Mini-laparotomy versus conventional laparotomy in emergency general surgery: a prospective study from a second-level hospital in Zambia
Sergiy Karachentsev
Roan Antelope General Hospital, PO Box 90297, Luanshya, Zambia
Phone: +260212515010
Fax: +260212671151
Womba Kadochi
Roan Antelope General Hospital, PO Box 90297, Luanshya, Zambia
Phone: +260212515010
Fax: +260212671151
DOI: https://doi.org/10.55320/mjz.51.1.448
Keywords: Small-incision laparotomy, standard laparotomy, emergency general surgery, length of hospital stay
ABSTRACT
Background: Mini-laparotomy (ML) is one of the approaches aimed to reduce intraoperative stress and enhance recovery in surgical patients. The objective was to determine how safe and feasible ML access is in emergency surgery.
Methods: This prospective, two-group, parallel active-controlled study evaluated adult patients operated on for acute abdominal conditions. Patients explored with the use of ML and those having standard laparotomy (SL) access formed two arms of the study. The ML was defined as open surgical access of less or equal 12 cm. Length of hospital stay and 30-day morbidity/mortality were primary endpoints. Secondary outcomes were operative time, estimated blood loss during the procedure, and postoperative pain control.
Results: Thirty-five patients were explored through ML, and 33 had an SL incision. The size of ML ranged from 6 to 12 cm, with the median being 10.5 cm. Employment of ML was associated with reduced length of stay (p=0.008), shorter operative time (p=0.003), and minimised need for opioid analgesia (p=0.008); however, the difference in postoperative complications was not statistically significant (ML: 20% versus SL: 27%, p=0.48) and mortality was similar in both groups (6%).
Conclusion: Our data demonstrate that ML is a safe technique that could be used for the treatment of urgent abdominal conditions in selected patients. Having comparable postoperative morbidity with the SL approach, it might lead to reduced pain and enhanced recovery after the procedure.
INTRODUCTION
Despite continuous advances in perioperative care, emergency abdominal surgery still carries a substantial risk of in-hospital complications and death worldwide[1,2] . Metabolic response to intraoperative trauma is considered an important determinant of postoperative complications and the risk of death after major surgery[3,4] . To attenuate operation-induced stress and expedite patient rehabilitation, various mini-invasive methods have been developed[5,6] . Reduced in size laparotomy incision is one of these techniques, which could be applied for visceral general surgery and intraabdominal vascular surgery procedures[7-9] .
Our institution is a 164-bed second-level referral hospital operating as the main medical centre in the area with a population of around 200,000, and we have a quite heavy workload with acute care surgery. In our efforts to optimise the postoperative recovery of the patients, we have started practising a small-incision approach in selective abdominal procedures in 2020. However, the safety and feasibility of ML incision in emergency surgery remain unclear. Review of the recent literature revealed that 1) vast majority of studies in visceral surgery reported on the use of laparoscopic and actively implementing robotic techniques[10-12] , 2) most of the works are restricted by areas of appendicectomy, cholecystectomy and colon surgery with associated conditions[6,13,14] , 3) in emergency setting, open laparotomy remains the principal surgical approach[15,16] , 4) reports on laparoscopy in abdominal trauma are scarce and still divided on its diagnostic and therapeutic potential[17-19] , and 5) those studies assessed the efficacy of different explorative techniques reported comparable outcomes after laparoscopic methods and ML[5,6,20] .
In this study, we aimed to evaluate how safe and technically feasible ML is in emergency surgery. We hypothesised that the small-incision laparotomy might bring additional clinical benefits to patients in comparison with the standard surgical approach technique.
MATERIAL AND METHODS
The work was conducted according to the ethical principles of medical research disclosed in the Declaration of Helsinki with all respect shown for the privacy and confidentiality of the personal information of the participants. Permission to perform the study and to publish results was obtained from the Roan Antelope General Hospital Ethical Standing Committee (Ref No 01/21). All participants were fully informed of the research and their consent for enrolment in the study and permission for taking pictures and publication were obtained.
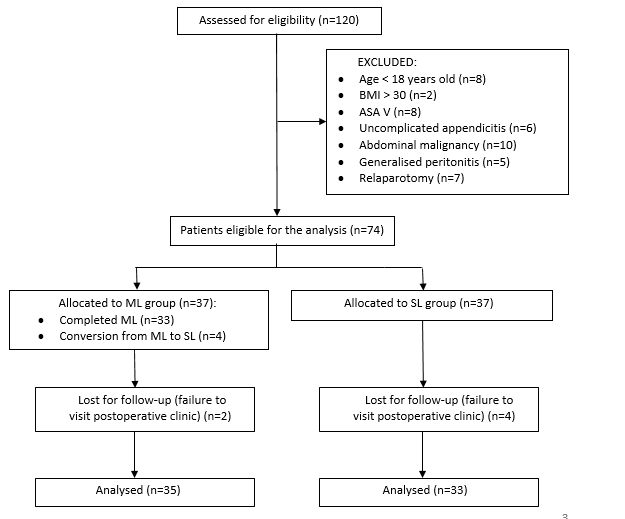
All consecutive patients operated on for urgent abdominal pathology from 03 December 2021 to 10 February 2023 were assessed for inclusion in this prospective two-group, parallel active-controlled clinical study. The inclusion criteria were as follows: 1) age > 18 years old, 2) Body Mass Index < 30, 3) American Society for Anaesthesiologists class I to IV. Patients under 18 years old were excluded from the study, as most standard abdominal incisions in children are of a small size. We did not include patients operated on for uncomplicated appendicitis for the same reason. Small incisions were not attempted in obese individuals with a Body Mass Index of above 30 due to reduced field of view and difficulties in manoeuvre in a deep operative wound. Patients who need a thorough inspection of the abdominal cavity or who may require mobilization of distant structures were also excluded from the study (Figure 1). To categorise eligible participants into study groups, an alternating allocation method[21] was used, and they were dichotomised based on alternate days of admission to the hospital.
