Traumatic Dental Injuries in a Tertiary Institution: A 4-Year Retrospective Analysis
Adeyemi MF
Department of Surgery, University Of Ilorin, Ilorin,Kwara State, Nigeria
Ernest MA
Department of Surgery, University Of Ilorin, Ilorin,Kwara State, Nigeria
Sanni-Abdullahi SO
Department of Surgery, University Of Ilorin, Ilorin,Kwara State, Nigeria
Igben Ehigie
Department of Surgery, University Of Ilorin, Ilorin,Kwara State, Nigeria
Garba Ashiru
Department of Surgery, University Of Ilorin, Ilorin,Kwara State, Nigeria
Nnebedum Mirian Nneamaka
Department of Surgery, University Of Ilorin, Ilorin,Kwara State, Nigeria
DOI: https://doi.org/10.55320/mjz.50.3.423
Keywords:Dental Injury, Trauma, avulsion, root fracture, Andreasen’s classification.
ABSTRACT
Background: Traumatic dental injury (TDI) has grown to be a significant public health issue due to its high prevalence as well as the significant negative effects it has on quality of life. This study aimed to examine the prevalence and causes of TDI in a Dental outpatient clinic for 4 years.
Materials and methods: A retrospective study was conducted on 52 TDI patients who were treated at a Tertiary Institution's Dental Outpatient clinic between June 1, 2017, and June 1, 2021. Data on age, gender, aetiology, types of teeth involved, types of dental trauma, the day the incidents occurred, and treatment options were retrieved. Traumatized teeth were classified using Andreasen’s classification. Statistical analysis was carried out using SPSS version 20.0.
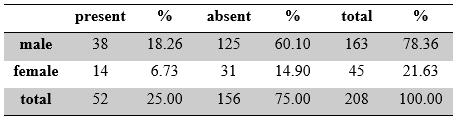
Results: A total of 208 patients with maxillofacial injuries (163 males and 45 females) aged 1 to 81 years were examined. The prevalence of TDI was 25%. Male and female prevalence were 18.2% and 6.7%, respectively. There were 52 TDI patients with a mean age of 16.5 ± 12.02.
The most common reason for TDI was motorcycle accidents at 30.77%. Avulsion (40.67%) and subluxation (50%) were the most frequently diagnosed injuries in the permanent dentition and primary dentition, respectively. There was no association between trauma source and dentition type (p=0.342), nor was there a difference between trauma source and gender (p=0.863).
Conclusion: The study observed that a high percentage of 40.38% had an injury to three or more teeth resulting in attendant functional and aesthetic complications. Hence public health issue that warrants urgent government attention.
INTRODUCTION
Traumatic dental injury (TDI) is one of the most common maxillofacial injuries worldwide.[1-2] Prevalence is high all over the world, this is influenced by location, culture, health insurance policies, and population’s age.[3,4,5,6,7,8] Epidemiological studies from various parts of the world show that the prevalence of TDI varies from 6.4% - 10.5% (9-11) with a male: female of 29.39:14.05. In Brazil, the study of Evelyn et al [9] showed a prevalence of 10.5%, with a male to female ratio of 12.2: 8.8 while Alkhedra et al [10] in Canada reported a prevalence of 6.4% with male to female ratio of 70.9:29.1. In India, Ain et al [11] reported 9.3% with male to female ratio 5.06:4.25. In Nigeria the prevalence is reported to be between 6.96% -9.1% (12-13) Akpata reported a prevalence of 12.4% among children in Lagos, southwest Nigeria.[14] Risk factors associated with a higher prevalence of dental trauma are increased overjet, class II malocclusion, need for orthodontics, and male gender.[7-8]
Previous studies have shown that the oral cavity is the sixth most commonly injured body site, with dental trauma accounting for approximately 5% of all injuries leading to the hospital or outpatient care.[15-16] Various studies show that domestic accident is the main aetiology of TDI in adult [12] while fall is most implicated in children.[17] TDI primarily affects the anterior teeth and can lead to complications such as tooth loss, dislocation/subluxation, crown discoloration, apical periodontitis, ankylosis, pulpal necrosis, and inflammatory root reabsorption. It may also include facial fractures, depending on the severity of the injury.[18,19,20,21,22,23,24] Several studies have shown that the prevalence of dental injury in patients with facial fractures ranges from 13% to 23 %.[4,21,22,25,26]
Traumatic dental injuries (TDIs) can cause aesthetic, social, and psychological problems by affecting a patient's appearance and speech, in addition to functional problems.[27] Prompt and appropriate treatment is necessary to minimize complications and save the affected tooth.
