Metastatic gastric cancer in a 23- year-old Zambian female diagnosed posthumously: A case report
Sydney Mpisa
University of Zambia School of Medicine, Department of Internal Medicine, Nationalist Road, PO Box 50110, Lusaka, Zambia
Tropical Gastroenterology and Nutrition Group, 26 Esther Lungu Road, Kamwala South, Lusaka, Zambia
Cordelia Himwaze
University Teaching Hospital, Department of Pathology and Microbiology, Nationalist Road, Private Bag RW IX, Lusaka, Zambia
Vutisa Dokowe
University Teaching Hospital, Department of Pathology and Microbiology, Nationalist Road, Private Bag RW IX, Lusaka, Zambia
Violet Kayamba
University of Zambia School of Medicine, Department of Internal Medicine, Nationalist Road, PO Box 50110, Lusaka, Zambia
Tropical Gastroenterology and Nutrition Group, 26 Esther Lungu Road, Kamwala South, Lusaka, Zambia
DOI: https://doi.org/10.55320/mjz.50.4.429
Keywords:Gastric cancer, adenocarcinoma, Zambia, case report
ABSTRACT
Background: Gastric cancer is one of the leading causes of cancer mortality globally and in Zambia, its exact burden is unknown. Here, we present a case of gastric cancer in a young adult that was diagnosed posthumously.
Clinical presentation: A 23-year-old female patient was referred to the largest tertiary care institution in Zambia, the University Teaching Hospital (UTH). She had been followed up at a district hospital. The patient had a three months' history of ill-health with symptoms of anaemia, abdominal pain and distension. During the period of ill-health, she had been managed symptomatically with abdominal pain being the main complaint. A week prior the patient had been admitted for symptomatic anaemia requiring two units of blood transfusion. The patient had no menorrhagia or hematemesis but admitted to episodes of dark coloured stools. Upon arrival at UTH, she was noted to be very frail, with pallor, tachycardia and gross abdominal distension and a nodular irregular liver, measuring 10cm below the costal margin. A digital rectal examination revealed the presence of melena. She had no jaundice, lymphadenopathy or finger clubbing but had bilateral pedal oedema. A provisional diagnosis of non-cirrhotichepatocellular carcinoma complicated by upper gastrointestinal bleeding was made.
Key findings: Investigations revealed normal alpha fetoprotein, a Transient Elastography value of75kPa and negative hepatitis B and C serology. Computerised tomography scan showed multiple liver masses with ascites. The patient continued to deteriorate despite supportive management and died on day 10 of admission. A post mortem was done which revealed a primary gastric adenocarcinoma with metastasis to the liver, lungs and pancreas.
Conclusion: This is an example of a case of gastric cancer that was not detected while the patient was alive. The age of the patient and the symptoms that are not specific to gastric cancer could have contributed to the delayed diagnosis. It illustrates how cases of gastric cancer would be missed by the Zambia National Cancer Registry recording system.
INTRODUCTION
Gastric cancer is a disease of global importance with over one million estimated new cases annually1. It is the third most common cause of cancer related deaths with over 784,000 deaths globally in 2020[1] . In Zambia, gastric cancer is ranked tenth among the common cancers seen country-wide, but it is the third most commonly diagnosed cancer at the University Teaching Hospital(UTH) gastrointestinal unit[2] . Most patients present with advanced disease that is not amenable to surgery and these usually have poor outcomes as was the case with our patient. The most predominant type of gastric cancer is adenocarcinoma. In literature, gastric adenocarcinoma is generally referred to as gastric cancer, leaving specific nomenclature to other sub-types[3] . Gastric adenocarcinoma will therefore be referred to as gastric cancer in this case report.
The development of gastric cancer is multi factorial influenced by environmental and genetic factors[4] . It is believed that gastric cancer may occur even after 20-30 years following exposure to carcinogenic agents. It is due to this heterogeneous nature and aggressiveness that it remains a global health problem. There are several ways of classifying gastric cancer. Histologically, the Lauren classification is widely used. It divides gastric cancer into diffuse, intestinal type and mixed type each with distinct epidemiological, morphological and molecular features[5] .Other ways of classifying gastric cancer include the World Health Organisation and The Cancer Genome Atlas classifications.