To calculate sample size, we used a formula for cohort study with a two-sided hypothesis test estimating a significance level of 5% and the power of the study of 80%[22] . For the reference study, we have chosen a recent meta-analysis of case-control studies[23] comparing outcomes in mini-invasive and open surgery for intestinal obstruction.
Sample size = (2SD²(Zα/₂ +Zᵦ)²)/d²
SD – Standard deviation (from the reference study) Zα/2– Z value for the level of significance (type 1, or α, error) Zᵦ – Z value for the power of a study (type II, or β, error) d – effect size = difference between mean values (from the reference study)
Based on this analysis, we expected an effect size in the main outcome in our patients—length of hospital stay (LOS)—to be 5 days. According to the calculation, each arm should have at least 33 participants. Anticipating drop-outs during follow-up, we increased the sample size to 37 patients in each group.
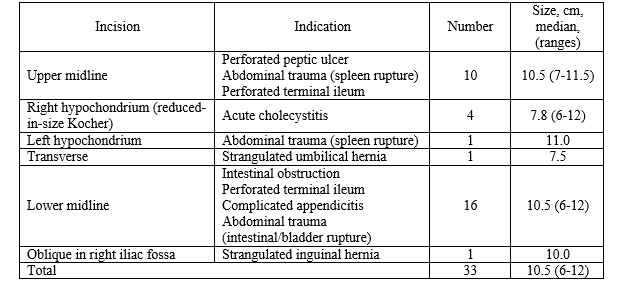
We defined ML as surgical approach with skin incision not exceeding 12 cm. The orientation and the length of the ML incisions are presented in Figure 2. We promptly converted the ML into a standard incision by extending the upper and lower edge of the wound in difficulties in intraabdominal visualisation and manipulation; however, in accordance with the methodology of the intention-to-treat principle[24] , these patients were retained in the originally assigned ML group. The surgical access in the SL cohort was achieved through a conventional midline laparotomy measuring from 13 to 22 cm.

Patients were treated in line with the concept of Enhanced Recovery After Surgery (ERAS)[25-27] , as much as our resources allowed (Supplementary Table). On admission, they received IV resuscitation and weight-adjusted doses of antibiotic, a nasogastric tube and urinary catheter were inserted when necessary. The physical status of patients was assessed by the American Society of Anaesthesiologists (ASA) classification[29] . Cases of acute pancreatitis were categorised according to the Revised Atlanta Classification[30] . The extent of injury in abdominal trauma victims was estimated by the revised Organ Injury Scale for solid organ injuries for the American Association for the Surgery of Trauma[31] , and Injury Severity Score (ISS)[32] . As diagnostic modalities, abdominal X-ray and Ultrasound were used routinely. The patients were operated according to their clinical needs. Operations were performed by two consultant surgeons and one senior registrar surgeon. The plan for the intervention was discussed in detail with an anaesthesiologist and the consensus was achieved in every case.
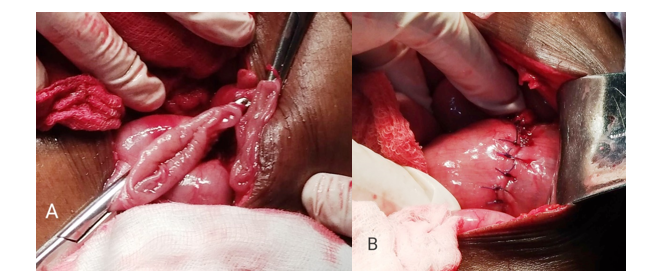
Gastrointestinal perforations were repaired by the application of interrupted slowly-absorbable sutures. To perform intestinal anastomosis, the hand-sewn technique was used, with one layer for the small bowel and two layers for the colon (Figure 3). Cholecystectomy was done by retrograde technique in both groups. At the end of the operation, layers of the abdominal wall were closed with a continuous slowly absorbable suture and the skin was sutured with interrupted sutures. Postoperative care included adequate pain control using Nonsteroidal Anti-inflammatory Drugs and opioid analgesics, early removal of nasogastric tube and urinary catheter, immediate commencement of the physiotherapy, early mobilization, and nutrition. The intensity of postoperative pain was assessed by the demand for opioid analgesics. Patients were followed up 30 days after discharge.
The primary outcomes were LOS and postoperative morbidity. LOS was calculated from the day of the operation. Morbidity was assessed according to Clavien-Dindo[33] . Mortality was determined as death following surgery during the hospital stay or within 30 days of the procedure, whichever is sooner[34] . Secondary outcomes included operating time (OT), estimated blood loss during the surgery (EBL) and postoperative pain control. OT and EBL were counted by a circulating theatre nurse and anaesthetist. Primary and secondary endpoints were compared between ML and SL subsets.
Descriptive statistics were employed to report the findings obtained. Continuous variables were presented as mean with standard deviation or median with interquartile ranges depending on the distribution of the data and analysed by t-test. Categorical data were expressed as frequency and percentage and assessed by chi-square analysis or Fisher exact test as appropriate. LOS was compared by log-rank test and presented graphically by Kaplan-Meier survival curves[35] . A p-value <0.05 was considered significant.