Previous studies have shown that the incidence of TDI is higher late at night and on weekends.[7-18] Traumatic dental injury has great public health burden. This has affected quality of life of people. Most the literature studied traumatic dental injury in children. There is dearth of information on adult population. However, the aim of this retrospective study was to investigate the prevalence and causes of TDI at the dental outpatient clinic of our centre over 4 years in mixed population. Findings from this study will add more references to the literature and also help the government to provide policies to regulate the causes of traumatic dental injury.
MATERIALS AND METHODS
This was a retrospective study of 52 consecutive patients who presented with TDI at University of Ilorin Teaching hospital dental outpatient clinic in Ilorin Kwara State between 1st June 2017 and 1st June 2021 that satisfied the inclusion criteria were selected. Our hospital is the only University Teaching Hospital in the state, which has a population of 3,192,893 people.[28] Our dental unit is the only dental clinic providing specialist care in the city and is frequented by dental patients and sees these patients every day of the week. Patients with incomplete data, traumatic brain injury, edentulous, and no surgical treatment were excluded from the study. Only patients who presented and were treated in our dental outpatient clinic were included in the study and analysed.
All the experiments in this study were conducted in accordance to relevant guidelines and regulations. This research was approved by Ethical review committees of the Ministry of Health, Ilorin, Kwara State (ERC Approval Number: ERC/MOH/2022/10/077). Informed consent was obtained from all subjects and/or their legal guardian(s). A semi-structured questionnaire was used to obtain necessary information, including socio-demographic characteristics, while relevant clinical examination findings such as date of the incident, type of dental fracture/injury, location of the damaged tooth, and tooth injury related to facial fracture location and treatment options of a consultant maxillofacial surgeon and trained dentists were recorded. Each patient was examined with the use of routine examination set such as mouth mirrors, examination probes, college tweezers and gauge. Other necessary investigations such as vitality test and radiographic assessment were done. Tooth injuries were classified according to Andreasen’s classification.[29]
Analysis was done using Microsoft Excel 2010 (Redmond, WA, USA) and SPSS 22 (IBM, Armonk, NY, USA. The chi-square test was used for the analysis of non-parametric variables such as gender, types of dental injury, teeth involved, and aetiology of trauma. Statistical significance was set at p<0.05.
RESULTS
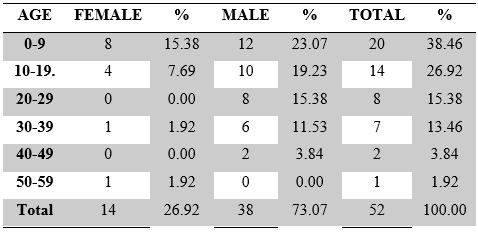
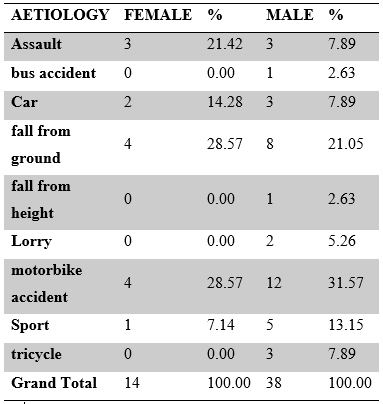
A total of 208 patients with maxillofacial injuries (163 males and 45 females) aged 1 to 81 years were examined. The prevalence of TDI was 25%. Male and female prevalence were 18.2% and 6.7%, respectively (Table 1). There were 52 TDI patients observed, with a mean age of 16.5 ± 12.02 and 28 (73.07%) males and 14 (26.92%) females (p < 0.003). The age ranged from 2 years to 50 years. More than 90% (49) of the patients were below 40 years. (Table2). The most frequent reason for TDI (table 3) was motorbike accident (30.77%, n= 52), followed by falls from ground (23.08%, n=12) and assault (11.53%, n=6).
