Experiences of women diagnosed with HIV during pregnancy at selected health facilities in Lusaka District, Zambia: A Descriptive Cross-Sectional Study
Brenda Nambala Sianchapa
University of Zambia, School of Nursing Sciences, Department of Midwifery, Women’s and Child Health, Lusaka, Zambia.
Patricia Katowa-Mukwato
University of Zambia, School of Nursing Sciences, Department of Basic and Clinical Nursing Sciences, Lusaka, Zambia.
Catherine M. Ngoma
University of Zambia, School of Nursing Sciences, Department of Midwifery, Women’s and Child Health, Lusaka, Zambia.
DOI: https://doi.org/10.55320/mjz.51.1.443
Keywords:Experience, women, HIV positive diagnosis, pregnancy, ART adherence, Intimate Partner Violence
ABSTRACT
Background: In an effort to prevent vertical transmission of HIV, pregnant women undergo HIV testing and where appropriate, are enrolled into HIV care. Receiving an HIV positive diagnosis can lead to stress and other experiences.
Aim: To explore the experiences of women diagnosed HIV positive during pregnancy at selected Health facilities in Lusaka district.
Methodology: This was part of a longitudinal mixed methods panel study which was done in 3 stages, and this was stage 3 of the study which utilised a descriptive cross-sectional study design. In-depth interviews were conducted on 17 purposively selected postpartum women who were diagnosed HIV positive during their recent pregnancy. Data were analysed using thematic analysis. The 6-phase coding framework for thematic analysis was used to identify themes and patterns in the data.
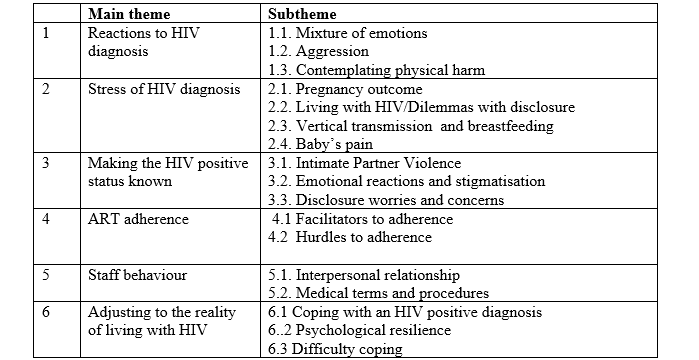
Major findings: Six main themes emerged: reactions to HIV diagnosis, stress of HIV diagnosis, making the HIV status known, ART adherence, staff behaviour and adjusting to the reality of living with HIV. Most participants reported a mixture of emotions upon receiving the diagnosis, including anger, disappointment, disbelief, shock, turmoil, with others becoming aggressive and contemplating physical harm to themselves and the foetus. Most participants reported being stressed about the diagnosis due to fear of vertical transmission and uncertainty about pregnancy outcome and future. Others reported Intimate Partner Violence upon disclosing to their sexual partners while some reported inconsistent ART adherence. Participants described some staff as being supportive, while others were described as being rude.
Conclusion: The study recommends empathetic support by Health care providers, to women diagnosed with HIV during pregnancy, together with their significant others as they undergo the reality of living with HIV.
INTRODUCTION
A diagnosis of Human Immune-deficiency Virus (HIV) usually causes stress in the affected individual because of its lack of cure[1] . Worse off, an HIV positive diagnosis during pregnancy may be stressing to the woman as it comes unexpectedly during a routine antenatal care visit, and has a number of effects. While many people have been diagnosed and lived with chronic medical conditions, HIV diagnosis can lead to social problems because it is usually associated with stigmatisation of the victims by society, and sometimes, self-stigmatisation[2] .
Individuals who would like to know their HIV status usually undergo Voluntary Counselling and Testing (VCT), and may postpone the VCT to a time when they are ready. However, in an effort to eliminate mother-to-child transmission (eMTCT) of HIV, pregnant women have to undergo HIV testing during antenatal care, and are commenced on HIV management as appropriate. Pregnancy is a sensitive and stressful state as the body of the pregnant woman adjusts in order to maintain the pregnancy and prepare for labour and delivery; and the puerperium[3,4] . An HIV positive diagnosis can contribute to stress and other negative effects, including, poor antiretroviral treatment adherence, poor attendance at health care and faster disease progression[5-8] .
With a diagnosis of HIV infection during pregnancy, the woman constantly fears about infecting her baby, and has the dilemma of disclosing her diagnosis to the spouse or family members. Disclosure is cardinal for her social support, adhering to antiretroviral medication (ARVs), and making a radical choice about infant feeding in an effort to eliminate Mother to Child Transmission of the infection. However, disclosure sometimes leads to Intimate Partner Violence (IPV). The Zambia Demographic and Health Survey reported that 85% of ever married women disclosed their diagnosis to their partner, and 10 % of ever married women aged 15 to 49 years have experienced physical violence from the husband during pregnancy in 63% of cases[9,10] . Some of this IPV could be resulting from disclosing an HIV positive diagnosis made during antenatal screening.
The effects of an HIV positive diagnosis during pregnancy can be made bearable when the affected woman is assisted to cope with her condition. All antenatal clinics, including those in Lusaka district are equipped to offer post-test counselling and enrol the clients into HIV care. When a mother diagnosed with HIV infection during pregnancy utilises effective coping strategies, the level of internalised stigma and depression begin to decrease, and self-esteem increases[8] .Those who employ negative ways of coping may resort to harmful behaviours, like substance abuse, continuing to have unsafe sexual intercourse, or simply denying that they have the virus [11,12] .
Governments around the world have been working to find solutions to the problem of HIV and many studies have been conducted which have led to discoveries and successes in handling HIV infected individuals. However, despite medical advances in the management of HIV, there are still emotional and social problems that can be as hard to deal with as the illness itself. For many people, it is a stigmatising condition which makes the burden of illness more difficult to bear. In order to provide appropriate services to women diagnosed with HIV during pregnancy, it is important to know their experiences.
This study therefore aimed to explore the experiences of women who were diagnosed HIV positive during pregnancy at selected Health facilities in Lusaka District. The findings will help in providing guidelines to care for the clients and their families to help them cope with the stress of an HIV positive diagnosis.
METHODS
Research design
This study utilised a qualitative descriptive cross sectional design. It was part of a longitudinal mixed methods panel study, which was conducted in 3 stages. Stages 1 and 2 collected quantitative data while stage 3 collected qualitative data.
Study setting
The study was conducted at Chilenje Level 1 Hospital, Kanyama Level 2 Hospital and George Health centre in Lusaka District, the capital of Zambia. The Health facilities offer maternal and child health services, HIV counselling and testing and ART services among others. The study settings were chosen to provide diversity in demographic characteristics of participants, which might have an influence on how they experience the diagnosis of HIV infection made during pregnancy.
Participants
The study population were women seeking 6th week postnatal care services at the study settings who tested HIV positive for the first time during their recent pregnancy.
