Malaria prevalence and associated additional risk factors among children under-five years who sleep under insecticide treated nets in Zambia
Mukumbuta Nawa
Levy Mwanawasa Medical University, Department of Biostatistics and Epidemiology
Prudence Mpundu-Zimba
Levy Mwanawasa Medical University, Department of Biostatistics and Epidemiology
Cephas Sialubanje
Levy Mwanawasa Medical University, Department of Biostatistics and Epidemiology
DOI: https://doi.org/10.55320/mjz.50.4.439
Keywords:Insecticide Treated Nets, Under-five children, malaria, anaemia
ABSTRACT
Background: Insecticide Treated Nets are one of the backbones of malaria prevention in Africa where the vector mosquitos bite at night and prefer humans for feeding. Children who sleep under Insecticide Treated Nets though protected still get malaria infections. This study aimed to assess the risk factors of malaria infection among under-five children who sleep under insecticide-treated Treated Nets.
Methodology: This was a secondary analysis of a cross-sectional survey the Malaria Indicator survey of 2021 in Zambia. Data was extracted from the database at the Ministry of Health and analysed in STATA version 14. Data was analysed in counts and frequencies, cross-tabulations and associations assessed using logistic regressing using complex data analysis.
Results: A total of 1695 children aged below five years who had slept under an Insecticide Treated Net the night before the survey were included in the study, 50.9% were female while 49.1 were male. Over a third of them (23.9%) had a fever in the previous two weeks, over half 51.9% of them had anaemia and 28.8% of them had malaria infection tested using Rapid Diagnostic tests. There was a 3.46 (95%CI 2.67 – 4.49) increase in the odds of having malaria if the under-five child was anaemic (haemoglobin less than 11mg/dl). Other factors that are usually associated with malaria infection such as younger age group, low socio-economic status, residing in rural areas and having had a fever in the previous two weeks.
Conclusion: In Zambia, about a third of under-five children who slept under insecticide-treated nets still had evidence of malaria infection. A significant risk factor for malaria infection among the under-five children who slept under ITNs was anaemia. Other known risk factors for malaria among under-five children such as age, rural residence, wealth status, province of residence and education of guardians were not statistically significant.
INTRODUCTION
Malaria remains one of the most significant health challenges in developing countries, particularly affecting children under the age of five years and pregnant women[1] . Children under five years old are particularly vulnerable to severe malaria, which can lead to severe anaemia, cerebral malaria, organ failure, and death[2] . Children under the age of five are especially vulnerable to the devastating effects of malaria due to their developing immune systems and lack of previous exposure to the parasites[2] . The impact of malaria on this age group is profound, leading to frequent and severe episodes of illness, hospitalization, and long-term cognitive and physical impairments[3] . Malaria-related deaths in this demographic account for a significant portion of global child mortality, hindering efforts to achieve sustainable development goals related to child health and well-being[4] .
Despite considerable progress in malaria control efforts, it remains a leading cause of morbidity and mortality, disproportionately affecting regions with limited access to healthcare, such as sub-Saharan Africa and parts of Southeast Asia. Recent global statistics on malaria show that over 95% of all malaria cases reported in 2020 were from sub- Saharan Africa and Asia[5] . Over two-thirds of the global malaria burden of malaria cases are concentrated in ten African countries namely Burkina Faso, Cameroon, the Democratic Republic of the Congo, Ghana, Mali, Mozambique, Niger, Nigeria, Uganda and the United Republic of Tanzania and in India[6] . Zambia is not one of the High Burden High Impact (HBHI) countries but borders three of the countries; mosquitoes know no boundaries and areas bordering these countries have the highest malaria prevalence in the country[7] . A recent survey in Zambia found that two in every three children had evidence of malaria antigens in the Luapula province which borders the Democratic Republic of Congo, and over 40% of the children in Muchinga and Northern Provinces which border Tanzania had malaria antigens[8] . The presence of malaria antigens in the blood as diagnosed by a Rapid Diagnostic Test (RDT) indicates that the person has an active malaria infection, is a chronic carrier or the individual is within a month of recovering from an infection[9] . Malaria is endemic in all parts of Zambia and has with peak seasons during rainy seasons from November to April[10] .
