Insights from the Field: A phenomenological study of Radiography students' computed tomography clinical placement experiences
Bornface Chinene
Harare Institute of Technology, Department of Radiography, Belvedere, Harare, Zimbabwe
P. O. Box BE 277, Belvedere, Harare, Zimbabwe.
Email: bchinene@hit.ac.zw; bornfacechinene@gmail.com
Phone: +263773270576
DOI: https://doi.org/10.55320/mjz.50.4.438
Keywords:Experiences, Radiography students, Computed Tomography, Clinical placement, Low-resource setting
ABSTRACT
Background:While there are studies that explore the overall experiences of radiography students during clinical placements, there is a lack of research specifically focusing on the experiences of students in the context of computed tomography (CT). Therefore, this study aimed to understand the experiences of radiography students during their clinical placements in CT imaging at a tertiary institution in Harare, Zimbabwe.
Methods:A qualitative descriptive phenomenological study design employing one-on- one interviews with 15 undergraduate students was conducted. The interview data was managed in Nvivo 12, and the inductive analysis was based on Giorgi's structured way of analysing phenomenological data.
Results: The findings show that student's experience during CT clinical placements was diverse and distinct compared to their other placements. Four themes emerged from the interview data that summarised their experiences i. Nervousness ii. Limited CT clinical exposure iii. Theory to Practice Conversion, and iv. Interpersonal skills. Initially, they felt nervous, but later they found the placements to be interesting and challenging. Some students were able to apply their theoretical knowledge to practical situations. Students also had an opportunity to improve their interpersonal skills. However, students also faced challenges such as equipment breakdowns and a shortage of consumables. These affected the student's ability to acquire the necessary clinical skills within the given time frame.
Conclusion: Given the limitations in accessing CT practical experience, innovative strategies such as software simulation-based training, particularly virtual reality CT simulation, are suggested to enhance students' preparedness.
INTRODUCTION
Computed tomography is an increasingly important imaging modality that has revolutionized diagnostic imaging.[1] With its advantages over conventional radiography, the use of CT has significantly increased in the past two decades.[2-4] Computed tomography allows for the elimination of superimposed anatomical structures and scatter, resulting in superior image quality.[5] As a result, it has become an integral part of the radiography curriculum in universities and colleges worldwide, providing students with the necessary knowledge and skills to utilize this advanced imaging technology.
The incorporation of CT into radiography education aims to equip students with the theoretical knowledge and clinical competencies required to safely and efficiently use CT in their clinical practice.[6] Clinical placements play a vital role in bridging the gap between theory and practice, allowing students to observe experienced professionals (preceptors) and gain practical experience.[7] However, clinical placements also present various challenges for students,[8] and while several studies have examined the experiences of radiography students during clinical placements,[9-12] there is a limited focus on CT-specific experiences.
In Zimbabwe, CT clinical sites face increasing resource pressure while accommodating growing student numbers. Computed tomography is considered a specialized field in medical imaging,[1] and requires operator-dependent adjustments for each examination and patient.[5] Additionally, due to the high radiation dose associated with CT, proper training is crucial to optimize examinations and ensure patient safety.[1] The Allied Health Practitioners Council of Zimbabwe (AHPCZ) mandates that radiographers perform CT examinations per departmental, national, and global CT standards.[13] Radiography training institutions meet this requirement by integrating CT theoretical knowledge and clinical placements into their curriculum. However, as state universities often lack their own hospitals or CT scanners,[14] students are placed in public and private radiology centres across the country, potentially influencing their clinical placement experiences.
This study aimed to understand the descriptions and meanings of CT clinical experiences among radiography students from a tertiary institution in Harare, Zimbabwe. By shedding light on the day-to- day activities of students during clinical placements, this research sought to identify gaps and deficiencies in CT clinical training. Furthermore, it aims to provide insights to CT radiographers and educators, enabling them to understand the student experience and introduce improvements for a more enriching learning environment.