The risk factors for development of gastric cancer are diverse and include, among others cigarette smoking, excessive alcohol consumption, diet rich in salted and smoked food, genetic factors and Helicobacter pylori infection[6] . We previously reported that about a quarter of gastric cancer patients in Zambia were below the age of 45 years[7,8] . This is considered to be early on set gastric cancer. We found that 64% of early onset gastric cancer in Zambia were of the intestinal sub-type[8,9] . Intestinal type of gastric cancer is predominantly triggered by environmental factors. The proportion of early onset gastric cancer that we reported was significantly higher than that reported elsewhere and therefore, there is a need to investigate gastric carcinogenesis in the Zambian setting. In addition, a previous audit of records at the Zambia National Cancer Registry revealed that 42% of patients with histologically confirmed gastric cancer at the University Teaching Hospital (UTH) were not included in the registry data[10] .
This case report is an example of undetected early onset gastric cancer whose diagnosis of gastric cancer was only made posthumously. It illustrates how the burden of gastric cancer is underestimated in Zambia.
Patient Information
The patient was 23 years of age with three a months' history of ill-health. She initially presenting with symptomatic anaemia, abdominal pain and progressive abdominal distension. She denied history of hematemesis but admitted to passing black coloured stool prior to presentation. She was nulliparous with a history of normal menses. Our patient was single, self-employed and had completed her grade 12 education. She had no history of smoking or alcohol intake and had no known family history of malignancies or chronic illnesses. A week prior referral to UTH, she was admitted at a local hospital where she presented with ahaemoglobin of 5.8g/dl. She was transfused 2 units of whole blood. Details from the local hospital were scanty.
Clinical Findings
The patient's blood pressure was 117/93mmHg, pulse rate 114 beats/minute, oxygen saturation was 98% on room air, temperature35.9 0C and arespiratory rate of 20 breaths/minute. She was ill looking in distress, but alert and orientated with pallor and bilateral pedal oedema. She had no jaundice or no lymphadenopathy.
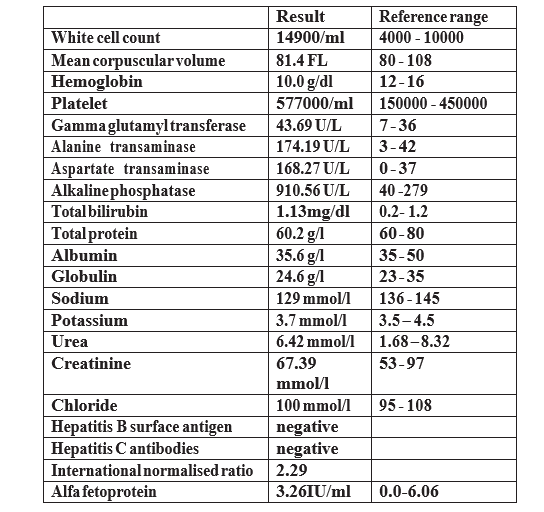
Abdominal examination revealed a grossly distended abdomen with visible abdominal veins, ascites, a palpable nodular liver 10cm below the costal margin and tenderness in epigastrium. Digital rectal exam revealed melena with no palpable masses. She had a haemic murmur and respiratory and neurologic examination were unrevealing. Investigations were ordered and were as shown in table 1.
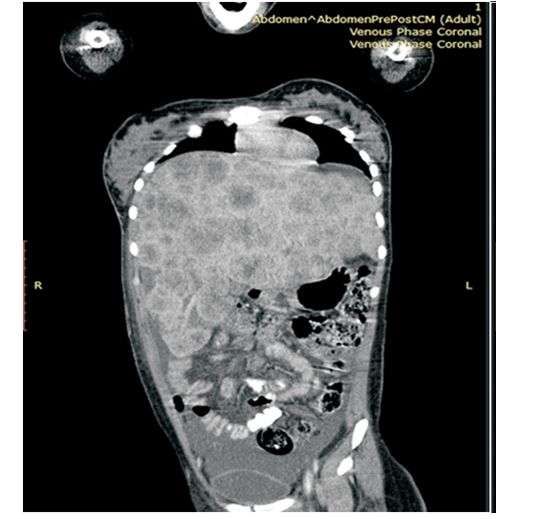
Evaluation using Transient Elastography (Fibroscan)revealed evidence of a stiff liver (75Kpa). On abdominal ultra sound scan, gross ascites was confirmed with poor visibility of the liver. However, Computerised tomography scan revealed multiple nodules in the liver as shown in Figure 1. There were also some deposits in the lungs. Doppler ultrasound of both limbs showed no evidence of deep vein thrombosis. The alpha feto protein was normal.
