CASE REPORT Breast cancer surgery under General Anaesthesia in a Nonagenarian male with a pacemaker: a case report from Nigeria
Dimoko AA
Department of Surgery, Bayelsa Medical University, Yenagoa – Bayelsa, Nigeria
Fyneface-Ogan S
Department of Anaesthesia, College of Health Sciences, University of Port Harcourt, Port Harcourt, Nigeria
DOI: https://doi.org/10.55320/mjz.51.1.446
Keywords:Male breast cancer, nonagenarian, pacemaker, general anaesthesia
ABSTRACT
Worldwide, breast cancer is the most common cancer. Male breast cancer (MBC) in men is still an uncommon and largely understudied and poorly reported disease. This disease makes up <1% of breast cancers in humans. In both males and females, breast cancer has been associated with high mortality rates. More than 80% of patients diagnosed with breast cancer will undergo surgery as part of their treatment and in most cases; surgery is performed under general anaesthesia. However, the coexistence of significant cardiac comorbidities further complicates the diagnostic and therapeutic approach of breast cancer in the elderly.
This case report describes the presentation, diagnostic journey, and the anaesthetic and surgical management of breast cancer in a 92-year-old male with a significant cardiac morbidity that impacts with the quality of life of the patient. The report also highlights the challenges associated with the intraoperative anaesthetic and postoperative pain management of the patient. It emphasizes the importance of multispecialty collaboration and the development of adjuvant treatments which are tailor made for the patient.
INTRODUCTION
Male breast cancer (MBC) is a rare condition making up < 1% of all malignancies in men and 1% of breast cancers globally? In Sub–Saharan Africa figures range from as low as 1.3% in Zimbabwe to as high as 12.5% in Kenya. In Nigeria, MBC accounts for between 2.2% and 8.0% of breast cancer cases (1). Median age at diagnosis is 65 years which is 8-10 years more than in women. Risk factors are multiple and include family history, obesity, alcohol intake, testicular damage, liver damage, radiotherapy to the chest and high ambient temperature. The final common pathway is testosterone-oestrogen imbalance. The relatively high incidence in some African countries is thought to be due to hyper-oestrogenaemia caused by hepatic schistosomiasis. [1,2]
A painless retroareolar lump is the commonest symptom. Nipple involvement and discharge may also occur. [3] Late presentations are common features in our environment because most patients are unaware of the existence of male breast cancer.[2] At least 90% of MBCs are invasive ductal carcinoma while < 2% is lobular. Over 90% are Oestrogen Receptor (ER) positive, Progesterone Receptor (PR) positive and Human Epidermal Growth Factor Receptor (HER) negative.[3]
Cardiology and oncology are often considered separate fields, but they often intersect because antecedent cardiovascular health can affect selection of treatment which may also result in cardiac toxicities that affect prognosis. The developing subspecialty of cardio-oncology aims to provide optimal cancer care without compromising cardiovascular health. [4]
CASE REPORT
A 92-year-old patient was seen in the surgical outpatient clinic with an 8 year history of a left sided breast mass and a 6-month history of bloody nipple discharge. He had excision biopsy at a private hospital 6 years previously with recurrence 6 months after the procedure. There was no record of the previous histology report. There was no family history of breast disease.
Physical examination revealed an elderly male weighing 53 kg (height and BMI?) who was slightly lethargic but was not pale, febrile or icteric. Pulse rate was 40/min and blood pressure was 130/90mmHg and apex beat was in the 5th left intercostal space mid-clavicular line. The first and second heart sounds were audible and there were no additional sounds. His chest was clinically clear. There was a 10cm by 14cm mass occupying the left breast. The mass was firm, non-tender, and adherent to overlying skin and free of the underlying pectoralis major muscle. The right chest wall and axilla were essentially normal.

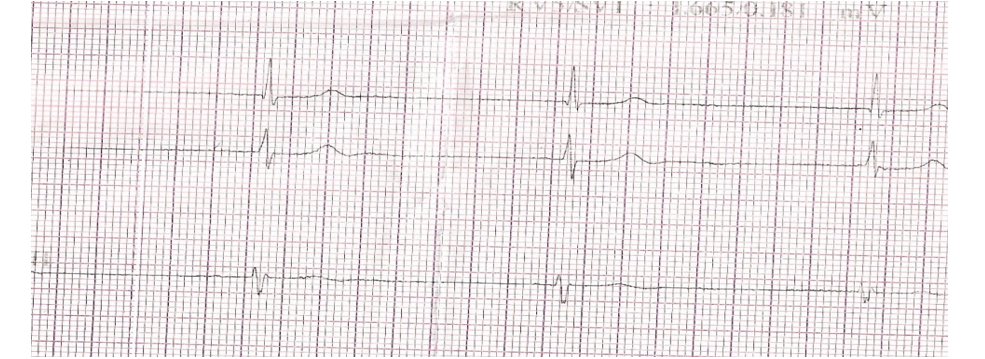
Frank's bloody discharge was observed from the left nipple and a solitary central axillary lymph node was palpable (use level I,II or lll). A core biopsy of the breast mass confirmed a diagnosis of infiltrating ductal carcinoma which was ER and PR positive. Chest radiograph and abdominal ultrasound did not show any evidence of distant spread. Stage the TNM and clinical stage of the cancer? Electrocardiogram confirmed second degree heart block and echocardiogram showed left ventricular hypertrophy.