In the fight against malaria, Long Lasting Insecticide-treated Nets (LLINs) have emerged as a crucial tool for preventing infection alongside other interventions such as Indoor Residual Spraying[11] . These nets have insecticides and create a physical barrier between individuals and disease-carrying mosquitoes, reducing the likelihood of bites and subsequent transmission of the parasite[12] . The insecticides used in treated nets not only repel mosquitoes but also kill them on contact, further decreasing the mosquito population in the vicinity and interrupting the disease's transmission cycle[13] . Despite the proven effectiveness of LLINs in preventing malaria, several challenges persist in ensuring their widespread and consistent use, particularly among children under five[14] . Economic constraints, inadequate access to healthcare facilities, cultural beliefs, and logistical barriers can impede the distribution and utilization of mosquito nets[14] . Additionally, the emergence of insecticide- resistant mosquitoes poses a growing threat to the efficacy of these preventive measures, necessitating continuous research and adaptation of strategies[15] .
The adoption and proper use of mosquito nets among children under five have been shown to yield numerous benefits. Firstly, consistent use of nets significantly reduces the risk of malaria infection, leading to fewer episodes of illness, decreased hospitalization rates, and improved overall child health[16] . This, in turn, contributes to reduced healthcare expenditures and increased economic productivity within affected communities[17] . Moreover, the reduction in malaria cases alleviates the burden on healthcare systems and resources, allowing for a more targeted allocation of limited resources toward other healthcare needs[17] .
Whilst LLINs have been known to prevent malaria in children and other demographics of the population, it has been during surveys that even children who use them also develop it though with reduced odds. A recent systematic review and meta- analysis on the effectiveness of LLINs showed that they reduced the risk of malaria and the odds ratio among users was 0.44 (95% CI 0.41 – 0.48)[18] . Many studies have investigated the malaria prevalence and risk factors in children under five years of age, however, our study looked at the prevalence and additional risk factors among children who already use LLINs. The findings of our study will help the scientific community, governments and program implementers in malaria-endemic regions to understand further interventions for those already protected by LLINs especially as we go towards malaria elimination by 2030.
METHODOLOGY
Study Design
This is a secondary analysis of data collected during a survey called the Malaria Indicator Survey.
Study Settings
The study covered all the ten provinces of Zambia. It has a tropical climate and is covered by savannah grasslands, river valleys and forested plateau land. The climate and landscape are conducive to the breeding and proliferation of malaria mosquito vectors. The government carries out ITN mass distribution every three years and targeted annual indoor residual spraying to eligible areas and households as part of its malaria prevention efforts. Many people therefore have benefited from either the mass distributions of ITNs or the routine distribution to under-five children through immunisation clinics and antenatal clinics for pregnant women.
Sample Size
Our study was powered to detect malaria prevalence of 29.3% in under-five children based on the Malaria Indicator Survey of 2021 (MoH, 2021). We powered the study at 80% to detect at least a 10% difference at 95% confidence level at the provincial level and urban versus rural strata. We used the formula:
N = (p0 q0 + p1 q1 ) (zá/2 + zâ )2.df/ (p1 – p0 )2
Where n = number of respondents . p0 = proportion of respondents with no exposure = 29.3% malaria (MoH, 2021) . p1 = proportion of respondents with exposure = 10% difference . á = level of significance = 0.05 . â = power complement = 80% .df = design effect = 1.5
Sampling Procedure
We included all children who were included in the primary study who met our criteria based on the age of six to 59 months who had slept under a net the night before the survey.
Data Collection
We extracted the data from the Malaria Indicator Survey database at the National Malaria Elimination Centre into Microsoft Excel and then imported it into Stata for cleaning and analysis. The primary survey used a questionnaire that was administered by trained research assistants.
Data Analysis
The data was analysed in Stata software version 14 using complex data analysis to account for the multistage sampling. We conducted descriptive statistics using counts, percentages, mean or median and confidence intervals depending on the distribution. We did parametric or non-parametric hypothesis tests to compare among sample groups depending on the distribution of the variable. For associations, we used logistic regression using stepwise forward model building by conducting univariate and multivariable analysis. A P-value of 0.05 was considered significant.