An initial diagnosis of non- cirrhotic hepatocellular carcinoma was made with a differential of metastatic liver disease unknown primary. Budd Chiari Syndrome was also entertained as a differential.
Therapeutic Intervention
Patient was admitted and started on supportive treatment, morphine 10mls per oral four times a day, lactulose 15mls per oral three times a day and metoclopramide 10mg intravenously three times a day. Patient was started on diuretics for the ascites and proton pump inhibitors in view of the gastrointestinal bleeding. An upper gastrointestinal endoscopy was planned after transfusion of two units of blood.
Follow-up and Outcomes
During subsequent reviews, the patient kept deteriorating clinically with blood results showed persistently elevated liver enzymes. Of note was marked elevation of alkaline phosphatase (a marker of bone metastasis). On day 10 post-admission patient continued to deteriorate with last review showing a hypotension of 75/55beats per minutes and a hypoglycaemia of 2.2mmol/l. Resuscitation attempts with inotropes, dextrose and oxygen therapy were instituted but the patient died later the same day.
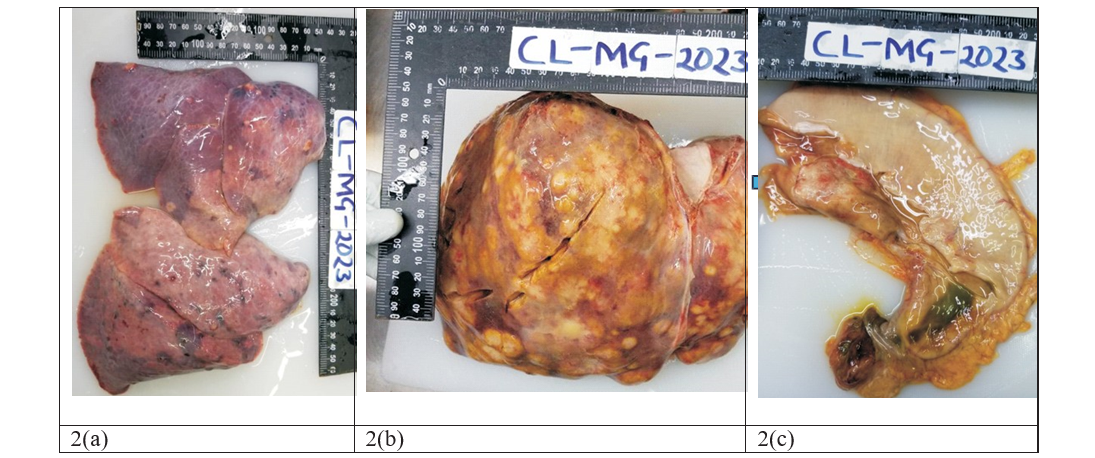
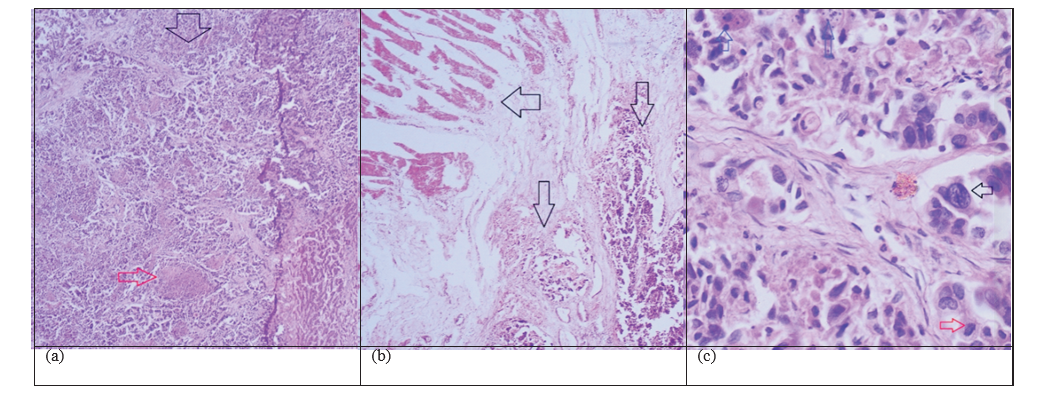
A clinical post-mortem was done and revealed primary gastric adenocarcinoma with metastasis to the liver, pancreas and lungs (images shown figure 2).Histology images are also shown in figure 3.
