the 6MWT and scored 70%, 75%, and 89% on spirometry tests at 2 weeks, 3 months, and 1 year respectively.
CONCLUSION
Our case report reaffirms the merit of CR in the management of patients undergoing pericardiectomy.
REFERENCES
- Bracewell NJ, Plasschaert J, Conti CR et al. Cardiac rehabilitation: Effective yet underutilized in patients with cardiovascular disease. Clin Cardiol. 2022; 45:1128–1134.
- Chiabrando JG, Grizzard JD, Montecucco F et al. Management of Acute and Recurrent Pericarditis. JACC State of the Art Review. J Am Coll Caediol. 2020 Jan; 7;75(1):76-92.
- Dsouza FV, Amaravadi SK, Samuel SR et al. Effectiveness of Inspiratory Muscle Training on Respiratory Muscle Strength in Patients Undergoing Cardiac Surgeries: A Systematic Review with Meta-analysis. Annals of Rehabilitation Medicine. 2021 May; 45(4)264-73.
- Elliot AM. Luo N, Tembo G et al. Impact of HIV on tuberculosis in Zambia: A Cross-sectional Study. BMJ. 1990 Sep;1;301(6749):412-5.
- Fabrin S, Soares N, Regalo SCH et al. Evolution of patients with heart disease after cardiopulmonary rehabilitation program: case-report. Fisioterapia Em Movimento. 2017; 30(1),169–176.
- Heutinck JM, de Koning IA, Vromen T et al. Exercise-based cardiac rehabilitation in stable angina pectoris: a narrative review on current evidence and underlying physiological mechanisms. Neth Heart J. 2024 Nov; 32:23–30.
- Kabwe L, Lakhi S, Kalinichenko S, Mulenga L. Prevalence of Subclinical Cardiovascular Disease in Health HIV Infected Patients at the University Teaching Hospital in Lusaka, Zambia. Medical Journal of Zambia. 2016; 1:12-23.
- Kirkman DL, Lee DC, Carbone S. Resistance-exercise for cardiac rehabilitation. Prog Cardiovasc Dis. 2022 Jan; 70:66-72.
- Lazaros G, Vlachopoulos C, Lazarou E, Tsioufis K. New Approaches to Management of Pericardial Effusions. Curr Cardiol Rep. 2021 Jul;1;23(8):106.
- Maria M, Gabriel BO, Nicolae B et al. Diagnosis and management of pericardial effusion. Journal of Mind and Medical Sciences: 2020 Jun;4(7),148-155.
- Mayosi BM, Wiysonge CS, Ntsekhe M et al. Clinical characteristics and initial management of patients with tuberculous pericarditis in the HIV era: The investigation of the management of pericarditis in Africa (IMPI Africa) Registry. J BMC Infectious diseases. 2006 Jan; 6(2);2334-6.
- Moradian ST, Heydari AA, Mahmoudi H. What is the Role of Preoperative Breathing Exercises in Reducing Postoperative Atelectasis after CABG? Rev Recent Clin Trials. 2019;14(4):275-279.
Medical Journal of Zambia, Vol 51, 1
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.