Ethical Considerations
The data was anonymised with coded identity numbers that were not traceable to the participants. In the primary survey, the heads of the households consented to participate in the study. The study had ethical clearance from the University of Zambia Biomedical Ethics Committee (UNZABREC).
RESULTS
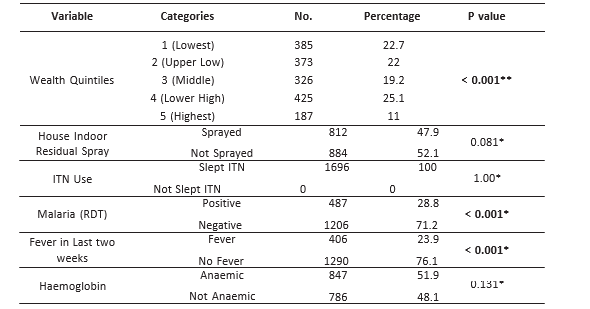
A total of 1, 696 under-five children were included in the study who had slept under insecticide-treated nets (ITNs) the night before the survey, of these, 864 (50.9%) were female and 832 (49.1%) were male and the proportions were not statistically different (P-value = 0.484). By age group, the composition was statistically different, the lowest were children below one year at 290 (17.1%) and the most were 429 (25.3%). The majority of heads of households had no or just primary level education 938 (65%) and very few 48 (3.3%) had tertiary level education. Similarly, the majority of the children resided in rural areas 1,572 (92.7%) compared to urban dwellers who were only 124 (7.3%). In terms of provinces, all provinces were represented, Lusaka province had the least number of respondents 63 (3.7%) and the highest were from Eastern province 291 (17.2). The poorest quintile was 385 (22.7%) whilst the highest quintile was only 187 (11%). Further, amongst these under-five children who had slept in ITNs the previous night, almost half stayed in indoor residual sprayed houses 812 (47.9%) compared to 882 (52.1%) who stayed in houses which were not sprayed with residual insecticides. In addition, 487 (28.8%) of them tested positive for malaria using Rapid Diagnostic Tests (RDTs), 406 (23.9%) had an episode of fever in the two weeks preceding the survey and 847 (51.9% had anaemia at the time of the survey. Table 1 summarises the baseline characteristics of the respondent children.
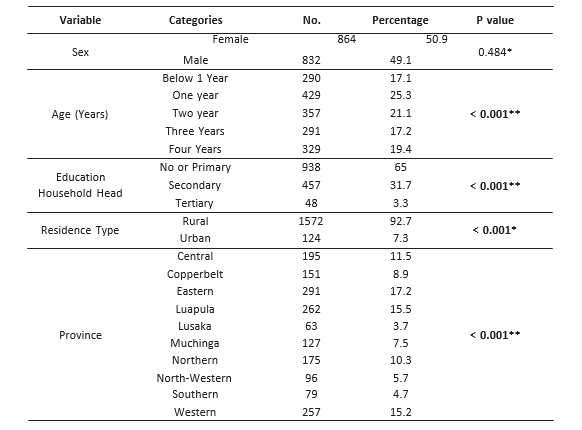
 * Test of Proportions
** Multiple Proportions Test (Marascuilo Procedure)
* Test of Proportions
** Multiple Proportions Test (Marascuilo Procedure)
When the data was stratified by malaria diagnostic results (RDT), there were no significant statistical differences by sex, age- group, education of household head, urban or rural residence, province, wealth quintile and whether a child had fever or not. However, there were significant statistical differences among those who had indoor residual spraying (P value = 0.004) and anaemia (P-value < 0.001). Table 2 summarises the cross-tabulations of different independent variables and the outcome variable rapid diagnostic test result.