Sampling technique
The health facilities were purposively selected. Purposive sampling was used to select 17 postnatal women who had been diagnosed with HIV during their recent pregnancy, based on the recommendation by Thomson et al, 2011 of a sample size of 12 to 20 participants in order to adequately analyse each participant’s data[15] .
Inclusion criteria
Diagnosed HIV positive for the first time during recent pregnancy and resident at the study settings
Exclusion criteria
Suffering from chronic medical conditions or pregnancy danger signs and complications at recruitment.
Procedures
Data collection tool
A self-constructed structured interview schedule translated into a local language called Chinyanja, was used to conduct the in-depth interviews and solicited information on participants’ experiences of the stress of an HIV positive diagnosis, IPV, ART adherence, physiological health and coping with the stress.
Data collection technique
Data were collected from September, 2022 to January, 2023 during the participants’6th week postnatal visit. The data collection instruments were administered after all the examinations for the visit had been conducted. The participants were identified by the Midwife conducting the postnatal examinations, and escorted to the interview room by the same midwife. The researcher, who had created rapport with the participants since their recruitment into the study, began by reminding the participants about the purpose of the study, which had been fully explained to them at recruitment. Participants did not have to sign a consent form during stage 3 as these were panel studies and they had signed the consent forms at enrolment. Chinyanja and English were used during data collection as they are the languages commonly spoken at the study settings.
Face to face in-depth interviews were conducted, each lasting 50 to 80 minutes, in which women were asked to narrate their experiences after receiving an HIV positive diagnosis. Open ended questions were asked to address each section of the interview schedule, and participants were encouraged to narrate their experiences with the necessary probes and prompts. A maximum of two (2) interviews were conducted per day whenever participants visited the Health facility for their 6th week postnatal visit.
The interviews were tape recorded, and transcribed verbatim after data collection. At the end of each interview, key points were summarised to the participant in order to verify the data. Thereafter they were thanked for their participation and given a snack owing to the longer period that they had spent at the health institution as they took part in the study. Participants at George Health centre were not given any snacks because the Sister in charge advised that they were suspicious of researchers who gave them food.
The interviews were conducted by a midwife who has a Master of Science Degree, and experience in qualitative data collection. Credibility was also enhanced by having the data scrutinised by two research supervisors who are Associate Professors and have experience in qualitative research.
Data analysis
Thematic analysis was used to analyse data. The 6-phase coding framework for thematic analysis[17] was used to identify themes and patterns in the data. Alphanumeric symbols were used to describe the study participants and their participant numbers were maintained as assigned at stage 1 of the study.
Ethical concerns
Ethical clearance was granted by University of Zambia Biomedical Research Ethics Committee (UNZABREC) on 5th January, 2022, REF. NO. 2150-2021; written permission was granted by the National Health Research Authority on 28th January, 2022, REF. NO. NHRA 000020/28/01/2022, and thereafter, by Lusaka District Medical Office and the study settings. The data is anonymous and there are no identification numbers to link the participants to it. This being part of a longitudinal panel study, participants’ names and phone numbers were written on a separate diary, for easy follow-up, but never on the data collection tool. There was no direct benefit for the participants, but the knowledge generated from this study is intended to improve the care for women diagnosed with HIV during pregnancy. There were no procedures in the study that caused direct harm to the participants as no experiments were done on them. Counselling services were available for those who broke down during the interviews. Participants were also accorded their full HIV package, thus, ART, counselling and scheduled reviews. Confidentiality was maintained by restricting access to documents containing participants’ information by using private rooms and passwords.
RESULTS
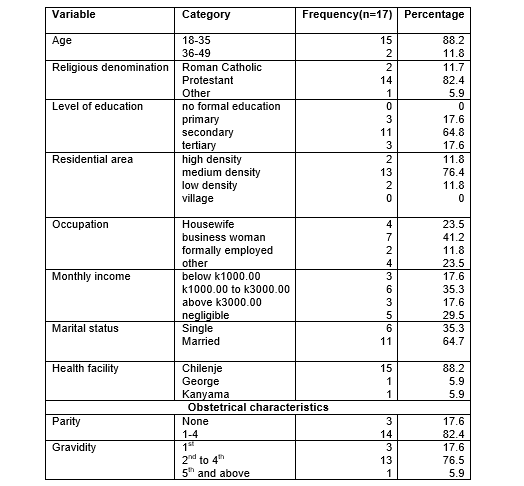
The demographic characteristics for the participants are found in Table 1 and majority (15: 88.2%) of them were in the age group 18 to 35 years, which is the safest for child bearing, with majority (11:64.7%) being married, and most (14: 82.4%) of them having 1 to 4 children. Marriage is the right place for childbearing in many cultures, which provides a stable home for children to grow and thrive in.
After data analysis six main themes emerged, with seventeen sub-themes (Table 2). The questions from which the themes emerged focused on participants’ experiences with being diagnosed HIV positive during a routine antenatal care visit, disclosure of an HIV positive diagnosis, induced stress, ART adherence, and coping with the stress of an HIV positive diagnosis. Participants gave several responses, upon which the sub-themes emerged.
1. Theme 1: Reactions to HIV diagnosis
Receiving an HIV positive diagnosis brings about a number of reactions because of its lack of a cure. Therefore, women who were diagnosed HIV positive during pregnancy had emotional and physical reactions to the news. Participants were asked how they felt when they were informed of their HIV positive diagnosis and most of them reported undergoing a number of emotional reactions which included the following;
1.1 Mixture of emotions
Most of the participants explained that they experienced a mixture of emotions like shock, turmoil, anger and disappointment, with some of them simply refusing to believe that this could be true. Others described the pain they felt, and how they cried, with ensuing depression. Some of them found solace in prayer while others sought counselling in order to deal with their mixture of emotions, like P 13 who explained it this way, ‘’ I kept quiet, was in shock. I was disturbed but after I was counselled, I accepted the condition. It happens because sometimes as a wife, you can be faithful but your husband may be going out with others so just accept and pray.” Other participants found it hard to accept the situation as summed up in the statement below;
This indeed shows the mixed emotions that women go through after receiving an HIV positive diagnosis during pregnancy. Participants also described being devastated, and regretting the pregnancy, like P 104 who said, “I was devastated because I used to test and I was negative before this”, and this was reiterated by P 17 who recalled the moment and, while crying, said, “I felt very bad and felt like committing suicide. I regretted the pregnancy, because before this, I was just okay.” In these instances, participants blamed their pregnancy for their diagnosis and attributed their HIV positive status to the pregnancy.
Some participants described receiving the diagnosis as a blow as expressed in the statement below;
Other participants reported being filled with fear at the prospect of dying, like P 21 who summed it as, “I felt and feared that I would die.” Fear of death could lead to more stress in the women, which could adversely affect their health and that of their unborn baby.
1.2 Aggression
Participants described being devastated which made them aggressive as follows; “I was devastated. I went and broke everything breakable at my boyfriend’s place” (P26). Having aggressive feelings and actions could add to the stress that one is experiencing, as they continue having negative feelings and unforgiveness to the offender.
