Pattern of Mandibular Fractures in a Nigerian Tertiary Health institution; a 4-year retrospective study
Adeyemi Moshood Folorunsho
Department of Surgery, University of Ilorin, Ilorin
Ernest Moninuola Adebusola
Department of Surgery, University of Ilorin Teaching Hospital Ilorin, Ilorin
Sanni-Abdullahi Shakira O
Department of Surgery, University of Ilorin Teaching Hospital Ilorin, Ilorin
Igben Ehigie
Department of Surgery, University of Ilorin Teaching Hospital Ilorin, Ilorin
Garba Ashiru
Department of Dental Surgery, Sir Yahaya Memorial Hospital Birnin Kebbi, Kebbi State
Nnebedum Mirian Nneamaka
Department of Surgery, University of Ilorin Teaching Hospital Ilorin, Ilorin
DOI: https://doi.org/10.55320/mjz.50.3.422
Keywords:mandibular fractures, mechanism of injuries, collision, crash-helmet, aetiology, prevention
ABSTRACT
Background: According to surveys, mandibular injuries aetiology varies between countries and even between centres in the same country. Mandibular fractures are the second most frequent facial injury, accounting for 15.5% to 59% of all facial fractures globally. The study aimed to find out if there were predictable patterns of fractured in the north central part of Nigeria.
Materials and Methods: Mandibular fracture patients treated during a 4-year period were identified in a retrospective analysis and examined based on factors including age, sex, mode of trauma, month and day of the week of presentation, number and anatomic location, treatment method and sequelae.
Results: The study reviewed 75 participants between the ages of 2 and 70. The mean age was 30.69 ± 11.22 years, and the gender split was 70 males (93.20%) and 5 females (6.80%), with a p-value of 0.09. The main cause was motorbike accident (51, 68%) and head on collision was the major mechanism of trauma road traffic accidents (52, 68.8%) and none of motorbike riders nor did passengers wear crash helmet. A total of ninety-nine fractures out of one hundred and six fractures were observed in males. A small percentage of patients (25, 33%) exhibited altered consciousness, however there was no statistically significant link between the aetiology and level of consciousness (p=0.818).
Conclusion: The mandibular body was most severely impacted and the primary mechanism of injury was head-on collision between two motorbikes. Speed restrictions and legislative law should be placed on the use of crash helmet.
INTRODUCTION
The mandible is the largest and strongest facial bone. Its unique feature of being the only movable bone of the skull[1] makes it vulnerable to fractures. Surveys show that mandibular injuries aetiology varies between countries and even between centres depending on the prevailing socioeconomic, cultural, and environmental factors in the same country. Mandibular fractures are the second most frequent facial injury, accounting for 15.5% to 59% of all facial fractures globally [1-4] .
Mandibular fractures occur commonly in Nigeria. Olasoji et al[4] , Adebayo et al [5] and Oginni et al[6] reported mandibular fractures accounting 66.02%, 68% and 69.13% respectively of all maxillofacial injuries in their studies. Most mandibular injuries in Nigeria are due to crashes[7,8,9,10] on slick roads, reckless motorcycle riding, and driving while intoxicated.[11-12] Complications arising from mandibular fracture such as Chronic pain, chewing and obstructive airway, prolonged hospital stay, loss of work hours and worsened social qualities of the patients and place a huge economic burden on treatment of mandibular fracture[7,8,13,14,15,17] .
Despite many reports about the incidence, diagnosis, and treatment of mandibular fracture, there is scarcity of studies investigating the pattern of mandibular fractures in Kwara State North-Central Nigeria. The purpose of this study was to describe the frequency and pattern of mandibular fractures seen in a Tertiary Health Institution in North Central Nigeria.
Understanding the epidemiological pattern in our geographical location will help evidence-based approach to prevention and treatment of mandibular fracture in our environment and different environment.
MATERIALS AND METHODS
Patients with mandibular fractures who visited the dental unit of the University of Ilorin Teaching Hospital, North central Nigeria between January 2018 and December 2021 were included in this retrospective study. Records of patients presenting with developmental disorders or pathological fractures were excluded. A specially designed proforma was used to collect the data. Data of interest were patients demographic, anatomic fracture site based on clinical and radiological findings, agent of injury, the use of a protective helmet, weekdays and month of presentation, the loss of consciousness at the time of the injury, and the length of hospital stay and treatment modalities and complication.