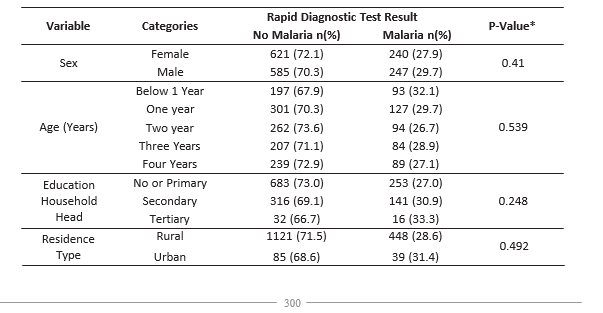
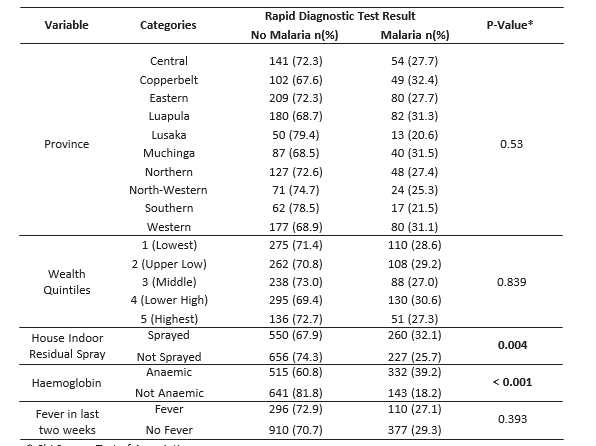 * Chi Square Test of Association
* Chi Square Test of Association
There were no statistically significant differences between female and male under-five children in the odds of malaria who slept under ITNs. Similarly, there were no differences in the odds of malaria among the different age-groups from infants, those who were aged one, two, three and four years. Other variables such as wealth quintile, residing in urban or rural areas, and educational levels of the heads of the households were also not statistically significant. In high-prevalence provinces such as Luapula and Northern Provinces, the odds of malaria were higher compared to Southern province, however, these were not statistically significant implying that the effects of ITNs significantly reduced the risk of malaria even in these high-burden provinces. Children who stayed in houses that were sprayed with residual chemicals and also slept under ITNs were associated with reduced odds of malaria, however, this was not statistically significant. On the other hand,children who were anaemic and slept under ITNs were still associated with 3.46 times higher odds of malaria and this was statistically significant. Table 3 summarises the unadjusted, adjusted odds ratios and the 95% confidence intervals of the odds ratios of different variables that were included in the study.
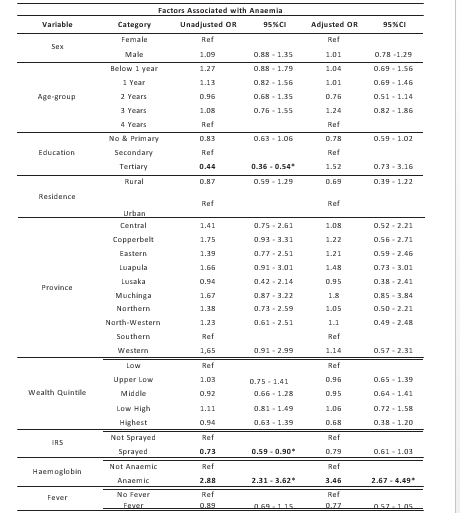 *Statistically Significant Odds Ratios and Confidence Intervals
*Statistically Significant Odds Ratios and Confidence Intervals
DISCUSSION
Insecticide Treated Nets (ITNs) are one of the cornerstone preventive tools against malaria, however, they are not the only ones and even people who use them are still at risk of malaria. Among children who slept under ITNs the night before the survey, almost a third of them tested positive for malaria using Rapid Diagnostic Tests. It should be noted and emphasised that this does not reflect the prevalence of malaria in under-five children in Zambia, but rather, among those who slept under an ITN the previous night using the RDT method in 2021 at the time of the survey. When RDTs are positive, they do not necessarily indicate an active infection as they can remain positive in the convalesce period up to four to six weeks post- treatment[19] . Our study does not imply that the third were positive and had active malaria infections, rather, they had evidence of malaria exposure in the recent past despite using the ITN preventive measures. It may be concerning that such a proportion could still be positive for RDTs despite using this preventive measure. A recent systematic review and meta-analysis which included thirty studies found that the effectiveness of ITNs was RR 0.49 (95%CI 0.32 – 0.74), implying that ITNs are not one hundred per cent protective but rather were able to reduce the risk of infection by about 51% when compared to those who did not use them[20] . Therefore, it is not surprising that we found children who were still positive despite having used ITNs. We, therefore, explored other additional factors associated with malaria infection among children who slept under ITNs.