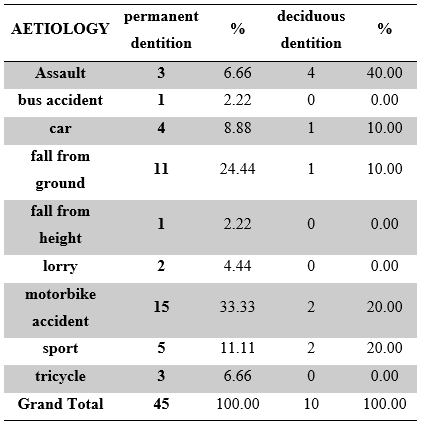
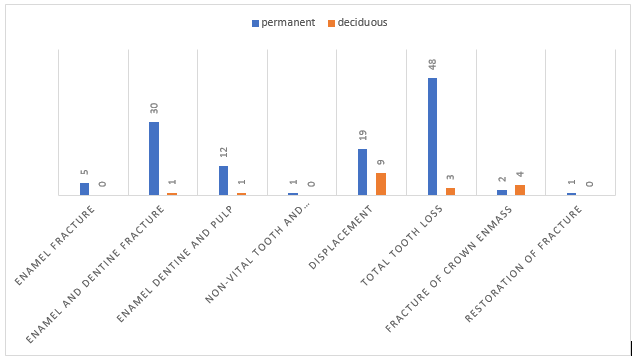
There was no association between trauma source and gender (p=0.863); table 3), nor was there a significant difference in trauma source compared to dentition type (p=0.342) (table4). Periodontal injuries were found to be the most common injuries in both permanent and deciduous teeth. Only 1 tooth was affected in (37.7%, n = 20) cases, 2 teeth were damaged in (21.2%, n = 11), and 40.38% (n = 21) had Three or more teeth affected. A total of 136 teeth were affected, with an average of 2.61 teeth damaged per patient. The upper central incisors were most commonly affected (38.9% n=53 Fig 1). For permanent Dentition; a total of n=118 teeth were involved in 45 patients. The most diagnosed injury was total tooth loss (40.67%, n=48) followed by enamel dentine fracture without pulp exposure (25.42%, n=30). But for deciduous dentition; a total of n=18 teeth were involved in 10 patients, and the most diagnosed injury was subluxation (50%, n=9) followed by total tooth loss (16.6%, n=3).

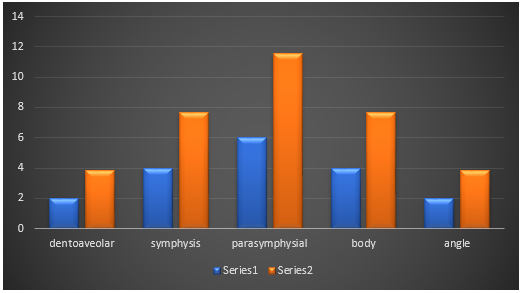
The most frequently diagnosed injury was avulsion (37.5%, n=51), followed by enamel-dentine fracture (22.79%, n= 31) then subluxation (20.58%, n=28 fig. 2). While 44 out of 52 patients had associated middle-third facial fractures. A total of 34 out of 52 patients (65.4%) had maxillary dentoalveolar fractures followed by (2, 9.1%) of Le fort 11 fractures.10 out of 52 patients had an associated combination of mandibular fractures fig.3. A total of (18 out of 52, 34.62%) traumatic dental injury patients had associated mandibular fractures .majority of them were parasymhyseal fractures (6, 11.5%) followed by symphysis and body (4, 7.7%) each (fig.4).