1.3. Contemplating physical harm
Other participants contemplated physical harm to themselves and their unborn babies as stated by some of them; “I wanted to commit suicide. I wanted to abort the baby because it would still die anyway” (P 17). This was emphasised by P 49 who also had depression and foeticidal ideas and this was her description, “during the time when I experienced depression, I felt that maybe I needed to abort, until after counselling. I felt the need to abort many times”. Asked why she wanted to abort, she responded, “I thought my baby will blame me when he grows up.” This shows that women may still be lacking understanding on HIV and its management, especially the role of ARVs in elimination of Mother to Child Transmission of HIV, which gives a chance to the babies to survive and grow up as HIV negative individuals.
Theme 2: Stress of HIV diagnosis
An HIV positive diagnosis is usually stress-inducing because people know that it is an incurable disease, with stigmatisation attached to it. When made during pregnancy, the diagnosis of HIV instils fear in most women as they keep worrying about the outcome of their pregnancy and health of their baby. Participants were asked if they got stressed by the HIV diagnosis and what stressed them most about it, and those who affirmed gave their reasons as described in the sub-themes below;
2.1 Pregnancy outcome
Participants reported being stressed due to uncertainty about the outcome of their pregnancy in light of their HIV positive status as explained by P 5 in the following statement;
2.2 Living with HIV and Dilemmas with disclosure
Most of the participants were stressed about living with the incurable virus while facing possible rejection and stigmatisation by their loved ones, which also caused dilemmas with disclosure of the diagnosis. Disclosure is necessary for the patients’ social support, prevention of infection to the spouse in the event that he is HIV negative, and ART adherence. A number of the participants cited fear of stigmatisation as the most stressor, as resounded by some of them, “I have to take the drugs secretly and I also fear that people will stigmatise me once they know” (P 18), and P 44 who said, “I feared further rejection from my husband.” P 45 also explained her fears in the following statement;
While others were stressed because of fear of stigmatisation by other people, participants also self-stigmatised, like P 5 who said, “When I aborted, I left my job because I was HIV positive’’ (P 5). Self-stigmatisation is not good because the patient gets stressed up thinking that people know about her condition and will talk about her when in fact, no one is even talking about her. Fear of stigmatisation can also lead to a lot of secrecy which can lead to compromised ART adherence as the patient would have to take the medicine secretly. Participants also reported breastfeeding their baby because if they did not, society would conclude that they were HIV positive (P 21).
Participants reported being uncertain about their future anymore, and this caused them stress. P 49 described her predicament as follows; “I have fears about leaving my child, ‘cos’ I want to see him grow up, I want to see him become something in future, get married, so that he achieves his goals, that’s what I pray for” and P 28 put it more clearer by saying; ‘’ I get stressed because I know that HIV kills.’’ These statements show how stressed participants were because of the HIV diagnosis, signalling the need of support measures to help them cope. Participants also had some misconceptions about HIV, like P 81 who described the reason for her being stressed in the following statement;
The experiences for P 81 show a mixture of constant fears that include; fear of death, fear of infecting the family and fear to disclose the HIV diagnosis which can lead to reduced quality of life. Some of the fears are unfounded, like fear of transmitting the virus through eating utensils, heralding the need for continuous dissemination of HIV news and management to the masses. For a pregnant woman, taking the medicine reduces the chances of vertical transmission of the virus. However, daily dosing with antiretroviral medication was cited as a source of stress for some of the participants as follows;
2.3 Vertical transmission and breastfeeding
Participants experienced mixed feelings about the efficacy of the ARVs which they were taking to prevent mother to child transmission of the virus. . P 104 described being stressed about the health of her baby by saying, “it stresses me because it is a chronic and untreatable disease. I think a lot of thoughts about my baby. Will she grow up? I pray always that she will not be infected”. Additionally, P 45 expressed her helplessness in preventing infection to her baby and said, “I just don’t want him to acquire this. I just have that ka (small) fear, may be through breastfeeding, I can infect him, though they say it’s not…I just want my baby to be okay”. In spite of being counselled about the relative safety of breastfeeding in an HIV positive status, the above statements show that mothers were not totally convinced about prevention of Mother-to-Child transmission of the virus by taking ARVs and this calls for continued counselling to help reduce the stress levels experienced by the women as most mothers will always want the very best for their children.
Other participants were stressed about breastfeeding concerns. Mothers obtain a lot of satisfaction from breastfeeding their new-borns as most of them have been rightly socialised that breast milk is the best feed for a new-born infant. HIV positive women need to be supported for them to cope when they have chosen an alternative feeding method for their baby in an effort to prevent infection to the baby. Inability to breastfeed leads to stress in both mothers and babies as admitted by some of them;
2.4 Baby’s pain
The stress of an HIV diagnosis was also to do with painful procedures on the baby, like drawing blood for HIV testing and mothers anguished at seeing the suffering of their babies, like P 39 who said, “Sometimes he cries and then I feel bad that I am failing him. Especially at discharge when they drew blood from him, he was crying and I felt that I am the cause for his pain.” This participant was discharged in an anguished state as she blamed herself for her baby’s pain, with no one noticing what she was going through. It is important for Health care providers to create rapport with their clients so that they can feel free to ventilate to them when they are troubled.
Theme 3: Making the HIV positive status known
Informing significant others about one’s HIV positive diagnosis is encouraged, mostly for ART adherence, coping assistance, and protection/treatment of the sexual partner. Disclosure of HIV positive status leads to varied reactions among those to whom the client discloses. Some participants disclosed to their sexual partners, some to their mothers and others to their workmates.
Participants were asked about the reactions of significant others upon informing them of their HIV positive status. The participants who disclosed to their sexual partners reported various reactions from them as discussed below;
3.1 Intimate partner violence
Some participants reported emotional violence by their partners, like P 21 who stated; “he told me not to tell anyone else but it saddens me when I can’t inform my relatives, and I know that he already knew his positive status.” Others, like P 23 reported mental torture and said; “he tortured me mentally, he was moody” (P 23), and P 5 who said;
Participants like P 5 would be asked to bring their husbands along for the test before disclosing if they expressed fear and uncertainty about the reactions of their husbands once they disclosed. Being diagnosed HIV positive during a routine antenatal care visit is stressful enough, but the stress and pain are increased by unsupportive husbands, who are supposed to console their wives. Therefore couple counselling and explaining the need to support their wives to husbands can be cardinal in reducing the stress in the pregnant woman.
3.2 Emotional reactions and stigmatisation
Some of the participants described emotional reactions which included turmoil and disbelief in their partners upon informing them of their positive status, like P 18 who had this to say;
Other spouses disbelieved and were shocked about the test results, like the husbands to P 40 and P 49 as stated by their wives, “he refused that it is not true and said that we needed to go together for the test”(P 40) and P 49 said, “he was in shock as well.” However, other participants reported receiving a lot of support from their partners, like P 44 who said; “ he took it lightly and encouraged me” (P 44). This shows that men also need a lot of support and counselling from Health care providers and significant others once their wives test HIV positive.