Some common risk factors associated with malaria infection in Zambia that were explored such assex, rural residence compared to urban residence, education status, wealth index and age were found were found not to be significant in our study[14,21] . Our study may not have found these to be significant because there were minimal random or no additional incremental or detrimental effects of these factors among children who slept under ITNs to either acquire or prevent malaria. To the best of our knowledge, this study is among those pioneering investigating additional factors among under-five children who slept under ITNs. In terms of regions or provinces, the differences were also not statistically significant, due to the pioneering nature of our study, there was limited literature on additional risk factors among children who slept under ITNs. Among studies that compared users against not users of ITNs, the northern regions of Zambia such as Luapula, Northern, Muchinga and North-western provinces have higher risks of malaria infection compared to the southern regions such as Lusaka and Southern provinces[14,22] .
Under-five children who slept under ITNs and whose houses were sprayed with residual chemicals were found to have reduced odds of malaria infection implying there were some synergic effects of IRS, however, when adjusted for other factors in the model, it was not statistically significant. An earlier study found that the synergistic effect of ITNs and IRS was inconclusive and the study did not recommend implementation of both ITNs and IRS[23] . A more recent systematic review found the beneficial effects of combining ITN and IRS interventions but also found mixed and inconclusive results, it did not meta-analyse the findings and thus recommended further research[24] . In agreement with the foregoing, our study is similarly showing insignificant benefits of combining ITNs and IRS. Of particular note is the more than three times increase in odds of malaria among under-five children who slept under ITNs who have anaemia. While our study did not establish causality or directionality of what came before the other between malaria and anaemia, it is known that malaria causes haemolysis which leads to anaemia but also anaemic patients fail to synthesise enough blood cells including immune cells to fight off infections so anaemia may predispose a patient to malaria[24] . A study done in Cote d'Ivoire found that more than three-quarters of the anaemia in children was hypochromic microcytic suggestive of iron deficiency than the normochromic normocytic which is characteristic of haemolytic anaemias[25] . It may therefore be worthy to research more on correcting anaemia through aematic supplementation in under-five children to boost red blood cell production.
CONCLUSION
This study has demonstrated that the prevalence of malaria among children who slept under Insecticide Treated Nets in Zambia using RDT was 28.8% and that anaemia was a significant risk factor among children with malaria. Significant negative findings in this study are that the benefit of adding IRS as a preventive measure against malaria to under-five children who already use ITNs was not statistically significant. Other notable negative findings were that rural and urban differences, provincial locations and wealth quintiles were also not significant risk factors for under-five children who sleep under ITNs.
RECOMMENDATIONS
We recommend further research on the association between malaria and anaemia. While it is known and well-established that malaria causes anaemia, there is a need to establish how anaemia predisposes to malaria infection. Further, we recommend research on haematic supplementation using folic acid and iron in under-five children to see if it can reduce anaemia in high malaria endemic settings like Zambia. While we have no concern with folate supplementation, we have concerns with iron supplementation as it can argument malaria infections among those infected, therefore we do not make policy recommendations yet but recommend molecular studies and randomised clinical trials to see if iron supplementation will be of benefit before any policies recommending iron supplementation in children are made.
LIMITATIONS
The study used secondary data from a cross- sectional study, by the nature of the design, we could not elicit causal effects but association. We also could only use variables that were already collected.
DECLARATIONS
FUNDING
This study was not funded
COMPETING INTERESTS
The authors declare no competing interests
AUTHOR'S CONTRIBUTIONS
NM, PMZ and CS developed the protocol and manuscript. All authors reviewed and approved the manuscript for publication.