METHODS
Research design
This study utilized a qualitative descriptive phenomenological study design to understand the universal experience of students during CT clinical placements.[15] Phenomenology is based on the philosophical tradition developed by Edmund Husserl in the early 20th century.[16] Husserl emphasized that the focus of a study should be the phenomenon perceived by an individual's consciousness and that consciousness is central to all human experience.[17] Therefore, the goal of descriptive phenomenology is to describe the universal essence of an experience as lived, which represents the true nature of the phenomena.[18] The consolidated criteria for reporting qualitative research (COREQ) were adhered to in this study.[19]
Setting
The institution is located in Zimbabwe's capital Harare. It is one of the two-state Institutions that offer a 4-year bachelor's degree in radiography. The CT module is done in the third year. To provide practical experience, the institution depends on three public hospitals to accommodate their students for clinical placements. However, an audit conducted on radiology equipment in Zimbabwe revealed that nearly 64% (14 out of 22) of CT units are privately owned.[20] Furthermore, equipment downtime and a shortage of consumables in the public sector reduce availability.[21,22] Consequently, tertiary institutions have to rely on private centres to place their students. However, private centres may be hesitant to allow students to operate their CT scanners even under supervision due to the high costs associated with purchasing, repairing, and maintaining the equipment.
Population and sampling
The institution has a yearly enrolment of approximately 25 students both for therapy and diagnostic. The total population is 104 students. Since the CT course is done in the 3rd year, the inclusion criteria were;
•Third and fourth-year students •Diagnostic Radiography major.
The students were purposively sampled until data saturation.
Data Collection and Analysis
The interview guide was developed, and then two lecturers from the School of Radiography reviewed the questions and suggested improvements. Following this, three pilot interviews were conducted with radiography students from another university to assess question clarity and estimate the expected duration of each interview. To minimize power dynamics between the researcher and the participants, a colleague from another health department (Who has a Ph.D. in Clinical Psychology), experienced in qualitative research, was asked to conduct face-to-face interviews with participants, each lasting approximately 20 minutes. The leading interview question was, “What were your experiences during CT clinical placements? The probing questions were adjusted to follow the flow of the discussion. The interviews were audio- recorded using the Voice Recorder (Version 3.25) Android application and transcribed verbatim. The interview data was managed in NVivo 12 [23] and inductive analysis was based on Giorgi's structured way of analysing phenomenological data.17The following are the five main stages that were followed in a step-by-step manner:
i. First, it was important to put aside any preconceived ideas before starting the analysis of the data. ii. Next, the interview transcripts were carefully reviewed to gain a thorough understanding of the information provided by the participants. iii. The transcripts were then grouped into units, which involved organizing relevant pieces of information into manageable chunks. iv. Based on these grouped units, themes were created to capture the key patterns and trends emerging from the data. v. Finally, keeping the phenomenon of study, the purpose of the research, and the research questions in mind, descriptive explanations of the themes were presented.
Trustworthiness and integrity of the study
This study employed Lincoln and Guba's,[24] criteria for establishing trustworthiness in qualitative research, which includes credibility, dependability, confirmability, and transferability. To enhance credibility, the transcribed interviews were shared with the participants for their input (Member checking).[15] Their feedback was used to improve the authenticity and accuracy of the data. To ensure confirmability, the results section included verbatim quotes from the participants. In addition, the researcher employed a process called "reflective meditation" to bracket his perspectives, preconceptions, and expectations about clinical placements, and to consider how these might influence his interpretation of interview transcripts. The researcher then recorded this self-reflection in a journal.
Ethical considerations
The study was carried out according to the Declaration of Helsinki.[26] Ethical approval for this studywas obtained from the University School of Allied Health Ethics Committee (SAHS/DR00027/23). To participate in the study, all respondents provided written informed consent, ensuring their voluntary involvement. To protect the privacy and confidentiality of the participants, their identities were kept confidential. Participants were informed that they had the option to withdraw from the study at any time if they wished to do so.