Emotional reactions and stigmatisation were also reported from other relatives and friends to whom participants disclosed and the emotional reactions were varied, including anger and disappointment, stigmatisation and disbelief as stated below;
3.3 Disclosure worries and concerns
Sometimes, patients who are diagnosed HIV positive fail to disclose to others for various reasons. Participants expressed discomfort/ hesitation in disclosing their diagnosis to other people and reasons cited included uncertainty about ensuing marriage relationship, fear of the unknown, dilemmas about origin of the infection and inability to trust people. Some participants explained their hesitation to disclose as stated below;
Other participants could not bring themselves to trust people with their information, like P 13 who answered; “no, I have not informed my family because I know their thinking and behaviours, I can’t trust them with my information. I have 2 sisters and 3 brothers, am the 3rd born. Our parents died” (P 13). This indicates the lack of support that may occur in families which can hinder the provision of emotional support to each other in times of need.
Theme 4: ART adherence
Adherence to antiretroviral medication is very important for viral suppression, better health outcomes, and PMTCT. Participants were asked questions about their ART experiences and adherence.
4.1 Facilitators to adherence
Participants explained what facilitated their ability to adhere, which included setting reminders. Their desire to prevent transmission of the virus to their babies was another reason. Setting reminders helped patients to remember to take their long term medications at the stipulated time and form a routine, which eventually integrated into their daily activities.
Participants 13 and 39 adhered to medication by setting an alarm for themselves, as explained; “I set an alarm for myself to help me remember to take the medicine” (P 13, P 39). Others adhered just for their baby’s sake as described by one of them; “but I love my baby, actually, I will say that he is my comfort and the reason for my adherence to medication” (P 39). These positive behaviours towards ART adherence should be encouraged to continue for clients’ better health and prevention of infection to the babies.
Participant 23 developed a psychological connection to taking the medicine and explained, “If I haven’t taken 20 minutes after I am supposed to take the medicine, I would feel itchy and start scratching. Asked when the itching would stop, she answered, “after I take, then the itching would stop about 45 minutes later” (P 23).
4.2 Hurdles to adherence
However, some participants had difficulties with adherence and described their challenges which included physical problems and forgetfulness.
Participant 21 experienced some side effects and explained, ‘’I experience dizziness and the bed would feel like it is going round and round. I feel dizzy so do not take the medicines sometimes’’ (P 21). Participants who reported problems with adherence due to experiencing side effects were referred for further attention to the In-charge.
Women who test positive for HIV should be encouraged and supported to disclose their positive status to their husbands to avoid the secrecy in taking the drugs which can lead to compromised adherence and increased risk of vertical transmission. Some participants, like P 18 had different hurdles with adherence and she had this to say;
Others would skip doses due to fear of stigmatisation as stated below;
These results show the reality of the fear of stigmatisation among clients who are diagnosed with HIV infection.
Theme 5: Staff behaviour
Health care workers play an important role in the lives of their clients, who usually pay attention to the advice given at the facility, and their attitude and practice play a vital role on how clients generally behave towards Health care. Participants were asked to describe the health care that they received during pregnancy, labour and delivery, and postpartum, with probes on why they described the care the way they did.
5.1 Supportive staff
Women described the staff behaviour during their course of care from antenatal, intranatal and postnatal periods as generally supportive, and expressed confidence in the ability of Health care workers to take good care of them as stated by some of them;
The supportive care of staff was further described as follows;
The above statements show the confidence of participants in their Health care providers which is good for the management of the HIV infection. Health care providers need to be applauded when they take good care of their clients to encourage them to continue.
5.2 Medical terms and procedures
Medical terms are used to describe conditions and procedures in medicine. Sometimes, Health care workers may get carried away and use the medical terms when speaking to clients, and participants complained about this as follows;
Other clients expressed disappointment at what they termed as lack of, or inadequate care from the providers, and inadequate explanations to the family on how they should care for the HIV positive woman, as expressed in the following sentiments; “though impolite, they treated me well. Sometimes, Health care workers are impolite and talk roughly to us. They offer no encouragement, no explanation about the disease or how to take care of the baby.” (P 14)
Participants also complained about not receiving their laboratory results on time, which affected some decisions that they had to make as stated below;
The Health care system always has trainees to sustain the health care profession, and they attend to clients during their training. However, their presence may cause fear in the clients as they are aware that the trainees may not have acquired the required competences as yet. Some participants had this to say; “during labour, I was afraid and I was just praying that they won’t make any mistake – there were a lot of students there which made me restless” (P 45).
In as much as participants described the Health care provision as good, others complained about the care that they received.
5.3 Rude staff
Others viewed staff as rude and less caring, though at times, they reported chancing staff who were good, which should not be the case, as expressed by some participants;
Theme 6: Adjusting to the reality of living with HIV
A diagnosis of HIV brings about changes in an individual’s life as they adjust to living with the virus. The mechanisms that are used by individuals to cope with a challenging situation are very important and can either help to reduce the stress, or make it worse.
6.1. Coping strategies
When asked questions on how they managed to cope with the stress of the challenging diagnosis of HIV during pregnancy, participants described how they managed to adjust their lives as follows;
6.1.1. Coping support
Participants mostly reported having good health and receiving support to cope from Health care workers, family and friends. They acknowledged the support of husbands too, while suspecting them of having infected them as some said; “my family supports me, including my husband. I think my husband is the one who brought the disease” (P 104).
Others explained their coping through self-encouragement, online resources and prayer, which is a helpful way of coping like P 13 who explained;
Even involvement in social activities, social media and informal groups where women meet and just talk randomly was cited as coping support by the participants, like P 45 who had this to say;
These results show the role that social media and informal groups play in shaping the lives of people and in helping the affected to cope with the stress of an HIV diagnosis. In the current age and era, people look for health related information on a number of sources, including social media.
6.1.2 Psychological resilience and moving on
Being resilient is important in helping people to forge ahead and live normally despite adverse circumstances. Participants became resilient and determined to live their lives on after being diagnosed with HIV.
Participant 40 stated; “I am trying by all means to live a normal life and take the medicine. I have told myself that I will take the medicine and live my life on in this world” (P 40).
Other participants described their coping by accepting the fact that they had seroconverted to being HIV positive, as represented below;
When women diagnosed HIV positive use their own coping resources, they tend to cope better and their stress levels reduce as they actively seek solutions to the problem of living with HIV.
6.2 Difficulty coping
Sometimes, coping with a challenging situation is difficult for various reasons. Some of the participants had difficulties coping for reasons which included depression and loss of the baby, as expressed by P 40, “the death of my baby has affected me, I think a lot. I feel overloaded. I had too much medication. Labour was induced and was very painful” (P 40). These findings show that women who are diagnosed with HIV during pregnancy may undergo a lot of stress and depression which can overstretch their coping mechanisms and lead to failure to cope.
DISCUSSION
This discussion is based on the findings from in-depth interviews that were conducted to explore the experiences of women who were diagnosed HIV positive at a routine antenatal care visit during their most recent pregnancy. Women reported experiencing stress at their HIV positive status due to various reasons, topped by fear on infecting their babies, fear of stigmatisation and uncertainty about the future. Participants reported disclosing their HIV positive status to their significant others which brought about various reactions, including emotional violence from their husbands. They also reported adhering to the ART regimen, particularly for the sake of their babies, and reported their relationship with Health care providers as both being supportive, and sometimes unsupportive.