The fractures were classified based on the type of combination of fracture and neurological status. Treatment protocol in the study centre during the study period included treatment primary closure of soft tissue defect at the time of presentation, prescription of liquid diet, antibiotics, and pain medications while definitive treatment included open reduction with miniplate and screw fixation or traction with intermaxillary fixation.
The information was entered into a Microsoft Excel spreadsheet and analysed using SPSS Statistics version 22. Categorical variables were presented in numbers and percentages. Qualitative variables were compared using chi-square test. P<=0.05 was considered statistically significant. All the experiments in this study were conducted in accordance to relevant guidelines and regulations. This research was approved by ethical review committees of Ministry of Health, Ilorin, Kwara State. ERC Approval Number: ERC /MOH/2022/10/076. Informed consent was obtained from all subjects and/or their legal guardian(s).
RESULTS
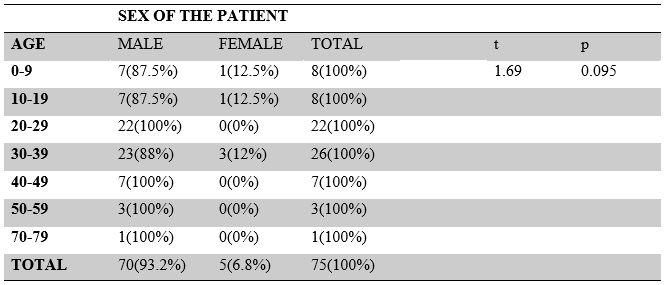
The study sample included 75 participants with ages ranging from 2 to 70, with a mean age of 30.69 ±11.22 years and a 95% confidence interval of 28.11 to 33.27. The study population was composed of 70 males (93.20%) and 5 females (6.80%). There was no difference between the means of the gender ages in the study population p=0.09. The modal age bracket was 30-39 years (26, 34.6%) [Table 1].
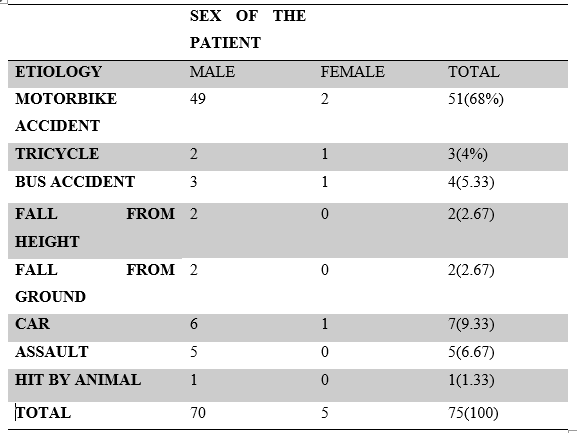
Fifty one (68%) out of 75 of the study participants had Motorbike crash making it the commonest aetiology, followed by nine car crashes, 33% [Table 2]. None of motorbike riders nor passengers used crash helmet.
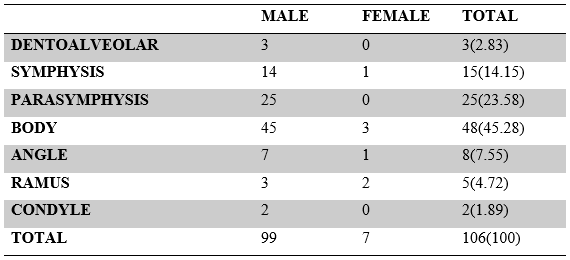
The para-symphyseal region, at 25 (22.32%), was the second-most frequent fracture site after the mandibular body, at 48 (42.86%). The least affected sites were the condyle and dentoalveolar region accounting for 2(1.79 %) and 5 (4.46%) respectively. No coronoid fracture was observed in the data figure 1.


All ramus fractures occurred from motorbike accident and 75 %( 79.5) of the body fracture was due to motorbike crash. The right and left parasymphysis 6.8%(7) was the commonest fracture combination followed by the right and left body fracture 4.1%(4) and the body and angle fracture 4.1%(4) respectively (Figure 3). Majority of the patients had unilateral mandibular fractures 46(61.33%).