REFERENCES
- Okiring, J, P Olwoch, A Kakuru, J Okou, et al. (2019). Household and maternal risk factors for malaria in pregnancy in a highly endemic area of Uganda: a prospective cohort study. Malaria Journal. 18(1): p. 144 https://doi.org/ 10.1186/s12936-019-2779-x
- Brejt, JA and LM Golightly, (2019). Severe malaria: update on pathophysiology and treatment. Current Opinion in Infectious Diseases. 32(5).https://journals.lww.com/co- infectiousdiseases/Fulltext/2019/10000/Severe_malaria update_on_pathophysiology_and.7. aspx
- Conroy, AL, D Datta, and CC John, (2019). What causes severe malaria and its complications in children? Lessons learned over the past 15 years. BMC Medicine. 17(1): p. 52https://doi.org/10.1186/s12916-019-1291-z
- Maduka, O, (2018). End malaria for good: a review of current strategies and future novelties for malaria elimination in Nigeria. Malaria world J. 9: p. 1.https://www.ncbi.nlm. nih.gov/pmc/articles/PMC8415072/
- World Health Organisation. World Malaria Report 2021 [cited 2022 February 21];Available from: h t t p s : / / w w w. w h o . i n t /t e a m s / g l o b a l - m a l a r i a - p r o g r a m m e / r e p o r t s / world-malaria-report-2021
- Yaro, JB, A Ouedraogo, ZA Ouedraogo, A et al., (2020). Acohort study to identify risk factors for Plasmodium falciparum infection in Burkinabe children: implications for other high burden high impact countries. Malaria Journal. 19(1): p. 371https://doi.org/10.1186/s12936-020- 03443-x
- Lubinda, J, Y Bi, U Haque, M Lubinda, B Hamainza, and AJ Moore, (2022). Spatio- temporal monitoring of health facility-level malaria trends in Zambia and adaptive scaling for operational intervention. Communications Medicine. 2(1): p. 79 https://doi.org/10. 1038/s43856-022-00144-1
- Ministry of Health, (2021) Malaria Indicator S u r v e y 2 0 2 1 . h t t p s : / / w w w . n m e c . org.zm/publications
- Monica Anna de, C, S Benoît, R Sol, I, et al., ( 2022 ) . Impact of seasonal malaria chemoprevention on prevalence of malaria infection in malaria indicator surveys in Burkina Faso and Nigeria. BMJ Global Health. 7(5): p. e 0 0 8 0 2 1 h t t p : / / g h . b m j . c o m / c o n t e n t / 7/5/e008021.abstract
- Danny, S, M Nawa, M Lwito Salifya, M Hudson, H Busiku, and S Cephas, (2023). Uptake of four or more doses of sulfadoxine- pyrimethamine for intermittent preventive treatment of malaria during pregnancy in Zambia: findings from the 2018 malaria in pregnancy survey. BMJ Open. 13(5): p. e073287 http://bmjopen.bmj.com/content/13/5/e073287. abstract
- Nawa, M, H Halwindi, and P Hangoma, (2020). Modelling malaria reduction in a highly endemic country: Evidence from household survey, climate, and program data in Zambia. J Public Health Afr. 11(1): p. 1096-1096 https://www.ncbi.nlm.nih.gov/pmc/articles/PM C7649733/
- Kampango, A, M Bragança, Bd Sousa, and JD Charlwood, (2013). Netting barriers to prevent mosquito entry into houses in southern Mozambique: a pilot study. Malaria Journal. 12(1): p. 99 https://doi.org/10.1186/1475-2875- 12-99
- Burns, M, M Rowland, R N'Guessan, et al. (2012). Insecticide-treated plastic sheeting for emergency malaria prevention and shelter among displaced populations: an observational cohort study in a refugee setting in Sierra Leone. Am J Trop Med Hyg. 87(2): p. 242-250 https://www.ncbi.nlm.nih.gov/pmc/articles/PM C3414558/
- Nawa, M, (2019). Influence of History, Geography, and Economics on the Elimination of Malaria: A Perspective on Disease Persistence in Rural Areas of Zambia. International Journal of Travel Medicine and G l o b a l H e a l t h . 7 ( 4 ) : p . 1 1 3 - 1 1 7 http://www.ijtmgh.com/article_99023.html