DISCUSSION
This study analysed and evaluated the prevalence and causes of TDI in children and adult population. The result show a prevalence of 25% TDI. Road traffic accident and assault were the major cause for permanent and deciduous dentition respectively. There was a significant association between dental trauma source and gender. However there was no significant association between aetiology and type of dentition. This study reported a TDI prevalence of 25%, close to that reported by Rusli et al.[30] of 23.2% while the prevalence of TDI from other Nigerian studies ranged from 6.5% to 19.5 % (31-34). This might be influenced by the difference in geographical locations. Prevalence is 66% in Korea 27.7% [35] in the UK 11%[36] in Greece and 8.4%[37] in France.[38] This range could be explained by other health insurance systems. In this study, the average age was 16.5 years ± 12.02, 73.1% Male and 26.9 % Female; M; F ratio of 2.7:1, this commensurate with other studies on the same topic (11,14,17,18) but the contrast to the finding in the study by Mahmoodi et al[27] where the average age of 14.7± 15.720. This could be attributed to varying sample sizes.
Some studies[40,41,42] have reported a change in the global cause of TDI from RTA to sports accidents but in our study, RTA by motorcycle was the highest cause of injury in adults and assault followed by fall were the highest cause of injury in deciduous dentition. As it is with previous studies, we had a significant male predominance, many of these studies reported a ratio of 2:1[22,23,24,25,42] while our study had a ratio of 3.6:1. This could be attributed to few numbers of females being involved in commercial motorcycle riding in this environment. Women tend to be less prone to trauma,[5-6] violent behaviour and participation in more aggressive types of activities than men.[30]
A high share percentage of patients are in 0-9yrs with a continuous decrease in age which is in tandem with the literature.[5,6,43] This may be brought on by poor motor coordination as well as observant and adventurous behaviour[39] in children. Periodontal injuries (subluxation and avulsion) are the most frequent injuries in children, with subluxation accounting for 50% of the case in the current study. Several studies[5,6,43] have found a similar trend in deciduous dentition. In this study, the most common injury in permanent dentition was total tooth loss (40.67%), which contrasts with most literature, which reported a higher proportion of enamel and dentine without pulp exposure ranging from 20.2% to 51.6%.[4-40] However, the proportion of enamel and dentin without pulp reported in this study is similar to that in the most reported literature, the plausible explanation being that the permanent teeth are more firmly embedded in the alveolar bone and are more likely to fracture.[21] which has been attributed to the higher elasticity of the supporting tissues, the relatively small roots and reduced alveolar bone support in deciduous dentition.
In our study TDI is more associated with middle third fracture than mandibular fracture this corresponds to the findings by Thoren (21), da Silva et al[25] , and Roccia et al[26] but is in divergence to the findings by Previous authors who reported that TDI was significantly more associated with mandibular fractures.[22,25,26,27,28,29,30] An explanation for this may be differences in the mechanism of injuries in which the majority of the TDI in our study were caused by motorcycle accidents, unlike other studies which were due to sports accidents.
In contrast to findings by Iso-Kungas[23] who reported a high prevalence of TDI in the symphyseal region of the mandible, our study revealed a high prevalence in the parasymphyseal region of the mandible. This might be due to the mechanism of the injury which is major as a result of a motorbike accident in our setting. However, this differs from the study results of Roccia et al.[25] in which mandibular condylar fracture was the most common bone fracture associated with TDI. Our study showed an average of 2.61 (n=136) injured teeth per patient, with the upper incisors being the most injured teeth, the average injured teeth being higher compared to previous studies.[5,6,21] This might have been a result of a lower number of participants in our study compared to others. However, the maxillary incisors being the most injured teeth are in line with international literature.[5-6] Appropriate preventative measures can be achieved by orientating commercial motorcyclists on the importance of Helmets for them and their passengers. Stricter laws on the use of seatbelts and tough penalties against drunk driving should be put in place.
A high percentage of patients with avulsion injuries could not present the affected teeth for reimplantation. Rehabilitation with prosthesis and space maintainers were done for the adults and children respectively. Children who suffered mild subluxation with deciduous teeth whose teeth are at the exfoliation stage were placed on observation and medication. Traumatic dental injuries that occur daily in the dental clinic cannot be completely eradicated, so efforts should be directed towards preventive measures such as educational programs for teachers, parents, careers, coaches, and paramedics that could help reduce the long-term effects of trauma and minimize and achieve better prognosis through prompt and proper treatment. And a reduction of environmental risk factors such as encouraging the use of the frictional type of tiles on the floor against the use of a slippery type of tiles.