He was referred to the cardiologist for evaluation and a transvenous pacemaker was inserted, placing the generator on the right side of the chest to leave the left side free for surgical intervention. Pulse rate normalized to 80/min after pacemaker insertion. In view of his advanced age and comorbidities a detailed discussion was held with the patient and his family on the risks and benefits of treatment. He was further reviewed by the cardiologist and Anaesthesiologist before being cleared for surgery under general anaesthesia.

The night before day of surgery he was further reviewed by the Anaesthesiologist and placed on a stat dose of oral diazepam 2.5mg. On the morning of surgery another oral dose of diazepam 2.5mg and intravenous ranitidine 50mg were administered.
In theatre, the patient was adequately preoxygenated and anaesthetic induction was with propofol 1.5mg/kg (80mg). Tracheal intubation was facilitated using suxamethonium 1.0mg/kg (50mg) and airway secured using a size 6.5mm (internal diameter) tracheal tube, Muscle relaxation was maintained with intravenous atracurium 0.4mg/kg body weight (20mg). Isoflurane 1.5% in 100% oxygen was administered to maintain unconsciousness while intraoperative analgesics administered were intravenous paracetamol 900mg and pentazocine 30mg. A modified radical mastectomy with level 1 axillary dissection was carried out. Intra-op vitals vital signs were essentially within normal reference ranges.
At the end of surgery, the conduct of anaesthesia was reversed and an admixture of atropine 1.2mg and neostigmine 2.5mg were administered. At full cognition, patient was transferred to the ward. Postoperative analgesia was with diclofenac100mg suppository 12 hourly, intravenous paracetamol 900mg eight hourly and intramuscular pentazocine 20mg every six hours in the first 48hrs. Subsequently, he received oral paracetamol 1000mg every six hours till the 4th postoperative day.
Recovery was uneventful and he was discharged on the 5th post-operative day. A review 14 days after discharge showed satisfactory wound healing. In view of his advanced age and cardiac co-morbidity it was felt that he would tolerate adjuvant chemo- and radiotherapy poorly. He was thus commenced on adjuvant hormonal therapy with Tamoxifen 20mg daily. Close cardiac monitoring with pacemaker interrogation was done on regular outpatient basis. A further review 6 months after surgery showed no significant adverse reactions to hormonal therapy. He is free of cardiac symptoms and the pulse rate remains within normal limits.
DISCUSSION
While MBC treatment options include surgery with or without radiation therapy, chemotherapy, hormonal therapy, and/or targeted therapy, comorbidity such as a cardiac disease poses an additional challenge. Treatment of MBC is guided by principles like those for female breast cancer (FBC). The relative rarity of MBC however makes studies to determine optimal treatment protocols difficult.
Modified mastectomy was the only option available to our patient as radiotherapy and other aggressive forms of management would have been inimical in the face of his cardiac disease. It is well known that the elderly with breast cancer who also have one or more risk factors for heart disease may indeed develop cardiovascular complications after breast cancer treatment.[5] It has been shown that combination chemotherapy utilizing anthracyclines like doxorubicin and other drugs such as 5 fluorouracil and paclitaxel are effective in neoadjuvant and adjuvant treatment. There is however a significant risk of irreversible heart damage especially in the elderly. Alternative drug regimens and therapies offer a less cardiotoxic profile and confer significant protection against breast cancer spread and recurrence. This is what informed our decision to use Tamoxifen in this patient instead of chemotherapy.[8]
Possible treatment modalities for MBC include surgery. Modified radical mastectomy with axillary dissection or sentinel node biopsy is the procedure of choice. Breast conserving surgery is also done but mostly in small, early tumours.[2] More than 90% of MBC are hormone receptor positive. Tamoxifen is the recommended adjuvant hormonal therapy unless where contraindicated.[3] Where an adverse side effect profile precludes tamoxifen use, aromatase inhibitors (AI) like anastrozole are used.[3] AI however do not provide maximal oestrogen blockade and need to be combined with a gonadotrophin releasing hormone (GnRH) analogue. The same effect may be achieved with bilateral orchidectomy.[2,8]
Adjuvant cyclical combination chemotherapy may be of benefit in aggressive or metastatic MBC. Specific drug combinations and treatment duration will depend on the individual case.[3]
Modified radical mastectomy was the only option available to our patient as radiotherapy and other aggressive forms of management would have been inimical in the face of his cardiac disease. It is well known that the elderly patients with breast cancer and one or more risk factors for heart disease may indeed manifest cardiac morbidity after breast cancer treatment.[5] It has been shown that combination chemotherapy with anthracyclines like doxorubicin and other drugs like 5 fluorouracil and paclitaxel is very effective in treatment of MBC. There is however a significant risk of irreversible heart damage especially in elderly patients. To avoid exacerbating an existing cardiac condition it was decided to withhold chemotherapy in our patient and instead commence hormonal treatment with tamoxifen which has a less deleterious effect on his heart while offering protection against spread and recurrence.[6]
One of the challenges in the anaesthetic management of our patient occurred during laryngoscopy and tracheal intubation. Securing the airway was fraught with loss of flexibility of the neck in our patient. However, this was anticipated as this was related to the age of the patient. There was severe joint ankyloses in the neck joints. Stiff joints, particularly in the cervical spine, hips, and shoulders, can prevent optimal patient positioning.