RESULTS
Demographics
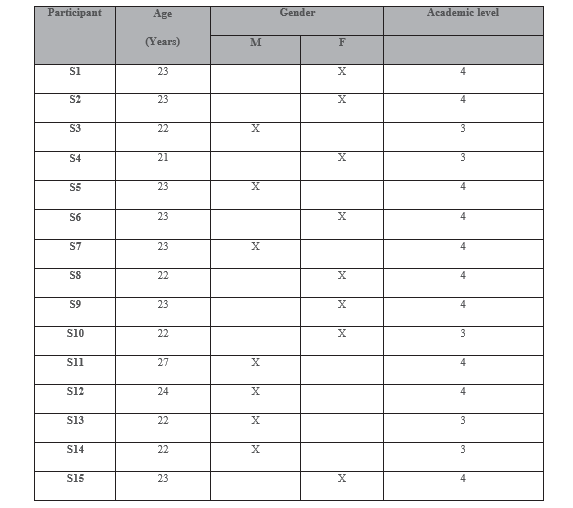
A total of 15 students took part in the study. Their demographic characteristics are summarised in Table 1.
Experiences of students during CT clinical placements.
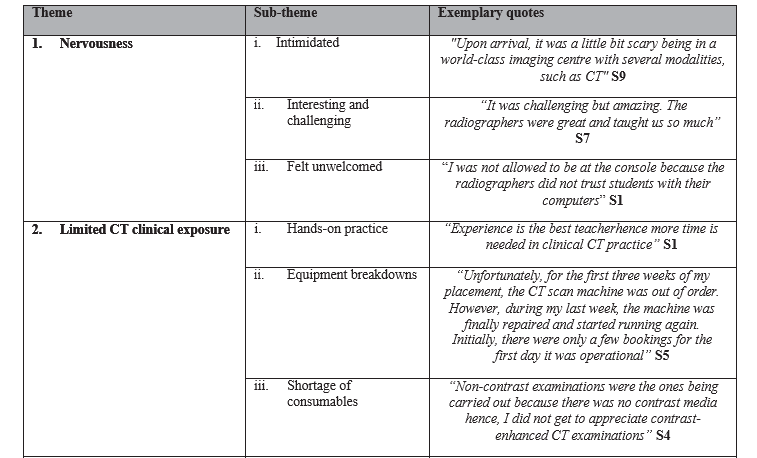
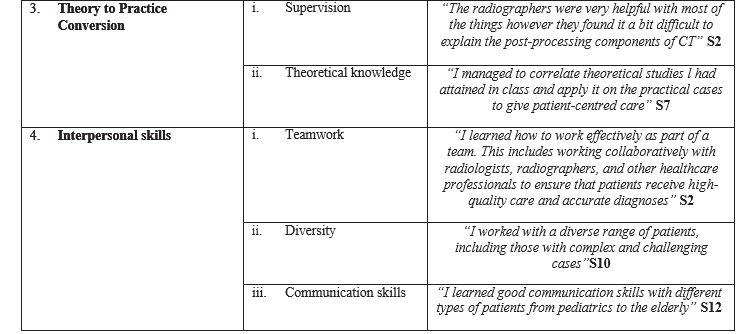
Through conducting interviews with students, four main themes and eleven subthemes emerged based on the data collected. Table 2 gives an overview of these findings.
Theme 1: Nervousness
This theme explores the experiences of students, especially during their first-time attending CT placements. Three subthemes emerged including: being intimidated, finding it interesting and challenging, and feeling unwelcomed.
i. Intimidated
During their course, students primarily focus on general radiography and only transition to more advanced modalities like CT towards the end of the course. As a result, many students reported feeling intimidated by this shift.
"XXX Hospital is known for having patients of different races, and as a result, they hold their patient care to high standards. Initially, we were not allowed to call patients from the reception desk or handle them during examinations."S6
"Upon arrival, it was a little bit scary being in a world-class imaging centre with several modalities, such as CT" S9
ii. Interesting and challenging
However, once the participants adjusted to the transition from general radiography to CT, they discovered that their placements were both interesting and challenging.
“It was challenging but amazing. The radiographers were great and taught us so much”S7
“...my experience was both rewarding and challenging, and I believe that it has prepared me well for future opportunities in the field of radiography”S11
This was particularly true because they had mostly been working in general radiography, so the opportunity to break away from the monotony was refreshing.