RESULTS
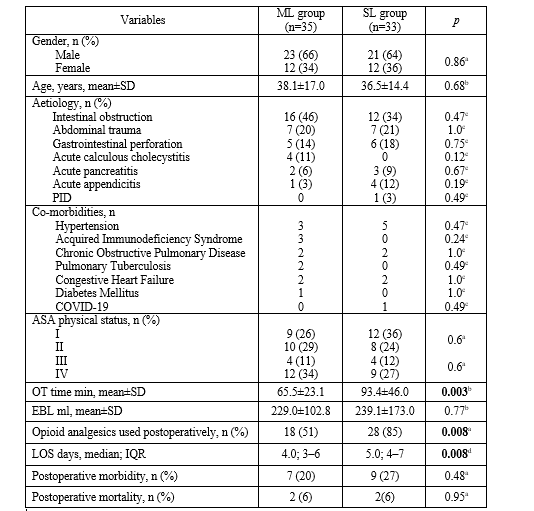
Out of 120 patients operated on for acute abdomen at the hospital during the study period, 68 participants were recruited with 35 in the ML arm and 33 in the SL arm. Demographics and clinical variables are presented in Table 1.
Indications for surgery were similar in both cohorts; however, it appeared that acute cholecystitis and intestinal obstruction were seen more often in the ML cohort, and complicated acute appendicitis was operated more frequently in the SL group. Characteristics of the ML incisions are presented in Table 2. Intestinal obstruction was the most common presentation in both groups and was caused by adhesions (ML: n=7, SL: n=6), volvulus (both ML and SL: n=6 each), strangulated hernia (ML: n=2), and intussusception of the jejunum caused by the tumour (non-Hodgkin’s lymphoma) (ML: n=1). Volvulus developed in the sigmoid colon (ML: n=5, SL: n=4), ileum (both ML and SL: n=1 each), in one patient from the SL cohort we encountered ileo-sigmoid volvulus when a loop of ileum was twisted around the base of the sigmoid colon. Peritonitis developed due to perforated peptic ulcer (ML: n=3, SL: n=2) or distal ileum (ML: n=2, SL: n=4), and complicated appendicitis (ML: n=1, SL: n=4).
 ML, mini-laparotomy, SL, standard laparotomy; n, number of patients; %, percentage; SD, standard deviation; IQR, interquartile range; NA, not applicable; PID, pelvic inflammatory disease; COVID-19, coronavirus disease 2019; ASA, American Society for Anaesthesiologists; OT, operating time; min, minutes; EBL, estimated blood loss; ml, millilitre; LOS, length of stay
aChi-squared test
bt test
cFisher exact test
dlog-rank test
ML, mini-laparotomy, SL, standard laparotomy; n, number of patients; %, percentage; SD, standard deviation; IQR, interquartile range; NA, not applicable; PID, pelvic inflammatory disease; COVID-19, coronavirus disease 2019; ASA, American Society for Anaesthesiologists; OT, operating time; min, minutes; EBL, estimated blood loss; ml, millilitre; LOS, length of stay
aChi-squared test
bt test
cFisher exact test
dlog-rank test
Abdominal trauma led to splenic laceration (ML: n=3, grade II: n=1, grade III: n=2; SL: n=2, grade II: n=1, grade III: n=1), bladder injury (ML: n=2, SL: n=2) and intestinal rupture (ML: n=2, SL n=1). Trauma was blunt except for two patients, one from each group, who sustained a penetrated stab injury. One trauma victim from the ML group sustained polytrauma with an ISS score of 22. In three trauma patients (ML: n=2, SL: n=1), associated chest and pelvis injuries were diagnosed, though with lower ISS scores ranging from 13 to 18. Natural history of disease complicated by the development of sepsis (ML: n=5, SL: n=6) and hypovolemic shock (ML: n=4, SL: n=3).
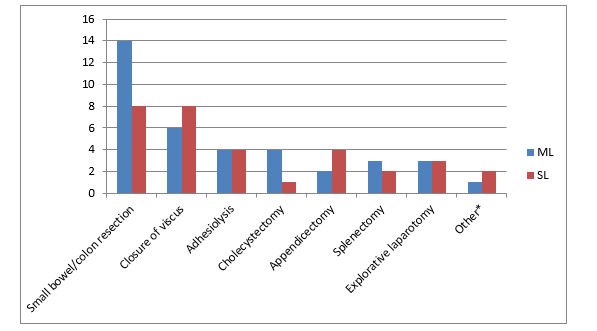
The procedures performed are depicted in Figure 4. When using the ML approach, manipulations were completed inside the peritoneal cavity in 26 patients, while in 9 cases the segment of the intestine was mobilised outside the abdomen by gentle traction. In 5 patients of this group, an ostomy through the separate skin incision was created as a part of the procedure (ileostomy n=2, sigmostomy n=3). In four cases, we extended the ML access to standard median laparotomy (conversion rate 11%): in two cases of intestinal obstruction caused by complex adhesions, in one patient with perforated terminal ileum and intraabdominal sepsis, and in one patient with penetrated thoracoabdominal trauma and injuries to the spleen and left kidney. Explorative laparotomy was done in acutely incarcerated umbilical hernia (ML: n=1), ruptured tubo-ovarian abscess (SL: n=1), and acute pancreatitis (2 patients in each group). The latter four patients were classified as moderately severe acute pancreatitis and were explored to rule out perforation peritonitis. One more patient with mild acute gallstone pancreatitis from the SL cohort was offered early cholecystectomy.