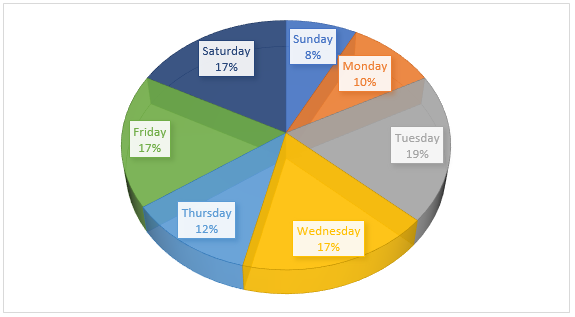
Two-thirds of the accidents happened during the weekdays in this study which is in contrast to some studies in which most of the incidents happened during weekends.[37-38] This could be because the aetiology in these reports were sports accident which is mostly played on weekends while the most frequent aetiology in our report was commercial motorcycle accident which is on daily basis. The range of prevalence might have been influenced by different cultural and socioeconomic diversity.
Limitations to this study included the fact that some TDI patients were also admitted and discharged from the hospital’s emergency without presenting at the dental outpatient clinic. This could account for the low figure of the total number of patients with TDI. Most patients with non-severe TDI are not likely to present to the hospital. This might be due to the socio-economic status of the majority of the Ilorin dwellers. Bias may have been introduced in this study because data were collected retrospectively. Nevertheless, the results of this study were largely consistent with those of other studies.
CONCLUSION
In conclusion, our study underscores the alarming prevalence of Traumatic Dental Injuries (TDI) in our population, revealing a concerning 25% incidence rate. Notably, the primary contributors to TDI differed between permanent and deciduous dentition, with road traffic accidents being the predominant cause for permanent dentition injuries, while assaults were identified as the major instigators for deciduous dentition trauma. Furthermore, our analysis revealed a significant association between the gender of individuals and the source of dental trauma, emphasizing the need for targeted preventive measures. Addressing the root causes of these injuries through comprehensive educational programs becomes imperative. Targeting teachers, parents, caregivers, coaches, and paramedics with preventative strategies and primary care knowledge could prove instrumental in minimizing the immediate and long-term consequences of dental trauma.
Early intervention and correct treatment are vital in improving prognosis and reducing the burden on both individuals and the healthcare system. To mitigate the pervasive impact of TDI, we recommend the implementation of robust educational initiatives. These programs should not only focus on creating awareness but also on imparting practical skills for timely and effective response to dental emergencies. Furthermore, a multidisciplinary approach involving collaboration between healthcare professionals, educators, and policymakers is crucial for the successful implementation of preventive measures. Our study also highlights the need for further research in this field. Future investigations should delve into the prevalence and management of TDI patients, considering factors such as socio-economic status, access to healthcare, and regional variations. Longitudinal studies could provide valuable insights into the lifelong consequences of dental trauma, aiding in the development of targeted intervention strategies and rehabilitation programs.
REFERENCES
- Petti S, Glendor U, Andersson L. World traumatic dental injury prevalence and incidence, a meta-analysis—one billion living people have had traumatic dental injuries. Dent Traumatol. 2018; 34(2):71–86.
- Alberto M, Dello D, Luigi G, Roberto A, Vittorio C, Vittorio C. Traumatic Dental Injuries: Clinical Case Presentation and a 10-Year Epidemiological Investigation in an Italian Dental Emergency Service. Case Rep Dent. 2021; 2021: 8649663.
- Rhouma O, McMahon AD, Conway DI, Armstrong M, Welbury R, Goodall C. Facial injuries in Scotland 2001–2009: epidemiological and sociodemographic determinants. Br J Oral Maxillofac Surg. 2013; 51 (3):211–6.
- Glendor U. Aetiology and risk factors related to traumatic dental injuries--a review of the literature. Dent Traumatol. 2009; 25 (1):19–31.