“CT removed the monotonous action like preprogrammed sequence that came with general radiography when you only needed to carry out projections for different examinations thus a common name coined button pusher was created”S13
iii. Felt unwelcomed
However, some students felt unwelcome in certain departments where they were placed because they were not permitted to touch anything, as evidenced by the following quotes:
“I was not allowed to be at the console because the radiographers did not trust students with their computers” S1
“I also had an experience with CT at a private center. As a student, I was only allowed to do room preparation and preparing cannula trays” S2
Theme 2: Lack of adequate time
This theme highlights the challenges faced by students with exposure to the CT modality during their clinical placements. Within this theme, four specific subthemes have emerged, all of which highlight the issues that have led to shortened placement times. These subthemes include the lack of hands-on practice, equipment breakdowns, insufficient time, and a shortage of necessary supplies.
i. Hands-on practice
Participants shared that during their time in the CT clinical departments, they were limited to being mere observers and were not allowed to have any hands-on experience. In addition, some radiographers were neglectful in explaining procedures or providing guidance to the students.
“Experience is the best teacher; hence more time is needed in clinical CT practice” S1
“I would just observe what was going on and the radiographers did not bother to explain what was going on even though I had never been attached to a department with a CT machine” S3
“The downside to this attachment was the fact we were just observing. I think we would have appreciated CT more if we were allowed to position patients or at least move the table into the gantry”S13
However, certain departments experienced a low influx of patients, resulting in students not receiving sufficient clinical exposure.
“I went to a government hospital that had only 3 CT patients booked per day. No contrast examinations were being done, so there was not much exposure” S2
Furthermore, due to the limited number of examinations that could be conducted, students had a restricted opportunity to gain exposure to other types of examinations.
“On average, an estimated 10 patients came for CT examinations per day with the most common examinations being CT brain, CT sinuses, aS6nd CT chest, abdomen, and pelvis. As a result, we became more familiar with these exams”
“Most examinations that we carried out during my placement were CT brain and sinuses hence I did not get to observe CT scans of other regions” S4
ii. Equipment breakdowns
Students also pointed out that their clinical exposure was shortened due to equipment breakdowns in some of the departments they were assigned to.
“…in my case when I arrived at the center, the CT scanner and fluoroscopy machines were down which then left me with only 2 modalities to learn from – Ultrasound and general x-rays”S3
“Unfortunately, for the first three weeks of my placement, the CT scan machine was out of order. However, during my last week, the machine was finally repaired and started running again. Initially, there were only a few bookings for the first day it was operational."S5
iii. Shortage of consumables
Participants also highlighted that the shortage of consumables also contributed to their hands-on practice in some departments.
“Non-contrast examinations were the ones being carried out because there was no contrast media hence, I did not get to appreciate contrast- enhanced CT examinations” S4
“During my placement there, films were not available hence images were put on a disk hence I did not get to learn how the images are printed on a film” S5
Theme 3: Theory to Practice Conversion
This theme focuses on the differences or similarities between what the students learned in class and what they observed in the clinical setting. It consists of two subthemes: Supervision and theoretical knowledge
i. Supervision
According to some students, although some of the radiographers were willing to assist them, they lacked effective teaching skills.
“The radiographers were very helpful with most of the things however they found it a bit difficult to explain the post-processing components of CT” S2
In addition, some radiographers showed no interest in teaching the students at all.
“The radiographers were only there to demonstrate on one patient then leave us alone”S14
ii. Theoretical knowledge
The students found the clinical placements to be helpful because they were able to connect what they had learned in class with what they observed in the clinical setting.
“I managed to correlate theoretical studies l had attained in class and apply it on the practical cases to give patient-centred care” S7
“CT brain scans were occasionally done which led to me personally appreciating the stuff we had learned in class. I could pinpoint an epidural hematoma or an infarct when it presented” S13
However, some students have noticed a difference between what they learn in the classroom and what they experience in the real-world clinical setting
“In class, we had done pathologies of the head CT so generally I had little knowledge of how abdominal pathologies present on a CT scan” S13
“For the rest of my attachment, bookings were full and examinations were supposed to be completed during the allocated time hence I did not get to learn how the reconstruction of images was done” S4
Theme 4: Interpersonal skills
This theme emphasizes the interpersonal skills that the students acquired through their CT clinical placements. Three subthemes were identified, including teamwork, diversity, and communication skills.
i. Teamwork
The students expressed that the CT clinical placements helped them recognize the significance of teamwork because they had a chance to collaborate with other healthcare professionals.