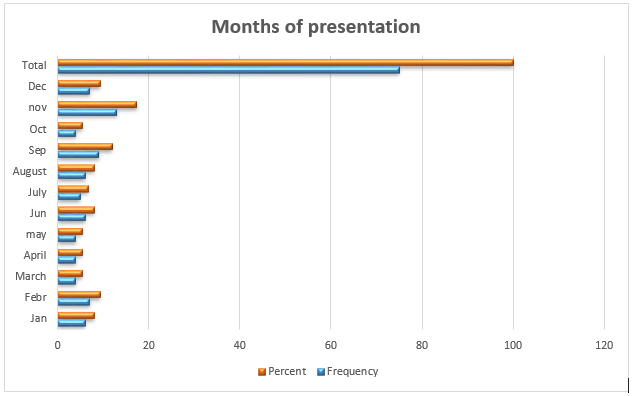
Most patients 44(58.6%) sustained mandibular fractures during the fourth 24(31.9%) and third 20(26.7%) quarters of the years. The modal month was November 13(17.3%) (Figure 4).
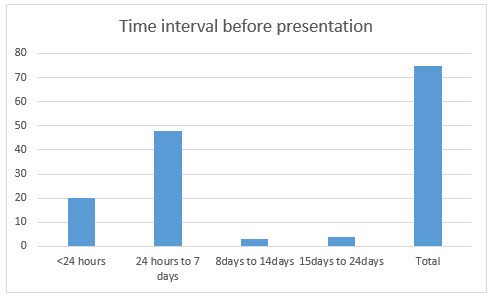
The majority of the participants 48 (64%) presented within the first week of their injuries Twenty-six-point seven percent (20) of participants presented less than 24hours of being injured (Figure 5).
In 25 (33.3%) of the patients, there was an associated altered level of consciousness (Glasgow coma scale less than 15). A few 28(37.25%) of the motorbike accident victims and majority 43 (57.14%) of car accident victims had some level of loss of consciousness. Hundred percent of patients with multilateral fractures were brought in unconscious (Figure 6). There is no statistically significant relationship between level of consciousness and aetiology (p=0.818) or fracture type (p=0.075).
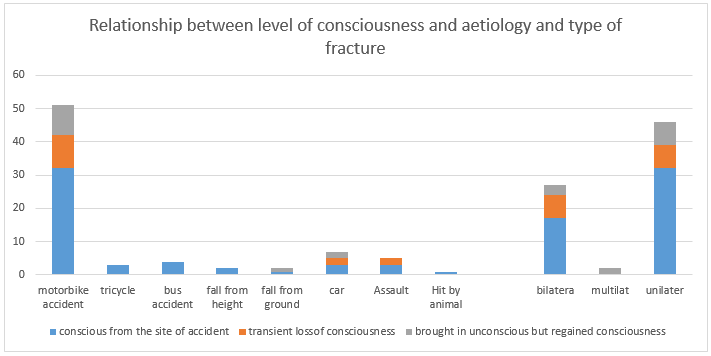
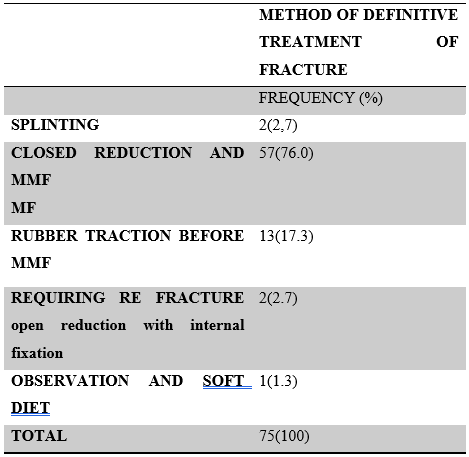
Table 4 shows that two patients (2.7%) with facture mal-union underwent open reduction and internal fixation, as well as 2 weeks maxillomandibular fixation. Most of the patients 57 (76%) had closed reduction and maxillomandibular fixation for six weeks. Few of them 13(17.3%) had slow reduction with rubber traction for one to two weeks before closed reduction with maxillomandibular fixation. The mean of hospital stay was 10.33days ±13.61. The commonest complication associated with closed reduction was trismus and one patient needed corrective surgery for malocclusion.
DISCUSSION
In this study, we discovered that the age distribution is similar to previous reports[7-10] , with males between the second and third decades of life having the highest prevalence of mandibular fractures. The low incidence in younger patients might be due to lower likelihood of prevailing mechanism of injury and bone elasticity in younger age group.