Demographic characteristics
The demographic characteristics for the participants are found in Table 1 and majority (15: 88.2%) of them were in the age group 18 to 35 years, which is the safest childbearing age, when women are neither too young, with reproductive organs still developing, nor too old, when degenerative processes as a result of aging have begun in their body, which can lead to complications, adverse pregnancy outcomes, and add to the stress of an HIV positive diagnosis[18] . Most (14: 82.4%) of them were religious, which could help them cope with an HIV positive diagnosis, like P 13 and P 17 who mentioned obtaining help to cope through friends at church and praying a lot. Religiosity has been found to be helpful in managing stressful situations as the affected learn to trust God for sustenance, and tend to cope better with adverse situations[19] .
A number of participants (11; 64.8%) attained secondary education and 13 (76.4%) resided in medium density areas. The residential area may have an effect on how women cope, with those in high and medium density areas having a lot of neighbours to talk to from time to time, easing their stress. Participants mentioned chatting away as one of the ways in which their stress was relieved (P 7). On the other hand, women residing in low density areas may mostly be lonely and constantly thinking about their HIV diagnosis and getting more stressed, like P 18 who reported that she was lonely, and highly stressed. This is in contrast to the findings by Cyimana et al who found that low residential density was associated with lower prevalence of severe postnatal depression[20] . The majority (11:64.7%) of the participants were married as marriage is the recognised place for procreation in the Zambian culture, however, this signifies a higher HIV infection rate among married women. Coupled with other demographic characteristics, like level of education, married couples face a substantial risk of contracting HIV from their partners[21] . In a marriage relationship, couples are expected to be faithful to each other, but most often, they have extra marital affairs and polygamous unions, which put them at risk of acquiring sexually transmitted infections, including HIV. In this study, couples suspected each other of having infected them, like P 5’s husband who accused her of having infected him, and P 21 who reported that the husband implored her not to tell anyone else about the HIV diagnosis because he, supposedly, had prior knowledge about his own HIV positive status. In as much as married women were more at risk of acquiring the virus, single women are equally at risk as discovered by Tlou and Wand et aL, hence, HIV prevention messages should continue to be given to all, regardless of their marital status[22,23] .
Experiences of women diagnosed HIV positive during pregnancy
Participants described their experiences with an HIV diagnosis that was made during pregnancy and most of them reported moderate to high levels of stress. Women explained being particularly stressed about an HIV diagnosis due to its lack of cure, uncertainty about their pregnancy outcome, intimate partner violence, fear of infecting their babies, inability to breastfeed and fear of death. This is similar to other studies which found stress and psychological challenges in perinatal women with HIV[24,25] . Some participants reported their shock at being diagnosed HIV positive, and even blamed the pregnancy for their positive status (P 17, P 104), as they reported having been HIV negative before pregnancy. This may mean that women were not testing regularly and did not notice when they seroconverted, but if they were truly infected during the pregnancy, the consequences could be increased risk of vertical transmission as transmission is highest in newly infected patients, calling for continued counselling on adherence to ART. Attributing their HIV positive status to the pregnancy could lead to unhappy feelings about it, which can eventually affect the development of the mother baby bond as bonding begins during pregnancy. However, some women had low stress levels, mostly because they appraised the HIV as a virus that can be controlled to enable them lead a normal life. Some of the participants felt stigmatised by their loved ones when they informed them of their diagnosis or indeed self-stigmatised, like P 45 who said that she was definite that people would talk about her HIV positive status. Similarly, Jolle et al found that social rejection and public ridicule were identified as HIV related stigma experiences[26] . The fear of HIV related stigma is real among the affected, and sometimes even affects ART adherence as reported by the study participants, like P 5, and hence Ministries of Health would do well to help demystify HIV[27-30] . Others never accepted, like P 40 who reported that her feelings were telling her that the diagnosis is not true, and that she would still go to another Health facility to test. During the study period, some women took long to come back for their next visits, or were lost to follow-up as they were still going to other centres to book again for antenatal care and retest for HIV due to denial of the positive results which they received. One such client kept going round the Health facilities after being diagnosed with HIV, hoping to get different results, and only reappeared at Chilenje with an inevitable abortion which became complete when she just arrived. Similarly, Madiba found non-acceptance for extended periods among South African pregnant women diagnosed HIV positive during pregnancy[31] . Failure to accept the diagnosis can lead to non-adherence to medication, or not taking the medication at all, which can have adverse health consequences for the mother and her baby. There is need for the Ministry of Health to digitalise clients’ records onto a national system which can allow detection/tracking of participants once they book for antenatal care, to save them the stress of booking at so many Health facilities in the hope of getting a negative test result.
Participants also reported disclosing their HIV status to their spouse and significant others, and described their experiences with disclosure, with most of them being given the support that they needed. Similarly, Mwamba et al found that 93% of HIV positive pregnant women were willing to disclose to at least one person[32] . Disclosure usually helps clients to cope with the stress because they will have nothing to hide, and may receive the support to cope in living with the condition. In his study, Zotova et al found that, disclosure was higher among participants diagnosed prior to their current pregnancy relative to those diagnosed during current pregnancy, and higher depressive symptoms were found among women diagnosed during their current pregnancy who disclosed to their partners[33] . These results support the grief model by Kubler-Ross (1969) where newly diagnosed women could have been in the early stages of the grief over loss of their old self and failed to immediately disclose the diagnosis. However, in the current study, most participants reported having disclosed their positive status to their spouse. Some participants reported emotional violence from their partners after disclosure which led to high stress levels, like P 23 who reported mental torture from her spouse, and P 5 whose husband kept accusing her of having infected him to the extent that she developed high blood pressure, left her marriage and miscarried. On the contrary, one study found that disclosure to their partners eased the stress from women[34] . This discrepancy of the results could be in the study populations that differed between the studies. Madiba and Putsoane conducted their study on adolescents and young women whose spouses could also be younger in age, and may not have really understood the gravity of the situation, while the current study was conducted on women of child bearing age. Most women disclosed to their relatives and reported various reactions, which included anger. P 23 reported that her mother was angry about her having been infected, but there was nothing that she could do since the daughter was married. This suggests the need for family centred care when managing women who are diagnosed with HIV infection during pregnancy, as other family members may equally be hurting and needing support. .
Health care providers should therefore continue encouraging the disclosure of an HIV positive diagnosis and also support by the significant others for the affected to help them cope with the stress that comes with an HIV positive diagnosis during pregnancy.
The World Health Organization[35] recommends consistent daily dosing with antiretroviral medication for optimum viral load suppression. People living with HIV who achieve an undetectable level of virus by consistent use of antiretroviral therapy are less likely to transmit HIV to their sexual partner(s) and are at low risk of HIV vertical transmission to their children[34] . Most participants reported adhering to their ARVs and reasons for adherence included doing so for the sake of the baby. However, participants also reported some problems that they had with adherence which included daily dosing, experiencing side effects, forgetting and fear of stigmatisation. This is similar to what Knettel et al found that stigmatisation negatively affected retention in HIV care[29] . Participants recommended long lasting injectable ARVs to reduce on daily dosing and forgetting to take the medication.