“I learned how to work effectively as part of a team. This includes working collaboratively with radiologists, radiographers, and other healthcare professionals to ensure that patients receive high- quality care and accurate diagnoses” S2
“I also worked closely with physicians and other healthcare professionals to interpret and analyse imaging results, and to develop treatment plans for patients. This made me realise that in the hospital it is vital to work as a team. In addition to my technical responsibilities, I played a vital role in patient care and communication” S10
More importantly, they had an opportunity to interact with radiologists;
“Moreover, we got to work with the radiologist when reporting general x-rays and got the chance to learn about the reporting process” S12
ii. Diversity
Furthermore, the students had the opportunity to work in a setting where they engaged with a diverse population of patients.
“I worked with a diverse range of patients, including those with complex and challenging cases” S10
iii. Communication skills
As a result of their interactions with diverse healthcare teams and patients, some students felt that their communication skills were greatly improved.
“While in CT, I got the chance to work with different radiographers who had also different strengths and preferences which in turn improved my CT as well as communication skills” S9
“I learned good communication skills with different types of patients from pediatrics to the elderly”S12
“I was also able to gain experience in the communication and interpersonal skills required for working in a clinical environment. This included the ability to interact with patients professionally and compassionately, as well as the ability to work effectively as part of a team”S11
DISCUSSION
Clinical experiences for radiography students take place in diverse social contexts, each with its organizational structure and impact.[8] Additionally, various factors, including student preparedness, faculty and clinical staff characteristics, peer support, clinical opportunities, and student participation, can influence students' perceptions of the clinical environment.[27] This study aimed to understand the experiences of radiography students during their clinical placements in CT imaging. To the best of the authors' knowledge, this study is the first to explore undergraduate students' experiences in CT clinical placements from a phenomenological perspective in Zimbabwe. The study emphasizes the importance for CT radiographers and educators to understand the student's perspective during their supervision, as this understanding can drive the implementation of improvements to enhance the overall student experience. However, future studies should involve students from multiple institutions to determine whether the findings of the current study are consistent across different student populations.
The students in the current study reported challenges that included CT equipment breakdowns and a shortage of consumables. These factors may have affected the student's ability to gain the necessary clinical competencies within the allotted time. Comparable studies conducted in similar settings have yielded similar findings. For instance, a study in Ghana revealed that a lack of equipment resulted in insufficient exposure to specialized procedures and limited time in treatment rooms.[28] Similarly, in an Ethiopian study, participants noted variations in resource availability and suitability across placement centres, with some considered well-equipped and suitable for teaching and learning, while others were deemed unsuitable.[29] Insufficient clinical practice in CT can significantly impact the delivery of quality healthcare once students graduate.
Universities especially in low-resource settings like Zimbabwe encounter several challenges when it comes to conducting clinical placements for high- end modalities like CT. One major hurdle is the high cost associated with having an onsite CT scanner. As a result, they must turn to either public hospitals or private radiology departments to allow students to gain practical experience. However, public facilities in Zimbabwe also face difficulties in maintaining the equipment, as highlighted by previous studies.[21,22, 30] On the other hand, private centres tend to have better equipment maintenance. However, they may have limitations on the number of students they can accommodate and may impose restrictions on the hands-on experience students can gain. In the current study, students reported that they were mostly allowed to observe and were not permitted to interact with the CT equipment. Additionally, the COVID-19 pandemic has worsened the situation by reducing clinical placements for students.[14] As a result, students may not receive sufficient exposure to practical CT experience, leading to potential unpreparedness for their future practice. Therefore, there is a pressing need for innovative strategies in CT education to ensure that this essential skill is adequately taught and learned in Zimbabwe and other similar settings.