The time of the procedure ranged from 31 to 126 min in the ML group and from 40 to 210 min in the SL cohort, and the average was significantly shorter in the index group (65.5±23.1 min and 93.4±46.0 min, respectively, p=0.003, 95% CI 9.73 to 46.07). Nonetheless, blood loss during the surgery was similar in both groups (ML: 229.0±102.8 ml versus SL: 239.1±173.0 ml, p=0.77, 95% CI –58.33 to 78.53). Two patients from the ML group and three patients from the SL group needed a blood transfusion intraoperatively. It is not clear why the difference in OT between the two groups was so significant; however, it is evident that more time is needed to close the bigger wound, especially if it is twice as big.
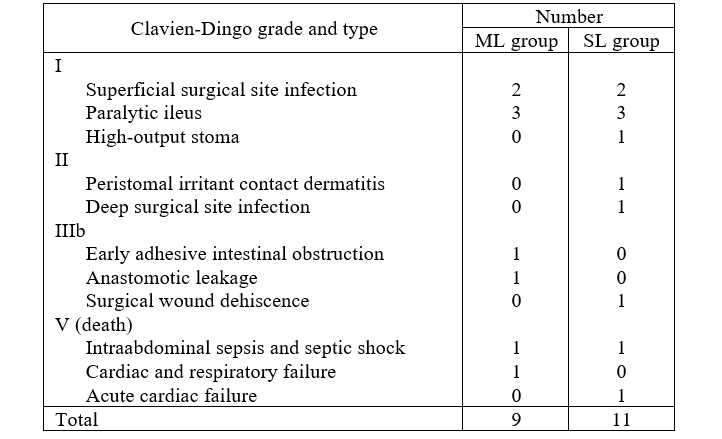
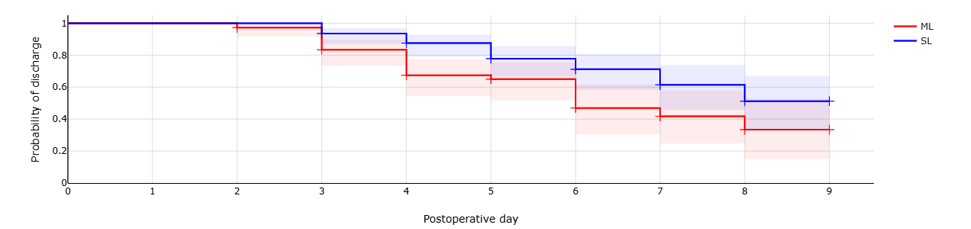
Postoperative complications were less frequent in the ML cohort, but the difference was not significant (Tables 1 and 3). Four patients died after operations, two in each group. Causes of death were recorded as follows: sepsis with septic shock (ML, n=1, female, sutured perforated ileum, leakage, relaparotomy via standard approach, ongoing peritonitis), refractory hypotension, and respiratory failure (ML, n=1, straightforward resection of ileum in adhesive intestinal obstruction with necrosis in a medically compromised patient of ASA class IV), colostomy retraction, faecal peritonitis, septic shock (SL, n=1). One patient of the SL cohort died with a sudden cardiovascular collapse on day 4 after an uncomplicated adhesiolysis procedure, and the cause of death remains unknown, as the autopsy was not performed. Cases of postoperative complications and deaths in the ML group were neither associated with missed intraabdominal pathology nor with insufficient exposure and difficulties in manipulations during the procedure. The hospital stay for survived patients was markedly shorter in the ML group (Table 1 and Figure 5).
DISCUSSION
We conducted this study to assess the feasibility of ML incisions in the emergency general surgery population. Analysis revealed that the ML is safe and practicable approach in selected patients with a low conversion rate and favourable short-term outcomes. There is no consensus in the literature about the definition of mini-laparotomy, and the length of the incision, characterised as ML, varies from 3 cm[36] to 18 cm[37] . In agreement with Wang et al.[38] , we defined the upper limit of the ML being 12 cm. With this size of the wound, gentle edge traction exposes the operative site sufficiently to perform a procedure, and, besides, it allows the surgeon to insert their hand into the abdominal cavity for tactile feedback. Most commonly, we used lower midline incision and found it sufficiently convenient to operate on different pathologies including, for example, sigmoid volvulus (Figure 3). In our opinion, manipulation with the distal part of the twisted sigmoid is technically easier with this approach. The second advantage is that midline incision can be easily converted into standard laparotomy in case of technical difficulties encountered. This approach for sigmoid volvulus was advocated in one study,[39] nonetheless, other orientations of ML access were described in the literature, namely vertical[40] , horizontal[41] , and oblique[36] incisions in the left iliac fossa.
To the best of our knowledge, there are no reports describing the application of ML in abdominal trauma. Laparoscopy was introduced to both penetrating and blunt abdominal injuries, but it is not widely used these days[17,42] . It has therapeutic potential, for example, in situations when non-operative management fails and at the same time the patient remains haemodynamically stable[19,43] , when the skill level and experience of a surgeon are sufficient to complete the procedure started laparoscopically[44] , and in “special” cases concerning the preferences of the patient[18] . However, laparoscopy in trauma is usually opposed to open exploration and performed in a situation of diagnostic uncertainty to avoid negative celiotomies[42,45] . In this study, ML was used in patients with abdominal trauma as a therapeutic procedure. The employment of the ML incision allowed a surgeon to do fast and easy access to the peritoneal cavity (which is essential in an emergency setting[46] ), promptly assess the intraabdominal situation and decide on further manipulations. In our series, six out of seven trauma cases were finished with a small incision when it was chosen as an initial technique.