The majority of patients in the current study presented within the first week of their injuries, which is consistent with Oginni et al[18] 2006 and Oginni et al[6] 2016 and many literature in Nigeria. This is however due to referral system in our setting where managing teams could not decide who among to refer to the next level of care and complicated by the concomitant injury at presentation. The delay in presentation might also be due to economic constraint and lack of appropriate transportation from the primary contact to tertiary facilities.
Despite the fact that maxillofacial fractures occurred throughout the year, a peak was seen in November, the fourth quarter (a dry season month in the north central of Nigeria. This period corresponds to end of the year when festive mood such as wedding and Christmas that take place.
In this series, majority of participants that were involved in car accidents had altered level of consciousness but regained consciousness after 24hours. Although the Glasgow coma scores may be a predictor of severity of injuries, our research indicates that car accident was likely to cause altered level of consciousness.
The most common kind of collisions still include motorbikes and other vehicles. However, the percentage caused by motorbike collisions is comparable to earlier reports from Nigeria. [19-20] nevertheless, less so than findings from certain other low- to middle-income nations [21-22] and high-income countries.[23-24] Our study reports 33/75(44 %) head on collision between two motorbikes which was higher than what Oluwadiya et al [27] reported 83 (22.3%) in their study, this might be due to risky behaviour of motorbike riders such as driving against traffic, neglecting to utilize headlights in low-light conditions, riding without a license, and driving while intoxicated although most of them were not captured in this study.
According to this study it was noted that most fractures occurred in the body (42.2%), accounting for about half of the recorded injuries. This is in agreement to some other Nigerian studies[4-11] . Chaurasia et al[8] and Barde et al[26] , however found the parasymphyseal region ranged from 39.8 % to 40.3% to be the commonest fracture site in their geographical location. Coronoid fractures have been reported by various literature as the least mandibular fractures, this is attributed to the protected position it occupies deep under the zygomatic complex and muscle buttresses[27] . We did not record any coronoid facture in this study. Although Singh et al[28] and Shein et al[29] reported incidence of 1.23-3.58% of coronoid fractures in their studies.
The most frequent mandibular fracture combination in our analysis was the right and left body 24.13% fracture. In contrast, Para symphyseal and Angle Fractures were shown to be the most frequent mandibular fracture combination by Sirimaharaj et al.[3] and Natu et al where the most frequently encountered fracture combination was parasymphyseal fracture and subcondylar fracture[15] This difference in the common site of fractures could be attributed to difference in mechanism of impact prevalent in various geographical locations and also major aetiologies in these locations.
The relationship between the injury's mechanism and the mandibular fracture site is statistically significant (p =0.001).100% of the fractures of the ramus occurred due to motorbike accident while 81.5% of the body fracture was attributed also to motorbike crash. 66.6% of the condylar fractures were because of fall from ground. The different aetiologies’ result in different focus of impact hence the hence the association and other external factors that were not captured such as the magnitude, direction, and force of the impact [30-31] and internal factors such as mouth opening [32,33,34] dental states such as third molar impaction[35-36] and characteristics of the bone itself, such as pathological processes, physiological atrophy, and osteoporosis [30] might also be due to the association. However, just a few investigations explored the mechanism underlying mandibular fractures.[30,32,32]
The growing population and urbanization in Nigeria with the limited Government funded and regulated public transportation system have led to the proliferation of the less organized commercial motorcycles and tricycles as a means of movement of people and products within a city. The combination of inherent risk in motorcycle and tricycle, poor compliance on traffic rules by users and bad roads leads to increased road traffic crashes and injuries.[10] All these factors participate in the number of mandibular fractures seen and the pattern of its epidemiology. Efforts should be geared to reduction of environmental (e.g. unsafe road’; road design faults, large pothole) and behavioural risk-factors (e.g. alcohol consumption, high speed, poor maintenance of the vehicle, poor driving skills, noncompliance of wearing of crash-helmet etc.) for mandibular fractures and this may have a great impact on prevention.