DISCUSSION
Our case report seeks to raise awareness of gastric cancer in Zambia. Our patient had short duration of illness and presented with advanced metastatic disease which was unfortunately diagnosed posthumously. Our patient was only 23years of age and as such we think our case will help clinicians to think of gastric cancer in young patients who present with symptoms of anaemia. Our patient was not a smoker and she was a teetotaller.
Gastric cancer is one of the medical conditions that requires invasive approaches for diagnosis, the main one being endoscopy. But due to related high running costs and demand on specialised personnel, endoscopy is not available in many health centres within Zambia. Therefore, the onus remains on the healthcare provider to refer suspected cases to centres that can diagnosegastric cancer. The major challenge that practitioners face is that gastric cancer has no specific symptoms[11] . In very early stages, it is completely asymptomatic. Later on, the patient might develop non-specific symptoms such as abdominal pain. The traditional alarm symptoms such as persistent vomiting, microcytic anaemia, unexplained weight loss, haematemesis or melaena present much later in the disease process[12] . Therefore, practitioners have to have a high index of suspicion for gastric cancer in order for them to request for an endoscopy. The initial symptoms that the patient being reported here presented with (anaemia, abdominal pain and distension) are late signs of gastric cancer. It is quite likely that she could have had other minor symptoms much earlier which were either ignored or treated inappropriately. It is possible that she did not even seek medical assistance for the early symptoms. The challenge of early diagnosis of gastric cancer is therefore a significant one.
The patient had no known family history of gastrointestinal malignancies but that does not rule out the genetic component.Gastric cancer is known to have some genetic predisposition particularly in individuals with specific mutations on genes such as the CDH1, APC, SMAD4 and Lynch syndrome genes (MLH1, MSH2, MSH6, EPCAM)[13] . We previously conducted a study which revealed a high occurrence of gastric tumours showing evidence of microsatellite instability[9] . In addition, we found that up to 23 % of gastric cancers in Zambia were positive for HER2 overexpression[14] . These molecular characteristics of gastric cancer have an impact on the prognosis of gastric cancer. In this case report, we did not have details of the molecular sub-type of the cancer that the patient had.
Salted and salty foods have long been associated with a modest 50% to 100% increased risk of gastric cancer in epidemiologic research conducted among diverse populations across the world[15,16] .Dietary intake of salt has been associated with increased incidence and mortality of gastric cancer. In a review of salt intake and mortality in 24 countries, Joossens et al., suggest that salt intake is a risk factor for stomach cancer mortality[17] . Prior studies have shown that the average salt intake in Zambia is above the WHO recommended levels[18] ,however in our patient, it was unclear if there was increased salt intake.
We did not have information on Helicobacter pylori (H. pylori) infection in the patient. H. pylori is the single most important risk factor for gastric cancer. However, the current understanding is that H. pylori related gastric carcinogenesis takes several years to occur[19] . Even if this patient acquired it in childhood, the number of years would not be enough to attribute this cancer to H. pylori alone. The peak age for developing gastric cancer is 60-80 years[20] . With evidence of a high occurrence of early onset gastric cancer in Zambia[7,8] , is it very likely that there are some other factors beyond H. pylori that accelerate the carcinogenesis process. One such factor is biomass smoke. We previously reported that exposure to biomass smoke was a significant risk factor for gastric cancer in Zambia[8,21,22] . As it is not possible to know how much exposure this patient had, we cannot know if at all it played a role.