The experiences with staff were also described, with participants reporting both support and inadequate support from staff (Table 2). In their study, Nyarko et al found that women had insufficient knowledge on importance of exclusive breastfeeding, when HIV transmission occurs and the merits of Caesarean section in PMTCT[36] . These findings, though obtained from pregnant women who might have been HIV negative reveal the inadequate explanations that are given to clients by the Health care workers. In the current study, women reported lacking knowledge on the medical terms and procedures because they were not explained to them by the Health workers. Participant 14 said that Health care workers should take time to explain the disease to the women, and teach them how to take care of their babies. This was resounded by P 9 who reported that Health professionals should take time to explain what is expected of the patients and also explain the medical terms to clients to make them understand. These findings are similar to what Nyamathi et al found among Indian women living with HIV who described the challenges that they face with obtaining and maintaining care and recommended educational services for women living with HIV[37] . Another study, though not conducted on postnatal women living with HIV, by Asadi et al, which explored HIV patients’ experiences of receiving Health care services equally found inappropriate behaviour of Health care staff towards patients[38] . In South Africa, Ndou et al also found negative experiences concerning the practices by Health care providers in a qualitative study that explored the perceptions of HIV positive patients of the care received at one of the clinics[39] . This therefore calls for Health care providers to give women information at their level of understanding so that they know whatever is being done on them. Staff were reported to be rude by some participants like P 49 who said that this made the women to feel stigmatised. When women feel stigmatised by Health care providers, or when they receive disrespectful and humiliating care, they can end up not returning to the Health facility. This can result in tension between Health care providers and clients and lead to other consequences like loss to follow up and home births that can be detrimental to the health of the mother and her baby as they will not receive the HIV care package as appropriate. There is need for Health care providers to remain professional all the time and mind how they talk to the clients. Alexis and Hope also found negative attitude towards pregnant women with HIV among medical practitioners in Cameroon. Similarly, Aleebrahim revealed that more than half of the nurses and midwives recruited in the study had moderately stigmatising attitudes towards people living with HIV and that midwives were very concerned about participating in a delivery by an HIV infected mother40, [41] . Overall, participants reported to have received good care from the providers in the current study, however, there is need for Health care providers to maintain a professional and empathetic attitude towards their clients at all times.
Some participants reported coping positively with the stress of an HIV diagnosis that was made during pregnancy, and described their coping support which included good physiological health, support from family, health care workers, online resources and even informal and social media groups. These results are similar to findings by Ashaba et al who reported that women coped through support from partners, family and friends, and also by being self-reliant[42] . Another similar study by Tong et al, though conducted on HIV positive Health Workers to explore their coping strategies found that they coped, among others, by seeking social support and applying problem-solving strategies[43] . This signifies the need for Health care providers to develop mechanisms to ensure that correct information about HIV and its management is shared on social media. Support from Health care workers is valued and would benefit the clients because it is professional and gives factual information on how clients should care for themselves. However, other participants reported inability to cope with the stress and some of them reported just avoiding to think about their HIV positive status. While avoiding could help for some time, the problem does not go away, and can result in adverse outcomes. Some participants reported adverse conditions and pregnancy outcomes which they attributed to the stress of an HIV positive diagnosis (P 5, P 18). Therefore, mental health care should be incorporated routinely in the management of women who are diagnosed with HIV during pregnancy, similar to what Akinsolu et al’s study has recommended[44] .
LIMITATIONS OF THE STUDY
Inadequate literature with regards HIV diagnosis during pregnancy, and the experiences of women which limited the literature review and the discussion of findings in light of existing literature. This was mitigated by using related literature.
The study was conducted in an urban setting, so generalisation to rural settings should be done with caution. This was minimised by using thick descriptions to allow the readers to judge the similarities of the study setting with other settings
Staff were not interviewed who could have added their observations on experiences and management of women diagnosed with HIV during pregnancy. This limitation was mitigated by creating rapport with participants and allowing them ample time to narrate their experiences which brought out rich information on what the participants were going through.
CONCLUSION
This study has brought out the experiences of women diagnosed with HIV during pregnancy at selected Health facilities in Lusaka district. Participants reported being stressed due to various fears, some reported Intimate Partner Violence upon disclosure to their sexual partners. Participants reported coping by assistance from Health care providers, family and friends, and from within themselves. Staff were generally described as being supportive, though some of them were reported to be rude.
The study recommends empathetic support to mothers who are diagnosed HIV positive during pregnancy, together with their significant others to help them cope with the stress that comes with an HIV positive diagnosis during pregnancy.
What is already known on this topic
Women experience psychological distress with a perinatal HV diagnosis.
What the study adds
This study provided information on experiences and what stresses women after being diagnosed with HIV during pregnancy, through to their 6th week postnatal visit in Lusaka district, and how they coped.
How the study might affect research, practice or policy
Participants reported stigmatisation from both Health workers and the community, and incorrect information on acquisition and management of HIV. Health care workers should continue sensitising communities to support women diagnosed with HIV during pregnancy and provide empathetic support to their clients. Midwives should ensure that correct information about HIV and its management is provided to perinatal women.
DECLARATIONS
ACKNOWLEDGEMENTS
I am indebted to Prof. Margaret C. Maimbolwa and Prof. A. Akakandelwa for their mentorship and practical advice. I thank the Lusaka District Health Office and the study sites for permitting me to conduct the study, and I sincerely thank my participants for taking part in the study. I am grateful to my employers, the University of Zambia for allowing and partly sponsoring my studies. I sincerely thank the NORHED project for partly sponsoring my studies too.
COMPETING INTERESTS
The authors declare that they have no competing interests.
REFERENCES
- Peirce A. The emotional impact of an HIV diagnosis. 2019. Available from https://www.everydayhealth.com/hiv-aids/hiv-diagnosis-emotional-impact.aspx Accessed 12 March 2021.