- Glendor U. Epidemiology of traumatic dental injuries--a 12 year review of the literature. Dent Traumatol. 2008; 24(6):603–11.
- Bucher K, Neumann C, Hickel R, Kuhnisch J. Traumatic dental injuries at a German university clinic 2004–2008. Dent Traumatol. 2013; 29(2):127–33.
- Borzabadi-Farahani A, Borzabadi-Farahani A. The association between orthodontic treatment need and maxillary incisor trauma, a retrospective clinical study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011; 112(6):75–80.
- Borzabadi-Farahani A, Borzabadi-Farahani A, Eslamipour F. An investigation into the association between facial profile and maxillary incisor trauma, a clinical non-radiographic study. Dent Traumatol. 2010; 26(5):403–8.
- Soriano EP, Caldas Jr AD, Carvalho MV, Amorim Filho HD. Prevalence and risk factors related to traumatic dental injuries in Brazilian schoolchildren. Dent Traumatol. 2007 Aug; 23(4):232-40.
- Alkhadra T, Preshing W, El-Bialy T. Prevalence of traumatic dental injuries in patients attending University of Alberta Emergency Clinic. The Open Dentistry Journal. 2016; 10:315.
- Ain TS, Telgi RL, Sultan S, Tangade P, Telgi CR, Tirth A, Pal SK, Gowhar O, Tandon V. Prevalence of traumatic dental injuries to anterior teeth of 12-year-old school children in Kashmir, India. Archives of Trauma Research. 2016 Mar; 5(1).
- Oginni AO, Adekoya-Sofowora CA. Pulpal sequelae after trauma to anterior teeth among adult Nigerian dental patients. BMC Oral Health. 2007 Dec; 7(1):1-5.
- Enabulele JE, Oginni AO, Sede MA, Oginni FO. Pattern of traumatised anterior teeth among adult Nigerians and complications from late presentation. BMC Research Notes. 2016 Dec; 9(1):1-6.
- Akpata ES. Traumatized anterior teeth in Lagos school children. J Med Assoc 1969; 6: 40-45
- Petersson EE, Andersson L, Sorensen S. Traumatic oral vs non-oral injuries. Swed Dent J. 1997; 21(1–2):55–68.
- Lin S, Levin L, Goldman S, Peleg K. Dento-alveolar and maxillofacial injuries: a 5-year multi-centre study. Part 1: general vs facial and dental trauma. Dent Traumatol. 2008; 24(1):53-5.
- Apias MA, Jimenez-Gracia R, Lamas F, Gil AA. A Prevalence of traumatic crown fractures to permanent incisors in a childhood population; Mostoles, Spain. Dent Traumatol. 2003; 19: 119-122.
- van den Bergh B, Karagozoglu KH, Heymans MW, Forouzanfar T. A. Aetiology and incidence of maxillofacial trauma in Amsterdam: a retrospective analysis of 579 patients. J Craniomaxillofac Surg 2012; 40:165–9.
- Al Ahmed HE, Jaber MA, Abu Fanas SH, Karas M. The pattern of maxillofacial fractures in Sharjah, United Arab Emirates: a review of 230 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004; 98:166–70.
- Bali R, Sharma P, Garg A, Dhillon G. A comprehensive study on maxillofacial trauma conducted in Yamunanagar, India. J Inj Violence Res 2013; 5:108–16.
- Thoren H, Numminen L, Snall J, Korni E, Lindqvist C, Lizuka T. Occurrence and types of dental injuries among patients with maxillofacial fractures. Int J Oral Maxillofac Surg 2010; 39:774–8.
- Lieger O, Zix J, Kruse A, Iizuka T. Dental injuries in association with facial fractures. J Oral Maxillofacial Surg 2009; 69:1680–4.
- Iso-Kungas P, Tornwall J, Suominen AL, Lindqvist C, Thoren H. Dental injuries in paediatric patients with facial fractures are frequent and severe. J Oral Maxillofacial Surg 2012; 70:396–400.