While the advantages of ML are comprehensively described in the literature[7,9,39] , the challenges, and risks associated with this approach should not be underestimated. First, patients with intra-abdominal infections often present in the late stage with a non-specific clinical picture, and this could complicate the diagnosis-making process. This is especially true in resource-scarce settings with limited diagnostic modalities[1] . At the same time, when deciding to perform the procedure using the minimal approach, the operator must precisely locate the anatomical site of interest before the operation starts. Second, inside the small incision, the surgeon is restricted in freedom of manipulation and could find it difficult to properly visualize abdominal organs to reveal associated or unrelated pathology. Third, delivery of the intestinal loops to the outside of the abdominal cavity for manipulation through a small incision can lead to compression of the mesenteric root and subsequent venous congestion of the externalised intestine which we saw in two of our patients.
The following measures were undertaken to alleviate manoeuvres within the small operative area. Before the procedure, a 10 cm high pillow was placed underneath the patient’s back. It decreased the depth of the operative wound and expanded the field of view for the surgeon at the site of the operation. In cases of sigmoid volvulus, the overdistended loop was initially desufflated by a large bore needle which allowed the surgeon to deliver it easily through a small incision. It was recommended by van der Naald et al.[39] , and we found this manipulation highly effective. To prevent compression of the mesenteric vessels, we tried to perform manipulations within the abdominal cavity. Exposure of the bowel loops outside the abdomen should be limited in time unless the procedure involves the resection of the delivered intestine. Next, it is crucially important to maintain consistent and cooperative communication between the surgeon and the anaesthesiologist, as the appropriate level of anaesthesia can significantly alleviate manipulations within a limited operative space[26] . Due to the plasticity of the abdominal wall and good muscle relaxation, it is possible, for example, to perform splenectomy through an incision which is smaller in size than the organ removed (Figure 6).

Having a positive experience with ML, we are however confident that even with the optimal surgical technique the clinical benefits for the patient are not just from the reduction in the size of the incision. We think because patients of both groups were equally treated according to the principles of fast-track surgery, an effect size in LOS, albeit significant, appeared to be less than expected initially. Statistically speaking, ERAS components produced a negative confounding effect here underestimating the outcome of the exposure; nonetheless, they were not able to dilute the beneficial effect of the intervention.
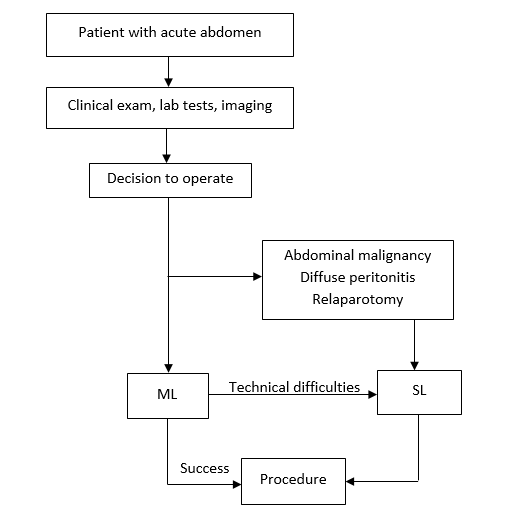
Therefore, ML can be considered optimal access in an environment where laparoscopic equipment or training is not yet available and as a viable alternative if the surgeon does not have enough experience with laparoscopy or when it is contraindicated for the patient. In this regard, we propose an algorithm for the selection of exploration method in patients with acute abdomen and trauma (schematically depicted in Figure 7). Of note, a decision to perform ML should be substantially grounded by careful weighting of both associated risks and expected benefits. Sound clinical judgment and sufficient surgical expertise are indispensable in selecting the optimal surgical approach, and the threshold for conversion to a standard laparotomy is to be low. It is vital that the standards of urgent surgical care are not impaired by choosing an ML exploration method. One should realize that making a small incision is not the goal of the management per sè, rather it is one of the available methods to perform the procedure in the most efficient and safe way to deliver optimal patient-centred care, and our findings confirm this.
Limitations
The results of the study should be interpreted with caution in the context of some considerations. The alternating assignment employed for the allocation of the patients to the groups can lead to selection bias[47] . On the other hand, it is an example of a systematic random sampling method, and thus, according to Ott and Longnecker[48] , it could provide a representative sample of a target population. Indeed, there is no reason to assume that there is a cyclic fluctuation of emergency admissions to the hospital within the week, and this notion is supported in the literature[49] . This technique is not uncommon for the evaluation of surgical treatment and can give more accurate evidence of an intervention effect than an observational design[24] . It is applied when practical considerations (for our study there were difficulties in randomisation of participants admitted urgently and a low-volume surgical hospital) and financial restrictions make performing a high-quality Randomised Clinical Trial impossible[50] . Further, a few of the patients were excluded from the analysis and, therefore, the results of the research cannot be extrapolated to all patients with urgent abdominal pathology. It is known, however, that the selection of the appropriate technique is not only expected, rather is necessary in emergency surgery, as not every patient with an acute abdomen could be managed by a minimally invasive surgical approach[11] . Next, the study population appeared to be quite heterogeneous with different indications for the exploration. Finally, as we pragmatically assessed the immediate effect of the exposure of interest, we are not aware of late complications. It is tempting to hypothesise that patients post ML exploration who experienced accelerated postoperative recovery may return to work faster and have less frequent late morbidity and higher aesthetic satisfaction than those operated by a standard laparotomy. Late outcomes need to be evaluated by further research with a longer follow-up period.