- HRSA. HRSA’S Ryan White HIV/AIDS Program. Addressing HIV Stigma and Discrimination to End the HIV Epidemic. Care Action Newsletter/November 2020. Available from https://hab.hrsa.gov/sites/default/files/hab/Publications/careactionnewsletter/care-nov-2020-newsletter.pdf. Accessed 1 August 2021
- Engidaw NA., Mekonnen AG. & Amogne FK. Perceived stress and its associated factors among pregnant women in Bale zone Hospitals, Southeast Ethiopia: a cross-sectional study. BMC Res Notes 12, 356 (2019). Available from https://doi.org/10.1186/s13104-019-4383-0. Accessed 24 October 2023
- Marshall J. and Raynor M. Myles Textbook for Midwives. 16th Edition. 2014. Churchill Livingstone. Edinburgh. ISBN 9780702051456
- Mukosha M, Chiyesu G, Vwalika B. Adherence to antiretroviral therapy among HIV infected pregnant women in public health sectors: a pilot of Chilenje level one Hospital Lusaka, Zambia. Pan Afr Med J. 2020 Feb 19;35:49. doi: 10.11604/pamj.2020.35.49.20078. PMID: 32537054; PMCID: PMC7250199. Accessed 12 March 2021
- Benson C, Wang X, Dunn KJ, Li N, Mesana L, Lai J, Wong EY, Chow W, Hardy H, Song J, Brown K. Antiretroviral Adherence, Drug Resistance, and the Impact of Social Determinants of Health in HIV-1 Patients in the US. AIDS Behav. 2020 Dec;24(12):3562-3573. doi: 10.1007/s10461-020-02937-8. PMID: 32488554. Accessed 1 August 2021
- Okawa S, Chirwa M. Ishikawa N, Kapyata H, Msiska CY, Syakanntu G, Miyano S, Komada K, Jimba M, Yasuoka J. Longitudinal adherence to antiretroviral drugs for preventing mother-to-child transmission of HIV in Zambia. BMC Pregnancy Childbirth 15, 258. 2015. https://doi.org/10.1186/s12884-015-0697-7. Accessed 12 March 2021
- Kotzé M, Visser M, Makin J, Sikkema K, Forsyth B. Psychosocial variables associated with coping of HIV-positive women diagnosed during pregnancy. AIDS Behav. 2013 Feb;17(2):498-507. doi: 10.1007/s10461-012-0379-7. PMID: 23196861; PMCID: PMC4238922. Accessed 1 August, 2021
- Zambia Statistical Agency, Ministry of Health (MOH) Zambia, and ICF. Zambia Demographic and Health Survey2019, Lusaka, Zambia and Rockville, Maryland, USA, Zambia Statistical Agency, Ministry of Health and ICF.
- Central Statistical Office (CSO) [Zambia], Ministry of Health (MOH) [Zambia], and ICF International. Zambia Demographic and Health Survey 2013-14. Rockville, Maryland, USA: Central Statistical Office, Ministry of Health, and ICF International. 2014
- Akatukwasa C, Getahun MEl, Ayadi AM, Namanya J, Maeri I, Itiakorit H, et al. Dimensions of HIV-related stigma in rural communities in Kenya and Uganda at the start of a large HIV ‘test and treat’ trial. PLoS ONE 16(5): e0249462. 2021 https://doi.org/10.1371/journal.pone.0249462 Accessed 14 September 2021
- Weiss NH, Peasant C, and Sullivan TP. Intimate Partner Violence and HIV-Risk Behaviors: Evaluating Avoidant Coping as a Moderator. AIDS Behav 21, 2233–2242 2017. https://doi.org/10.1007/s10461-016-1588-2 Accessed 14 September 2021
- Chilenje Action Plan and Budget 2022
- Kanyama Health Management Information System data 2022
- Thomson G, Dykes F and Downe S. Qualitative Research in Midwifery and Childbirth. Phenomenological approaches. Routledge. London and New York. ISBN 978-0-415-57501-0 (hbk). ISBN 978-0-415-57501-0 (hbk). 2011. Available from www.bcbi.nlm.nih.gov/pubmed/?term=jenny-Makin. Accessed on 14 September 2021
- Polit, DF and Hungler, BP. Essentials of nursing research. Methods, Appraisal and Utilization. Fourth edition. 1997. Lippincott. Philadelphia. ISBN 0-397-55368-4Pp 303-308.
- Clarke V and Braun V. Teaching thematic analysis: Overcoming challenges and developing strategies for effective learning. The psychologist. 2013 Sep 2;26(2):120-3. ; 2013. Available from https://uwe-repository.worktribe.com/preview/937606/Teaching%20. Accessed on 1 August 2023.
- Zhang X, Liu KB, Liu FJ, Yang HJ, Yu Y. [Clinical characteristics and pregnancy outcomes of pregnant women in different age groups in Beijing]. Zhonghua Fu Chan Ke Za Zhi. 2018 Jul 25;53(7):452-458. Chinese. doi: 10.3760/cma.j.issn.0529-567x.2018.07.003. PMID: 30078254. Accessed on 1 August 2023
- Ironson G, Kremer H, Lucette A. Relationship between Spiritual Coping and Survival in Patients with HIV. J Gen Intern Med. 2016 Sep;31(9):1068-76. doi: 10.1007/s11606-016-3668-4. Epub 2016 May 5. PMID: 27149968; PMCID: PMC4978670. Accessed 30 May 2021
- Cyimana A, Andrews B, Ahmed Y, Vwalika B. HIV/AIDS and Postnatal Depression at the University Teaching Hospital, Lusaka, Zambia. Med J Zambia. 2010; 37 (2):78-83. PMID: 23226901; PMCID: PMC3515762. Accessed 25 January 2024
- Nabukenya AM, Nambuusi A, Matovu JKB. Risk factors for HIV infection among married couples in Rakai, Uganda: a cross-sectional study. BMC Infect Dis 20, 198 2020. https://doi.org/10.1186/s12879-020-4924-0
- Tlou B. The influence of marital status on HIV infection in an HIV hyperendemic area of rural South Africa, 2000-2017. Afr J AIDS Res. 2019 Mar;18(1):65-71. doi: 10.2989/16085906.2018.1559209. PMID: 30880581.
- Wand H, Morris N, Moodley J, Naidoo S, Reddy T. Impact of marital status on risk of HIV in South Africa (2002-2017). AIDS Care. 2023 May;35(5):739-744. doi: 10.1080/09540121.2022.2067312. Epub 2022 May 3. PMID: 35503713.
- Waldron EM, Miller ES, Wee V, Statton A, Moskowitz JT, Burnett-Zeigler I. Stress, coping and the acceptability of mindfulness skills among pregnant and parenting women living with HIV in the United States: A focus group study. Health Soc Care Community. 2022 Nov; 30(6):e6255-e6266. doi: 10.1111/hsc.14063. Epub 2022 Oct 10. PMID: 36214377; PMCID: PMC10092748.
- Ashaba S, Kaida A, Coleman JN, Burns BF, Dunkley E, O'Neil K, Kastner J, Sanyu N, Akatukwasa C, Bangsberg DR, Matthews LT, Psaros C. Psychosocial challenges facing women living with HIV during the perinatal period in rural Uganda. PLoS One. 2017 May 1; 12(5):e0176256. doi: 10.1371/journal.pone.0176256. PMID: 28459866; PMCID: PMC5411062.
- Jolle J, Kabunga A, Okello TO, Kadito EO, Aloka J, Otiti G, Aluku AA, Kumakech E, Udho S. HIV-related stigma experiences and coping strategies among pregnant women in rural Uganda: A qualitative descriptive study. PLoS One. 2022 Oct 7;17(10):e0272931. doi: 10.1371/journal.pone.0272931. PMID: 36206276; PMCID: PMC9543605.