One strategy that is trending is software simulation- based training.[31] Simulation software offers a secure and effective platform for students at any level to practice and acquire the necessary clinical skills to enhance the quality of healthcare services.[32] By utilizing simulation for CT techniques, students can better prepare themselves and gain a deeper understanding of technical challenges and complex situations. One type of simulation software that has been used is Virtual Reality CT.[33] Incorporating virtual reality CT simulation strategies into a comprehensive learning package has the potential to enhance students' preparedness for their clinical learning experiences,[32,34] in low-resource settings. However, there are potential challenges in low-resource settings when it comes to implementing virtual reality training in CT. These challenges include inadequate policies, a shortage of technical expertise, and support to set up and sustain the systems.[35,36] Moreover, ensuring that virtual reality simulations are culturally relevant and suitable for African learners can also be a hurdle.[37] Therefore, it is crucial to conduct further research to examine these issues and determine an effective system that can enhance the clinical learning of student radiographers.
Practical recommendations for establishing a CT simulation training unit in Zimbabwe and similar settings include the following:
i. Establish a platform and infrastructure for the development of a CT simulation unit. Seek financial support from government, university, commercial companies, suppliers, private and public hospitals, and private donations. ii. Identify academic staff and technical support staff to man the simulation unit. iii. Register with the Allied Health Practitioners Council of Zimbabwe (AHPCZ) and other relevant international regulatory bodies. iv. Integrate CT simulation seamlessly into the radiography curriculum, considering the safety and ethical aspects of student training. v. Assess the reliability of the tools. vi. Continuously improve as necessary.
Limitations of the study
The study's limitation is that it only included students from one university, which may restrict the applicability of the findings to other institutions. Nevertheless, the findings may be relevant to other institutions and low-resource settings. Furthermore, even though the sample size obtained is relatively small, we made sure to achieve saturation during the interviews to enhance the quality of the data.
CONCLUSION
The findings show that students' experience during CT clinical placements was diverse and distinct compared to their other placements. Initially, they felt nervous, but later they found the placements to be interesting and challenging. Some students were able to apply their theoretical knowledge to practical situations. Students also had an opportunity to improve their interpersonal skills. However, students also faced challenges such as equipment breakdowns and a shortage of consumables. These affected the student's ability to acquire the necessary clinical skills within the given time frame.
Therefore, this study highlights the impact of equipment breakdowns and shortages on students' clinical competencies and emphasizes the potential long-term effects on healthcare delivery. Given the limitations in accessing practical experience, innovative strategies such as software simulation- based training, particularly virtual reality CT simulation, are suggested to enhance students' preparedness. However, challenges in implementing such strategies in low-resource settings are acknowledged, indicating the need for further research to address these issues and develop effective systems for enhancing the clinical learning of student radiographers.
DECLARATIONS
Acknowledgments
I would like to express my gratitude to all the students who willingly participated in the study. Your willingness to contribute has been invaluable to the research process. Additionally, I would like to extend my thanks to all the lecturers who generously agreed to review the themes and subthemes. Your expertise and insights have greatly enriched the study
Conflict of Interest
N/A
Funding sources.
N/A
REFERENCES
- Carver E, Carver B. Medical imaging: Techniques, Reflection and Evaluation. Second. Edinburgh: Churchill Livingstone; 2012. 417–437.
- Westmark S, Hessellund T, Hoffmann A, Madsen BB, Jensen TS, Gielen M, et al. Increasing use of computed tomography scans in the North Denmark Region raises patient s a f e t y c o n c e r n . E u r J R a d i o l . 2023;1;166:110997.
- Frija G, Damilakis J, Paulo G, Loose R, Vano E. Cumulative effective dose from recurrent CT examinations in Europe: proposal for clinical guidance based on an ESR EuroSafe I m a g i n g s u r v e y . E u r R a d i o l . 2021;31(8):5514–23. Available from: https://link.springer.com/article/10.1007/s003 30-021-07696-1
- Number of CT examinations in selected countries 2019. Statista. [cited 2024 Jan 25]. Available from: https://www.statista.com/ statistics/283085/computer-tomography- examinations-in-selected-countries/
- Romans L. Computed Tomography for Technologists. 1st ed. Baltimore, Maryland: Wolters Kluwer Health. Lippincott Williams & Wilkins; 2011. 1–402.