There is evidence that gastric cancer is commoner among Zambians of a lower socio-economic status[8] . Our patient was similarly from a low socioeconomic environment but it remains unclear which exact factors within her environment would have led to the disease.
It is true that by the time we saw this patient, palliative care was the only option. However, it is possible that if the diagnosis had been made earlier, there could have been room for curative therapy. We, therefore, advocate for enhanced efforts aimed at improving early gastric cancer diagnosis in Zambia.
Limitations of the case
Details of what transpired between the onset of symptoms and referral to UTH are scanty. We also did not have information on molecular characteristics of the cancer to facilitate inferrance on what could have caused its development at such an early age. In addition, we did not have information on H. pylori infection, which is a major risk factor for gastric cancer. H. pylori is prevalent in Zambia but knowing the status when the patient already had a metastatic gastric cancer would have had no impact on patient management.
CONCLUSION
This is a case of gastric cancer diagnosed posthumously. Without a high index of suspicion for gastric cancer among young patients, such cases will continue occurring in Zambia. And if post-mortems are not done, they will not be reported.
DECLARATIONS
Acknowledgments
Dr Chola Mulenga and Dr Sabuni Mwimanenwa- registrars in the department of internal medicine who helped in the management of the patient during admission at UTH.
All authors had no conflict of interest.
REFERENCES
- Ferlay J, Ervik M, Lam F, Colombet M, Mery L, Piñeros M, Znaor A, Soerjomataram I, Bray F (2020). Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. Available from: https://gco.iarc.fr/today, accessed [12th January 2024]
- Kayamba V, Kelly P. Delayed referral for diagnostic endoscopy is a contributing factor to late gastric cancer diagnosis in Zambia. Health Press. 2019 Feb;3(2):14-19.
- Ramos MFKP, Ribeiro Júnior U, Viscondi JKY, Zilberstein B, Cecconello I, Eluf-Neto J. Risk factors associated with the development of gastric cancer - case-control study. Rev Assoc Med Bras (1992). 2018 Jul;64(7):611-619. doi: 10.1590/1806-9282.64.07.611.
- Machlowska J, Baj J, Sitarz M, Maciejewski R, Sitarz R. Gastric Cancer: Epidemiology, Risk F a c t o r s , C l a s s i f i c a t i o n , G e n o m i c Characteristics and Treatment Strategies. Int J Mol Sci. 2020 Jun 4;21(11):4012. doi: 10.3390/ijms21114012.
- Lauren P. The two histological main types of gastric carcinoma: diffuse and so-called intestinal-type carcinoma. An attempt at a histo- clinical classification. Acta Pathol Microbiol S c a n d . 1 9 6 5 ; 6 4 : 3 1 - 4 9 . d o i : 10.1111/apm.1965.64.1.31.
- Yusefi AR, Bagheri Lankarani K, Bastani P, Radinmanesh M, Kavosi Z. Risk Factors for Gastric Cancer: A Systematic Review. Asian Pac J Cancer Prev. 2018 Mar 27;19(3):591-603. doi: 10.22034/APJCP.2018.19.3.591.
- Kayamba V, Asombang AW, Mudenda V, Lisulo MM, Sinkala E, Mwanamakondo S, Mweemba I, Kelly P. Gastric adenocarcinoma in Zambia: a case-control study of HIV, lifestyle risk factors, and biomarkers of pathogenesis. S Afr Med J 2013;103: 255-259. doi: 10.7196/ samj.6159.
- Kayamba V, Zyambo K, Mulenga C, Mwakamui S, Tembo MJ, Shibemba A, Heimburger DC, Atadzhanov M, Kelly P. Biomass Smoke Exposure Is Associated with Gastric Cancer and Probably Mediated Via Oxidative Stress and DNA Damage: A Case-Control Study. JCO Glob Oncol. 2020 Mar; 6:532-541. doi: 10.1200/GO.20.00002.