- Zhou HH, Ongodia D, Liu Q, Yang RT, Li ZB. Dental trauma in patients with maxillofacial fractures. Dent Traumatol. 2013; 29:285–90.
- Da Silva AC, Passeri LA, Mazzonetto R, De Moraes M, Moreira RW. Incidence of dental trauma associated with facial trauma in Brazil: a 1-year evaluation. Dent Traumatol. 2004; 20:6–11.
- Roccia F, Boffano P, Bianchi FA, Ramieri G. An 11-year review of dental injuries associated with maxillofacial fractures in Turin, Italy. J Oral Maxillofac Surg. 2013; 17:269–74.
- Mahmoodi B, Rahimi-Nedjat R, Weusmann J, Azaripour A, Walter C, Willershausen B. Traumatic dental injuries in a university hospital: a four-year retrospective study. BMC Oral Health. 2015; 15(1):1-7.
- Population 2006-2016, National Bureau of Statistics, https://nigerianstat.gov.ng/elibrary/read/474, (Accessed on 7th October, 2022)
- Pagadala S, Tadikonda DC. An overview of classification of dental trauma. International Archives of Integrated Medicine, 2015; 2(9): 157-164.
- Muhammad Ruslin1, Jan Wolff, Paolo Boffano, Henk S. Brand, Tymour Forouzanfar Dental trauma in association with maxillofacial fractures: an epidemiological study. Dent Traumatol. 2015; 4:318-323.
- Agbelusi GA, Jeboda SO. Traumatic fracture of anterior teeth in 12-year old Nigerian children. Odontostomatol Trop. 2005; 28:23–7.
- Otuyemi OD. Traumatic anterior dental injuries related to incisor overjet and lip competence in 12-year-old Nigerian children. Int J Paediatr Dent. 1994; 4:81–5.
- Adekoya-Sofowora CA, Adesina OA, Nasir WO, Oginni AO, Ugboko VI. Prevalence and causes of fractured permanent incisors in 12-year-old suburban Nigerian schoolchildren. Dent Traumatol. 2009; 25:314–7.
- Taiwo OO, Jalo HP. Dental injuries in 12-year old Nigerian students. Dent Traumatol. 2011; 27:230–4.
- Bae JH, Kim YK, Choi YH. Clinical characteristics of dental emergencies and prevalence of dental trauma at a university hospital emergency centre in Korea. Dent Traumatol. 2011; 27(5):374–8.
- Portman-Lewis S. An analysis of the out-of-hours demand and treatment provided by a general dental practice rota over a five-year period. Prim Dent Care. 2007; 14(3):98–104.
- Lygidakis NA, Marinou D, Katsaris N. Analysis of dental emergencies presenting to a community paediatric dentistry centre. International Journal of Paediatric Dentistry, 1998; 8(3):181-190.
- Tramini P. Al Qadi Nassar B, Valcarcel J, Gibert P. Factors associated with the use of emergency dental care facilities in a French public hospital. Spec Care Dentist. 2010; 30(2):66–71.
- Santos SE, Marchiori EC, Soares AJ, Asprino L, de Souza Filho FJ, de Moraes M. A 9-year retrospective study of dental trauma in Piracicaba and neighbouring regions in the State of Sao Paulo, Brazil. J Oral Maxillofac Surg. 2010; 68(8):1826–32.
- Bae JH, Kim YK, Choi YH. Clinical characteristics of dental emergencies and prevalence of dental trauma at a university hospital emergency centre in Korea. Dent Traumatol. 2011; 27(5):374–8.
- Gassner R, Tuli T, Hachl O, Rudisch A, Ulmer H. Craniomaxillofacial trauma: a 10 year review of 9543 cases with 21067 injuries. J Craniomaxillofac Surg 2003; 31:51–61.
- Hecova H, Tzigkounakis V, Merglova V, Netolicky J. A retrospective study of 889 injured permanent teeth. Dent Traumatol. 2010; 26(6):466–75.
- Portman-Lewis S. An analysis of the out-of-hours demand and treatment provided by a general dental practice rota over a five-year period. Prim Dent Care. 2007; 14(3):98–1042.
Medical Journal of Zambia, Vol 50, 3
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.