The doses of agents used for anaesthesia were also reduced. It is well known that with increasing age, changes in the brain result in a relative increase in the potency of propofol. As measured by electroencephalography suppression, geriatric patients are 30% more sensitive to the effects of propofol, when compared to younger patients, hence the reduced dose of propofol used in our patient. The choice of atracurium in our patient was premised on the fact that the degree of functionality of both the liver and kidneys have reduced significantly. Atracurium will depend on the Hoffmann’s degradation for its metabolism, hence its use in our patient.
Isoflurane was used in 100% oxygen. It has been shown that at the parenchymal level, age-related lung changes mimic those of emphysema in the elderly[7] . Alveolar airspace and physiologic dead space increase while surface area decreases, inhibiting gas exchange and causing a ventilation-perfusion mismatch. The functional residual capacity decreases while the closing capacity increases resulting in earlier closure of small airways, diffuse atelectasis, and shunting. These appear in pulmonary function testing as decreased forced expiratory volume (FEV1), decreased diffusion capacity of the lung (DLCO), and increased alveolo-capillary gradient.[7]
CONCLUSION
It is important for elderly individuals with male breast cancer to have a multidisciplinary team of healthcare professionals, including surgeons, anaesthetists, cardiologists, oncologists, and other specialists to improve treatment outcomes. Given the limited data specific to male breast cancer, more research and clinical trials are needed to refine treatment strategies and improve outcomes. In the context of this case, it is also important to educate patients on the existence of male breast cancer.
DECLARATIONS
Informed consent
Verbal informed consent was obtained from the patient and his family.
Conflict of interest
None.
REFERENCES
- Kidmas AT, Ugwu BT, Manasseh AN, Iya D, Opelika AS. Male breast malignancy in Jos University teaching hospital. West African Journal of Medicine 2005; 24(1):36-40.
- Zheng G, Leone JP. Male Breast Cancer: An Updated Review of Epidemiology, Clinicopathology, and Treatment. J Oncol. 2022 May 24; 2022:1734049. doi: 10.1155/2022/1734049
- Leon-Ferre RA, Giridhar KV, Hieken TJ, Mutter RW, Couch FJ et al. A contemporary review of male breast cancer: Current evidence and unanswered questions. Cancer and Metastasis Reviews 2018;37 :599-614.
- Mehta LS, Watson KE, Barac A, Beckie TM, Bittner V et al. Cardiovascular disease and breast cancer: Where these entities intersect: A scientific statement from the American Heart Association. Circulation. 2018; 137(8):e30-66.
- Barish R, Lynce F, Unger K, Barac A. Management of Cardiovascular Disease in Women with Breast Cancer. Circulation 2019; 139(8):1110-1120
- Reis SE, Costantino JP, Wickerham DL, Tan-Chiu E, Wang J, Kavanah M. Cardiovascular Effects of Tamoxifen in Women with and without Heart Disease: Breast Cancer Prevention Trial. J National Cancer Inst. 2001; 93: 16-21
- Hedenstierna G, Tokics L, Scaramuzzo G, Rothen HU, Edmark L et al. Oxygenation Impairment during Anesthesia: Influence of Age and Body Weight. Anesthesiology 2019; 131(1): 46-57
- Cutuli B, Le-Nir CC, Serin D, Kirova Y, Gaci Z et al. Male breast cancer. Evolution of treatment and prognostic factors. Analysis of 489 cases. Critical reviews in Oncology and Hematology 2010; 73(3): 246-254.
Medical Journal of Zambia, Vol 51, 1
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.