There are also some strengths of this study to be mentioned. To control the potential confounders, we performed the following. First, we excluded non-eligible participants before the allocation process applying clear and specific criteria for the enrolment in the study. As a result, study cohorts appeared to be well-matched for the main demographic and clinical variables (Table 1). Second, to achieve acceptable statistical power we obtained the required sample size. Third, we applied intention-to-treat analysis anticipating the methodological and practical benefits associated with this strategy[23] . Fourth, quantitative outcomes (OT, EBL) were calculated blindly by independent evaluators not involved directly in the study. Fifth, we have a low proportion of patients who dropped out during follow-up (8%), and this could strengthen inferences from the data evaluated. Last, as the counterargument to the aetiological heterogeneity of the population, this is a clinical study, and the participants are expected to represent a cross-section of the real-world admissions to acute surgical services. Therefore, acknowledging the weaknesses of our analysis, we assume that the findings obtained could be of certain relevance for clinicians working in smaller hospitals and we hope that our work will encourage further research in the field.
CONCLUSION
According to our data, ML is a safe, minimally invasive and attractive alternative to a traditional laparotomy approach in emergency general surgery, and, although demanding, it could be applied for the treatment of a larger number of conditions that are currently practised. Our results suggest that this technique could benefit the patients enhancing their postoperative recovery. Evident limitations of this work warrant large-scale studies to validate the findings obtained. The following questions that could be asked include: 1) Are there specific indications to use the ML in patients with acute abdomen? 2) What should be the role of ML in abdominal trauma? 3) Could the employment of ML access reduce the incidence of late postoperative complications compared with the conventional exploration method? After all, is there any place for ML incision in the modern laparoscopic and robotic era?
What is already known on this topic:
• Mini-invasive surgery has become a standard approach in many elective general procedures • Open laparotomy remains a predominant access in surgical emergency including abdominal trauma • Immediate results of laparoscopy-assisted procedures and ML are comparable
What this study adds:
• ML is a safe exploration which is associated with similar morbidity compared with a conventional laparotomy in an emergency setting • ML could bring additional benefits to patients reducing intra-operative stress and enhancing their recovery
DECLARATIONS
Acknowledgements The authors acknowledge members of the surgical team, information officers, and management of the hospital for their support during the study
Competing interests The authors declared that they have no competing interests
Funding No funding or grants were received for the study
Authors’ contributions Study concept, design and supervision: SK. Acquisition, analysis of data, and drafting of the manuscript: both authors. Both authors critically revised read and approved the final manuscript.
REFERENCES
- Meara JG, Leather AM, Hagander L, et al. Global Surgery 2030: Evidence and solutions for achieving health, welfare, and economic development. Lancet 2015; 386: 569-624.http://dx.doi.org/10.1016/S0140-6736(15)60160-X
- Rickard J, Pohl L, Abahuje E. Indications and Outcomes for Non-Trauma Emergency Laparotomy: A Comparison of Rwanda, South Africa, and the USA. World J Surg 2021 Mar 45(3): 668-77. https://doi.org/10.1007/s00268-020-05862-y
- Khuri SF, Henderson WG, De Palma RG, et al. Determinants of Long-Term Survival After Major Surgery and the Adverse Effect of Postoperative Complications. Ann Surg 2005;242(3): 32–48. DOI: 10.1097/01.sla.0000179621.33268.83.
- Scott MJ, Baldini G, Fearon KCH, et al. Enhanced Recovery After Surgery (ERAS) for gastrointestinal surgery, part 1: pathophysiological considerations. Acta Anaesth Scand 2015; 59: 1212–31. DOI: 10.1111/aas.12601.
- Chen CF, Lin YC, Tsai HL, et al. Short- and long-term outcomes of laparoscopic-assisted surgery, mini-laparotomy and conventional laparotomy in patients with Stage I-III colorectal cancer. J Minim Access Surg. 2018 Oct-Dec; 14(4): 321-34. DOI: 10.4103/jmas.JMAS_155_17
- Zhao JJ, Syn NL, Chong C, et al. Comparative outcomes of needlescopic, single-incision laparoscopic, standard laparoscopic, mini-laparotomy, and open cholecystectomy: A systematic review and network meta-analysis of 96 randomized controlled trials with 11,083 patients. Surgery 2021; 170(4): 994-1003; https://doi.org/10.1016/j.surg.2021.04.004
- Balasubramanian A, Cheddie S, Naidoo NM, et al. An evaluation of mini-laparotomy cholecystectomy in the laparoscopic era: a rural experience. S Afr J Surg 2018; 56(2): 36-40. http://dx.doi.org/10.171159/2078-5151/2018/v56n2a2287
- Zhou T, Zhang G, Tian H, et al. Laparoscopic rectal resection versus open rectal resection with minilaparotomy for invasive rectal cancer. J Gastrointest Oncol 2014; 5(1): 36-45; doi: 10.3978/j.issn.2078-6891.2013.052.