- Kayamba V, Butt J, Waterboer T, Besa E, Choudhry N, Hamasuku A, Julius P, Heimburger DC, Atadzhanov M, Kelly P. Molecular profiling of gastric cancer in a population with high HIV prevalence reveals a shift to MLH1 loss but not the EBV subtype. Cancer Med 2020 May;9(10):3445-3454. doi: 10.1002/cam4.3001.
- Shumba S, Kayamba V. Analysis of the proportion of university teaching hospital gastric cancer data included in the Zambia national cancer registry. Afr Health Sci. 2023 Mar;23(1):438-443. doi: 10.4314/ahs.v23i1.46.
- Matsuoka T, Yashiro M. Novel biomarkers for early detection of gastric cancer. World J Gastroenterol. 2023 May 7;29(17):2515-2533. doi: 10.3748/wjg.v29.i17.2515.
- Maconi G, Manes G, Porro GB. Role of symptoms in diagnosis and outcome of gastric cancer. World J Gastroenterol. 2008 Feb 28;14(8):1149-55. doi: 10.3748/wjg.14.1149.
- Long JM, Ebrahimzadeh J, Stanich PP, Katona BW. Endoscopic Surveillance in Patients with the Highest Risk of Gastric Cancer: Challenges and Solutions. Cancer Manag Res. 2022 Oct 10;14:2953-2969. doi: 10.2147/CMAR. S277898.
- Kasochi C, Julius P, Mweemba I, Kayamba V. Human epidermal growth factor receptor 2 over expression in gastric and gastroesophageal junction adenocarcinoma in patients seen at the University Teaching Hospital, Lusaka, Zambia. Afr Health Sci. 2020 Dec;20(4):1857-1864. doi: 10.4314/ahs.v20i4.41li>
- Lam SK. 9th Seah Cheng Siang Memorial Lecture: gastric cancer--where are we now? Ann Acad Med Singap. 1999 Nov;28(6):881-9.
- World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR). Continuous Update Project Report: Diet, Nutrition, Physical Activity and Stomach Cancer 2018. Available at dietandcancer.org [accessed on 12thJanuary 2023].
- Joossens JV, Hill MJ, Elliott P, Stamler R, Lesaffre E, Dyer A, Nichols R, Kesteloot H. Dietary salt, nitrate and stomach cancer mortality in 24 countries. European Cancer Prevention (ECP) and the INTERSALT Cooperative Research Group. Int J Epidemiol. 1 9 9 6 J u n ; 2 5 ( 3 ) : 4 9 4 - 5 0 4 . d o i : 10.1093/ije/25.3.494.
- Oelke ND, Rush KL, Goma FM, Barker J, Marck P, Pedersen C. Understanding Perceptions and Practices for Zambian Adults in Western Province at Risk for Hypertension: An Exploratory Descriptive Study. Glob J Health Sci . 2 0 1 5 J u l 8 ; 8 ( 2 ) : 2 4 8 - 5 9 . d o i : 10.5539/gjhs.v8n2p248.
- Take S, Mizuno M, Ishiki K, Yoshida T, Ohara N, Yokota K, Oguma K, Okada H, Yamamoto K. The long-term risk of gastric cancer after the successful eradication of Helicobacter pylori. J Gastroenterol. 2011 Mar;46(3):318-24. doi: 10.1007/s00535-010-0347-9.
- Guenter J. Krejs. Gastric Cancer: Epidemiology and Risk Factors. Digestive Diseases. 2010. 28 (4-5): 600–603.
- Kayamba V, Heimburger DC, Morgan DR, Atadzhanov M, Kelly P. Exposure to biomass smoke as a risk factor for oesophageal and gastric cancer in low-income populations: A systematic review. Malawi Med J. 2017 Jun;29(2):212-217. doi: 10.4314/mmj. v29i2.25.
- Kayamba V, Kelly P. Environmental factors associated with gastric carcinogenesis. Curr Opin Gastroenterol. 2022 Mar 1 ; 38 ( 2 ): 156 - 161 . doi: 10 . 1097 / MOG. 0000000000000812.
Medical Journal of Zambia, Vol 50, 4
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.