- Lee K, Baird M, Lewis S, Mcinerney J, Dimmock M. Radiography Computed tomography learning via high- fi delity simulation for undergraduate radiography students. Radiography. 2020;26(1):49–56. Available from: https://doi.org/10.1016/ j.radi.2019.07.001
- Mifsud C., Castillo J, Portelli J. Radiography students ' clinical placement experiences in M R I ?: A p h e n o m e n o l o g i c a l s t u d y. Radiography. 2015;21(1):e17-20.
- Chamunyonga C, Singh A, Mit-radiography D, Imaging M, Ed M, Gunn T, et al. Strategies to develop student support mechanisms in medical radiation sciences clinical education. J Med Imaging Radiat Sci. 2020;51(4):512–7. Available from: https://doi.org/10.1016/ j.jmir.2020.08.004
- Portanier Mifsud C, Castillo J, Portelli JL. Radiography students' clinical placement experiences in MRI: A phenomenological study. Radiography. 2015;21(1):e17–20. Available from: https://linkinghub.elsevier. com/retrieve/pii/S1078817414000960
- Chinene B, Sanyamandwe C, Hlahla T. Challenges experienced by radiography students during clinical placements in a low r e s o u r c e s e t t i n g : A q u a l i t a t i v e phenomenological study. South African Radiogr. 2023;61(2):32–40.
- Ondari BO, Rajeswaran L, Ekemiri KK, Xavier SF, Jean N. Experiences of Medical Imaging Students and Clinical Learning in a Limited Resource Setting - A Qualitative Study in Rwanda. J Glob Radiol. 2019;5(1):1–7.
- Bwanga O, Lidster J. Radiography Students ' Perceptions and Experiences of their Clinical Placements?: A Qualitative Systematic Review. East African Sch J Med Sci. 2019;2(7):367–80.
- Allied Health Practitioners Council of Zimbabwe. Professional registration. 2023. Available from: https:// www. google. com/search?gs_ssp=eJwFwUEKgCAQAEC6 Br2gi5fOuq2S-oQ-EWqaglSokM9vZpzoRQ FCBQnwHWzQC-ugEKzlYlMuyLCiZh 2FAB64dKgMSmH32eSc_EmiN7lF8hbjWm rpuX2pP7dEGR0&q=allied+health+practitio ners&oq=allied+health&aqs=chrome.1.0i355i 512j46i175i199i512j69i57j0i5
- Taylor B, McLean G, Sim J. Immersive virtual reality for pre-registration computed tomography education of radiographers: A narrative review. J Med Radiat Sci. 2023;70(2):171–82.
- Adu P. A Step- by- Step Guide to Qualitative Data Coding. New York: Routledge; 2019.
- Giorgi AP, Giorgi BM. The descriptive phenomenological psychological method. In: Qualitative research in psychology: Expanding perspectives in methodology and design. Washington DC: American Psychological Association; 2003. p. 243–72.
- Giorgi A. An application of phenomenological method in psychology. In: Giorgi, A, Fischer, WF, von Eckartsberg, R, eds Duquesne Studies in Phenomenological Psychology. Pittsburg: Duquesne University Press; 1975. p. 1–59. Av a i l a b l e f r o m : h t t p s : / / d o i . o r g / 10.5840/dspp197529
- Shorey S, Ng ED. Examining characteristics of descriptive phenomenological nursing studies: A s c o p i n g r e v i e w. J A d v N u r s . 2022;78(7):1968–79.
- Tong A, Flemming K, McInnes E, Oliver S, Craig J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med Res Methodol. 2012;12(181):1–8.
- Chinene B, Mutasa E, Bwanga O. Computed Tomography (CT) Imaging Services in Zimbabwe?: A Mini-review Study. Int J Med Rev. 2023;10(3):543–52.