- Settembrini AM, Aronici M, Martelli E, et al. Is Mini-Invasive Surgery an Alternative for the Treatment of Juxtarenal Aortic Aneurysms? Ann Vasc Surg 2022 Jan; 78: 220-5; https://doi.org/10.1016/j.avsg.2021.06.014
- Corcione A, Angelini P, Bencini L, et al. Joint consensus on abdominal robotic surgery and anesthesia from a task force of the SIAARTI and SIC. Minerva Anestesiol 2018 Oct; 84(10): 1189-1208. DOI: 10.23736/S0375-9393.18.12241-3.
- De’Angelis N, Khan J, Marchegiani F, et al. Robotic surgery in emergency setting: 2021 WSES position paper. World J Emerg Surg 2022; 17: 4; https://doi.org/10.1186/s13017-022-00410-6
- Donohue SJ, Reinke CE, Evans SL, et al. Laparoscopy is associated with decreased all-cause mortality in patients undergoing emergency general surgery procedures in a regional health system. Surg Endosc 2022; 36: 3822–32. https://doi.org/10.1007/s00464-021-08699-1
- Chen CF, Lin YC, Tsai HL, et al. Short- and long-term outcomes of laparoscopic-assisted surgery, mini-laparotomy and conventional laparotomy in patients with Stage I-III colorectal cancer. J Minim Access Surg 2018 Oct-Dec; 14(4): 321-34. DOI: 10.4103/jmas.JMAS_155_17.
- Zhang G and Wu B. Meta‑analysis of the clinical efficacy of laparoscopic appendectomy in the treatment of acute appendicitis. World J Emerg Surg 2022;17: 26. https://doi.org/10.1186/s13017-022-00431-1
- Ceresoli M, Pisano M, Abu‑Zidan F, et al. Minimally invasive surgery in emergency surgery: a WSES survey. World J Emerg Surg 2022; 17(1): 18; https://doi.org/10.1186/s13017-022-00419-x
- Frassini S, Cobianchi L, Fugazzola P, et al. ECLAPTE: Effective Closure of LAParoTomy in Emergency—2023 World Society of Emergency Surgery guidelines for the closure of laparotomy in emergency settings. World J Emerg Surg 2023; 18: 42. https://doi.org/10.1186/s13017-023-00511-w
- Gao Y, Li S, Xi H, et al. Laparoscopy versus conventional laparotomy in the management of abdominal trauma: a multi‑institutional matched‑pair study. Surg Endosc 2020; 34: 2237-42. https://doi.org/10.1007/s00464-019-07013-4
- Romeo L, Bagolini F, Ferro S, et al. Laparoscopic surgery for splenic injuries in the era of non‑operative management: current status and future perspectives. Surgery Today 2021; 51: 1075-84; https://doi.org/10.1007/s00595-020-02177-2
- Sermonesi G, Tian BWCA, Vallicelli C, et al. Cesena guidelines: WSES consensus statement on laparoscopic‑first approach to general surgery emergencies and abdominal trauma. World J Emerg Surg 2023;18: 57. https://doi.org/10.1186/s13017-023-00520-9
- Kong F-B, Deng Q-M, Deng H-Q, et al. Propensity score–matched comparison between totally laparoscopic right hemicolectomy with transcolonic natural orifice specimen extraction and conventional laparoscopic surgery with mini-laparotomy in the treatment of ascending colon cancer (with video). Gastrointest Endosc 2021 Sept; 94(3): 642-50. https://doi.org/10.1016/j.gie.2021.03.028
- Axelrod, DA, Hayward, R. Nonrandomized Interventional Study Designs (Quasi-Experimental Designs). In: Penson DF, Wei JT (eds) Clinical Research Methods for Surgeons. 2006. Humana Press. https://doi.org/10.1007/978-1-59745-230-4_4
- Charan J, Biswas T. How to Calculate Sample Size for Different Study Designs in Medical Research? Indian J Psychol Med 2013; 35(2): 121-6. DOI: 10.4103/0253-7176.116232.
- Quah GS, Eslick GD, Cox MR. Laparoscopic versus open surgery for adhesional small bowel obstruction: a systematic review and meta-analysis of case–control studies. Surg Endosc 2019; 33: 3209–32. https://doi.org/10.1007/s00464-018-6604-3
- Tripepi G, Chesnaye NC, Dekker FW, et al. Intention to treat and per protocol analysis in clinical trials. Nephrology 2020; 25: 513-7. https://doi.org/10.1111/nep.13709
- Scott MJ, Baldini G, Fearon KCH, et al. Enhanced Recovery After Surgery (ERAS) for gastrointestinal surgery, part 1: pathophysiological considerations. Acta Anaesth Scand 2015; 59: 1212-31. DOI:10.1111/aas.12601.
- Feldheiser A, Aziz O, Baldini G, et al. Enhanced Recovery After Surgery (ERAS) for gastrointestinal surgery, Part 2: consensus statement for anaesthesia practice. Acta Anaesth Scand 2016; 60: 289-334. DOI: 10.1111/aas.12651.
- Peden CJ, Aggarwal G, Aitken RJ. Guidelines for Perioperative Care for Emergency Laparotomy Enhanced Recovery After Surgery (ERAS) SocietyRecommendations: Part 1—Preoperative: Diagnosis, Rapid Assessment and Optimization. World J Surg 2021; 45: 1272-90. https://doi.org/10.1007/s00268-021-05994-9
- Surgical Site Infection Event: Center for Disease Control. 2010; http://www.cdc.gov/nhsu/PDFs/pscManual/9pscSSIcurrent.pdf?agree=yes&next=Accept. Updated Jan 2015. Accessed October 06, 2022.