- Kalichman SC, Katner H, Banas E, Hill M, Kalichman MO. HIV-related stigma and non-adherence to antiretroviral medications among people living with HIV in a rural setting. Soc Sci Med. 2020 Aug; 258:113092. doi: 10.1016/j.socscimed.2020.113092. Epub 2020 May 30. PMID: 32585544; PMCID: PMC8571810.
- Pantelic M, Steinert JI, Park J, Mellors S, Murau F. 'Management of a spoiled identity': systematic review of interventions to address self-stigma among people living with and affected by HIV. BMJ Glob Health. 2019 Mar 19; 4(2):e001285. doi: 10.1136/bmjgh-2018-001285. PMID: 30997170; PMCID: PMC6441299.
- Knettel BA, Cichowitz C, Ngocho JS, Knippler ET, Chumba LN, Mmbaga BT, Watt MH. Retention in HIV Care during Pregnancy and the Postpartum Period in the Option B+ Era: Systematic Review and Meta-Analysis of Studies in Africa. J Acquir Immune Defic Syndr. 2018 Apr 15; 77 (5):427-438. doi: 10.1097/QAI.0000000000001616. PMID: 29287029; PMCID: PMC5844830.
- Monteiro S, Villela W, Soares P, Pinho A, Fraga L. 'Protective' silence surrounding AIDS: Reasons and implications of non-disclosure among pregnant women living with HIV in Rio de Janeiro (Brazil). Glob Public Health. 2018 Jan; 13(1):51-64. doi: 10.1080/17441692.2016.1211163. Epub 2016 Jul 25. PMID: 27455879.
- Madiba S. When Pregnancy Coincides with Positive Diagnosis of HIV: Accounts of the Process of Acceptance of Self and Motherhood among Women in South Africa. Int J Environ Res Public Health. 2021 Dec 9; 18 (24):13006. doi: 10.3390/ijerph182413006. PMID: 34948615; PMCID: PMC8700982.
- Mwamba RN, Sao SS, Knettel BA, Minja LM, Osaki H, Mmbaga BT, Watt MH. The Disclosure Dilemma: Willingness to Disclose a Positive HIV Status among Individuals Preparing for HIV Testing During Antenatal Care in Tanzania. AIDS Behav. 2021 Mar;25(3):908-916. doi: 10.1007/s10461-020-03058-y. Epub 2020 Oct 3. PMID: 33011883; PMCID: PMC7886955.
- Zotova N, Familiar I, Kawende B, Kasindi FL, Ravelomanana N, Parcesepe AM, Adedimeji A, Lancaster KE, Kaba D, Babakazo P, Yotebieng M. HIV disclosure and depressive symptoms among pregnant women living with HIV: a cross-sectional study in the Democratic Republic of Congo. Journal of the International AIDS Society, 25(2), e25865. 2022. https://doi.org/10.1002/jia2.25865 Accessed 24 October 2023.
- Madiba S, Putsoane M. Testing Positive and Disclosing in Pregnancy: A Phenomenological Study of the Experiences of Adolescents and Young Women in Maseru, Lesotho. AIDS Res Treat. 2020 Feb 12;2020:6126210. doi: 10.1155/2020/6126210. PMID: 32099675; PMCID: PMC7037533.
- World Health Organisation. HIV and AIDS Key fact sheets. 2023. Available from https://www.who.int/news-room/fact-sheets/detail/hiv-aids
- Nyarko V. Knowledge, attitudes and practices regarding the prevention of mother-to-child transmission of HIV among pregnant women in the Bosone Freho District in the Ashanti region of Ghana: a descriptive cross-sectional design. PAMJ-Clinical Medicine. 2019:1:69. [doi: 10.11604/pami-cm.2019.1.69.20659]. Available from https://www.clinical-medicine.panafrican-med-journal.com/content/article/1/69/full
- Nyamathi A, Thomas B, Greengold B, Swaminathan S. Perceptions and health care needs of HIV-Positive mothers in India. Prog Community Health Partnersh. 2009 Summer;3(2):99-108. doi: 10.1353/cpr.0.0067. PMID: 20208256; PMCID: PMC7727722.. available from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7727722/
- Asadi H, Imani-Nasab MH, Garavand A, Hasoumi M, Kia AA, Haghi B, Setoodehzadeh F. HIV positive patients’ experiences of receiving catre: A phenomenological study in Iran. 2018. DOI: 10.2174/1874613601812010150. Available from https://openaidsjournal.com/VOLUME/12/PAGE/150/FULLTEXT/
- Ndou TV, Maputle SM, Risenga PR. HIV-positive patients' perceptions of care received at a selected antiretroviral therapy clinic in Vhembe district, South Africa. Afr J Prim Health Care Fam Med. 2016 Apr 26;8(2):e1-6. doi: 10.4102/phcfm.v8i2.926. PMID: 27380841; PMCID: PMC4887595. Available from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4887595/
- Alexis D, and Hope JS. "“Knowledge, Attitudes, and Practices of Health Personnel of Maternities in the Prevention of Mother-to-Child Transmission of HIV...” (2018), by Elie Nkwabong, Romuald Meboulou Nguel, Nelly Kamgaing, and Anne Sylvie Keddi Jippe". Embryo Project Encyclopedia. 2021-04-06. ISSN: 1940-5030 https://hdl.handle.net/10776/13251
- Aleebrahim F, Nasirian M, Ramezani A. Nurses’ and midwives’ job satisfaction and stigmatizing attitudes towards HIV/AIDS in Yazd City, Iran, in 2020. HIV & AIDS Review. International Journal of HIV-Related Problems. 2023;22(2):160-167. doi:10.5114/hivar.2023.126543.
- Ashaba S, Kaida A, Burns BF, O'Neil K, Dunkley E et al (2017). Understanding coping strategies during pregnancy and the postpartum period: a qualitative study of women living with HIV in rural Uganda. BMC pregnancy and childbirth, 17(1), 138. https://doi.org/10.1186/s12884-017-1321-9. [Cited 2021 Jul 17]. Available from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5423027/
- Tong H, Zhou Y, Li X, Qiao S, Shen Z, Yang X, Zhang Q, Zeng C. Stress coping strategies and their perceived effectiveness among HIV/AIDS healthcare providers in China: a qualitative study. Psychol Health Med. 2022 Apr;27(4):937-947. doi: 10.1080/13548506.2021.1983184. Epub 2021 Sep 27. PMID: 34579602; PMCID: PMC8957619. Available from Stress coping strategies and their perceived effectiveness among HIV/AIDS healthcare providers in China: A qualitative study - PMC (nih.gov)
- Akinsolu FT, Abodunrin OR, Lawale AA, Bankole SA, Adegbite ZO, Adewole IE, Olagunju MT, Ola OM, Dabar AM, Sanni-Adeniyi RA, Gambari AO, Njuguna DW, Salako AO, Ezechi OC. Depression and perceived stress among perinatal women living with HIV in Nigeria. Front Public Health. 2023 Nov 20; 11:1259830. doi: 10.3389/fpubh.2023.1259830. PMID: 38054071; PMCID: PMC10694505.
Medical Journal of Zambia, Vol 51, 1
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.