- Chinene B, Mudadi L, Mutandiro L, Mushosho EY, Matika W. Radiographers ' views on the workplace factors that impact their mental health?: Findings of a survey at central hospitals in Zimbabwe. J Med Imaging Radiat Sci. 2023;54(2, Supplement):S52-61. Available f r o m : h t t p s : / / d o i . o r g / 1 0 . 1 0 1 6 / j.jmir.2023.02.013
- Hinrichs-Krapels S, Tombo L, Boulding H, Majonga ED, Cummins C, Manaseki-Holland S. Barriers and facilitators for the provision of radiology services in Zimbabwe: A qualitative study based on staff experiences and observations. PLOS Glob Public Heal. 2023;3(4):e0001796. Available from: http://dx.doi.org/10.1371/journal.pgph.00017 96
- Nvivo. Qualitative data analysis software; QSR International Pty Ltd. Version 12. 2018.
- Lincoln YS, Guba EG. Naturalistic Inquiry. Sage Publications. Newbury Park, CA; 1985.
- Moustakas C. Phenomenological research methods. New York: SAGE Publications, Inc.; 1994.
- WMA. WMA Declaration of Helsinki – Ethical Principles for Medical Research Involving Human Subjects. The World Medical Association, Inc. 2018 [cited 2020 Apr 1]. Available from: https://www.wma.net/ policies-post/wma-declaration-of-helsinki- ethical-principles-for-medical-research- involving-human-subjects/
- Fortsch P, Henning JE, Nielsen LE. Connecting classroom to clinical practice: a comparison of programs. Radiol Technol. 2009;81(2):112–21.
- Kyei KA, Antwi WK, Offei RO. Challenges Faced by Radiography Students During C l i n i c a l Tr a i n i n g . Clin Med Res. 2015;4(3–1):36–41.
- Kumsa MJ, Lemu BN, Nguse TM, Omiyi DO, Akudjedu TN. Radiography Clinical placement challenges associated with radiography education in a low-resource setting?: A qualitative exploration of the Ethiopian l andscape. Radiography. 2022 ; 28 ( 3 ) : 634 – 40 . Available from: https://doi.org/10.1016/j.radi.2022.04.014
- Maboreke T, Banhwa J, Pitcher R. An audit of licenced Zimbabwean radiology equipment as a measure of health access and equiry. Pan Afr Med J. 2019;36(60):1–11.
- Partner A, Shiner N, Hyde E, Errett S. First year student radiographers' perceptions of a one- week simulation-based education package designed to increase clinical placement capacity. Radiography. 2022;28(3):577–85. Av a i l a b l e f r o m : h t t p s : / / d o i . o r g / 10.1016/j.radi.2022.04.007
- Nguyen TT, Hoang NT, Le VC, Nguyen T Van, Ha TH. Simulation-Based Training for Radiography Students as a Solution in Covid- 19 Pandemic?: Student ' s Perspective from a Developing Country Running Title?: SBT for Radiography Students in Vietnam. Univers J Public Heal. 2022;10(4):385–92.
- Gunn T, Rowntree P, Starkey D, Nissen L. The use of virtual reality computed tomography simulation within a medical imaging and a radiation therapy undergraduate programme. J Med Radiat Sci. 2021;68(1):28–36.
- Kim S, Bochatay N, Relyea-Chew A, Buttrick E, Amdahl C, Kim L, et al. Individual, interpersonal, and organisational factors of healthcare conflict: A scoping review. J Interprof Care. 2017;31(3):282–90. Available f rom: https:// www. t andfonline. com/ doi/full/10.1080/13561820.2016.1272558
- UNESCO. Evaluation of Virtual Reality in Africa: An educational perspective. Paris; 2004.
- Harrington J. The Potential of Using Virtual Reality in Education in Nigeria. The Borgen Project. 2022.
- Mkwizu KH. Virtual Reality and Open Schooling: Challenges and Opportunities. NiosAc.in. 2022;1(1). Available from: https://www.nios.ac.in/media/documents/IJO S/articles/IJOS_Ch-19.pdf
Medical Journal of Zambia, Vol 50, 4
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.