- Horvath B, Kloesel B, Todd MM, et al. The Evolution, Current Value, and Future of the American Society of Anesthesiologists Physical Status Classification System. Anesth 2021; 135: 904-19. DOI:10.1097/ALN.0000000000003947.
- Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis—2012: revision of the Atlanta classification and definitions by international consensus. Gut 2013; 62: 102–11. https://doi.org/10.1136/gutjnl-2012-302779
- Kozar RA, Crandall M, Shanmuganathan K, and the AAST Patient Assessment Committee. Organ injury scaling 2018 update: Spleen, liver, and kidney. J Trauma Acute Care Surg 2018; 85(6): 1119-22. DOI: 10.1097/TA.0000000000002058.
- Baker SP, O'Neill B, Haddon W Jr, et al. The injury severity score: a method for describing patients with multiple injuries and evaluating emergency care. J Trauma 1974; 14(3): 187-96.
- Dindo D, Demartines N and Clavien P-A. Classification of Surgical Complications. A New Proposal With Evaluation in a Cohort of 6336 Patients and Results of a Survey. Ann Surg 2004; 240: 205-13. DOI: 10.1097/01.sla.0000133083.54934.ae.
- Watters DA, Wilson L. The Comparability and Utility of Perioperative Mortality Rates in Global Health. Curr Anaesth Rep 2021; 11: 48-58; https://doi.org/10.1007/s40140-020-00432-3
- Chestovich PJ, Browder TD, Morrissey SL, et al. Minimally invasive is maximally effective: Diagnostic and therapeutic laparoscopy for penetrating abdominal injuries. J Trauma Acute Care Surg 2015; 78(6): 1076-85. DOI: 10.1097/TA.0000000000000655.
- Seow-En I, Seow-Choen F. Sigmoid volvulus treated by mini-incision. Tech Coloproctol 2014; 18: 1169-71. DOI: 10.1007/s10151-014-1230-0.
- Fleshman JW, Fry RD, Birnbaum EH, et al. Laparoscopic-assisted and minilaparotomy approaches to colorectal diseases are similar in early outcome. Dis Colon Rectum 1996; 39: 15-22; https://doi.org/10.1007/BF02048262
- Wang X-D, Huang M-J, Yang C-H. Minilaparotomy to rectal cancer has higher overall survival rate and earlier short-term recovery. World J Gastroenterol 2012 Oct; 18(37): 5289-5294; http://dx.doi.org/10.3748/wjg.v18.i37.5289
- Van der Naald N, PrinsMI, Otten K, et al. Novel Approach to Treat Uncomplicated Sigmoid Volvulus Combining Minimally Invasive Surgery with Enhanced Recovery, in a Rural Hospital in Zambia. World J Surg 2018; 42: 1590-6; https://doi.org/10.1007/s00268-017-4405-9
- Enrique EL, Hamdy KA. Minilaparotomy without general anesthesia for the treatment of sigmoid volvulus in high-risk patients: A case series of 4 patients. Inter J Surg Case Reports 2017; 34: 23-6. DOI: 10.1016/j.ijscr.2017.02.055.
- Tavassoli A, Maddah G, Noorshafiee S, et al. A Novel Approach to Minimally Invasive Management of Sigmoid Volvulus. Acta Med Iran 2016; 54(10): 640-3.
- Cirocchi R, Birindelli A, Inaba K, et al. Laparoscopy for Trauma and the Changes in its Use From 1990 to 2016: A Current Systematic Review and Meta-Analysis. Surg Laparosc Endosc Percutan Tech 2018 Feb; 28(1): 1-12. https://doi.org/10.1097/SLE.0000000000000466
- Huang GS, Chance EA, Hileman BM, et al. Laparoscopic Splenectomy in Hemodynamically Stable Blunt Trauma. J Soc Laparoendosc Surg 2017 April-June; 21(2): e2017.00013. DOI: 10.4293/JSLS.2017.00013.
- Smyth L, Bendinelli C, Lee N, et al. WSES guidelines on blunt and penetrating bowel injury: diagnosis, investigations, and treatment. World J Emerg Surg 2022; 17: 13. https://doi.org/10.1186/s13017-022-00418-y
- Bain K, Meytes V, Chang GC, et al. Laparoscopy in penetrating abdominal trauma is a safe and effective alternative to laparotomy. Surg Endosc 2019; 33: 1618-25. https://doi.org/10.1007/s00464-018-6436-1
- Frassini S, Cobianchi L, Fugazzola P, et al. ECLAPTE: Effective Closure of LAParoTomy in Emergency—2023 World Society of Emergency Surgery guidelines for the closure of laparotomy in emergency settings. World J Emerg Surg 2023; 18: 42. https://doi.org/10.1186/s13017-023-00511-w
- Davidson I and Hillier V. Comparison of four methods of allocation for clinical trials with small sample sizes. Physiotherapy 2002; 88(12): 722-9.
- Ott RL, Longnecker M. An Introduction to Statistical Methods and Data Analysis. 7th Edition. Boston, Cengage Learning, 2015, p.28-9.
- Fusco D, Saitto C, Arcà M, et al. Cyclic fluctuations in hospital bed occupancy in Roma (Italy): supply or demand driven? Health Serv Manage Res 2003; 16: 268-75.
- McCulloch P, Taylor I, Sasako M, et al. Randomized trials in surgery: problems and possible solutions. BMJ 2002; 324: 1448–51. https://doi.org/10.1136/bmj.324.7351.1448
Medical Journal of Zambia, Vol 51, 1
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.