- Nawa, M, (2020). Investigating the Effect of Prompt Treatment on Malaria Prevalence in Children Aged Below Five Years in Zambia: A Nested Case-control Study in a Cross-Sectional Survey. Advances in Public Health. 2020: p. 4 2 8 9 4 2 0 h t t p s : / / d o i . o r g / 1 0 . 11 5 5 / 2020/4289420
- Nkya, TE, U Fillinger, OP Sangoro, R Marubu, E Chanda, and CM Mutero, (2022). Six decades of malaria vector control in southern Africa: a review of the entomological evidence-base. Malaria Journal. 21(1): p. 279 https://doi.org/ 10.1186/s12936-022-04292-6
- Rugnao, S, S Gonahasa, C Maiteki-Sebuguzi, et al., (2019). LLIN Evaluation in Uganda Project (LLINEUP): factors associated with childhood parasitaemia and anaemia 3 years after a national long-lasting insecticidal net distribution campaign: a cross-sectional survey. M a l a r i a J o u r n a l . 1 8 ( 1 ) : p . 207https://doi.org/10.1186/s12936-019-2838-3
- Yang, G-g, D Kim, A Pham, and CJ Paul (2018). A Meta- Regression Analysis of the Effectiveness of Mosquito Nets for Malaria Control: The Value of Long-Lasting Insecticide Nets. International Journal of Environmental Research and Public Health, 2018. 15, DOI: 10.3390/ijerph15030546.https://www.mdpi.co m/1660-4601/15/3/546
- Mbabazi, P, H Hopkins, E Osilo, M Kalungu, P Byakika-Kibwika, and MR Kamya, (2015). Accuracy of two malaria rapid diagnostic tests (RDTS) for initial diagnosis and treatment monitoring in a high transmission setting in Uganda. Am J Trop Med Hyg. 92(3): p. 530-6 D O I : 1 0 . 4 2 6 9 / a j t m h . 1 4 - 0180.https://www.ncbi.nlm.nih.gov/pmc/articl es/PMC4350543/
- Wangdi, K, L Furuya-Kanamori, J Clark, et al. (2018). Comparative effectiveness of malaria prevention measures: a systematic review and network meta-analysis. Parasites & Vectors. 11(1): p. 210https://doi.org/10.1186/s13071- 018-2783-y
- Degarege, A, K Fennie, D Degarege, S Chennupati, and P Madhivanan, (2019). Improving socioeconomic status may reduce the burden of malaria in sub-Saharan Africa: A systematic review and meta-analysis. PLOS O N E . 1 4 ( 1 ) : p . e 0 2 1 1 2 0 5 D O I : 10.1371/journal.pone.0211205.https://doi.org/ 10.1371/journal.pone.0211205
- Kyomuhangi, I, A Andrada, Z Mao, et al. (2023). Assessing national vector control micro- planning in Zambia using the 2021 malaria indicator survey. Malaria Journal. 22(1): p. 365 https://doi.org/10.1186/s12936-023-04807-9
- Okumu, FO, (2012). Combining insecticide- treated bed nets and indoor residual spraying for malaria vector control in Africa. Malaria Journal 10 ( 1 ) : 208 https:// doi. org/ 10.1186/1475-2875-10-208
- Musoke, D, E Atusingwize, C Namata, R Ndejjo, RK Wanyenze, and MR Kamya, (2023). Integrated malaria prevention in low- and middle-income countries: a systematic review. M a l a r i a J o u r n a l . 2 2 ( 1 ) : p . 7 9 https://doi.org/10.1186/s12936-023- 04500-x
- Acheampong, CO, MA Barffour, KJ Schulze, et al. (2021). Age-specific differences in the magnitude of malaria-related anaemia during low and high malaria seasons in rural Zambian c h i l d r e n . E J H a e m . 2 ( 3 ) : p . 3 4 9 - 356.https://doi.org/10.1002/jha2.243
- Ehouman, MA, KE N'Goran, and G Coulibaly, (2022). Malaria and anaemia in children under 7 years of age in the western region of Côte d'Ivoire. Frontiers in Tropical Diseases. 3.https://www.frontiersin.org/articles/10.3389/ fitd.2022.957166
Medical Journal of Zambia, Vol 50, 4
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.