In the current study, maxillomandibular fixation was the most often used type of treatment. Slow reduction with elastic band was used for grossly displaced fracture for about week before immobilization for six to seven weeks. Only a small number of individuals received open reduction and internal fixation. This was due to the financial capability of the patients. The majority could not afford the cost of a kit for internal fixation. None of patient treated with open reduction and internal fixation had complication. There was no scar formation in our study because it was intraoral approach.
The study was not left out of limitation. It was a single centre designed study. Some information such as impact’s size and direction of the agent of injury could not be measured. The intrinsic bone characteristic like physiological atrophy, osteoporosis and pathological processes could not be ascertained. These are tough variables to measure. The mechanism of the mandibular fracture should therefore be the subject of multicentre prospective clinical investigation in the future.
CONCLUSION
The pattern of mandibular fracture was highly related to the age and sex while the level of consciousness was correlated with either aetiology or fracture type. The study also demonstrates that the primary mechanism of injury for the cause of mandibular fractures was head-on collision between two motorcyclists, and none of the victims wore a crass helmet. The mandibular body was most severely impacted. Educational programs that inform commercial motorbike riders of the high-speed restriction and place a strong emphasis on the use of crash helmets should be advocated. The findings of this epidemiological pattern will help evidence-based approach to prevention and treatment of mandibular fracture in our environment and different environment.
Conflict of Interest.
All authors declare that they have no conflicts of interest.
Author Contributions
Conceived and designed the experiments: Adeyemi MF (BDS).
Analysed the data: Igben Ehigie
Wrote the paper: Adeyemi MF (BDS)
Substantial contribution to acquisition of data: Nnebedum Mirian Nneamaka
Critically revised article for important intellectual content: Garba Ashiru
Critically reviewed the manuscript: Ernest MA, Sanni-Abdullahi SO
Approved the final version of the manuscript: Adeyemi MF (BDS)
REFERENCES
- Ghodke, M. Shah, S. and Bhoyar, S. Prevalence of mandibular fractures reported at C.S.M.S.S Dental College, aurangabad from february 2008 to september 2009. Journal of International Society of Preventive and Community Dentistry 2013;3(2):51.
- Biju, P. and Mohan, A. Biomechanics of Cranio Maxillofacial Trauma. Journal of Maxillofacial and Oral Surgery 2012;11(2):224–30.
- Wimon Sirimaharaj, M.D. FRCS (T), FICS* KPM. The Epidemiology of Mandibular Fractures Treated at Chiang Mai University Hospital: A Review of 198 Cases. The journal of Medical Association of Thailand 2008;(91):868–74.
- Olasoji, H.O. Tahir, A.and Arotiba, G.T. Changing picture of facial fractures in northern Nigeria. British Journal of Oral and Maxillofacial Surgery2002;40(2):140–3.
- Adebayo, E.T. Ajike, O.S. and Adekeye, E.O. Analysis of the pattern of maxillofacial fractures in Kaduna, Nigeria. British Journal of Oral and Maxillofacial Surgery 2003;41(6):396–400.
- Oginni, F. Oladejo, T. and Alake, D. Facial bone fractures in Ile-Ife, Nigeria: An update on pattern of Presentation and care. Journal of Maxillofacial and Oral Surgery 2016;15.
- Adeyemo, W. Laldeine, A. Ogunlewe, M. and James, O. Trends and characteristics of Oral and Maxillofacial injuries in Nigeria: a review of the literature. Head & Face Medicine 2005;1(7).
- Chaurasia, A. and Katheriya, G. Prevalence of mandibular fracture in patients visiting a tertiary dental care hospital in North India. National Journal of Maxillofacial Surgery 2018;9: 123.
- Ugboko, V. Odusanya, S. and Fagade, O. Maxillofacial fractures in a semi-urban Nigerian teaching hospital. International Journal of Oral & Maxillofacial Surgery 1998;27(4):286–9.
- Fasola, A. Nyako, E. Obiechina, A. and Arotiba, J. Trends in the characteristics of Maxillofacial fractyures in Nigeria. Journal of Maxillofacial and Oral Surgery 2003;61(10):1140–3.
- Adekeye, E.O. The pattern of fractures of the facial skeleton in Kaduna, Nigeria. A survey of 1,447 cases. Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology 1980;49(6):491–5.
- Oginni, F. Ajike, S. Obuekwe, O. and Fasola O. A prospective Multicenter Study of Injury Profile, Severity and Risk Factors in 221 Motorcycle Injured Nigerian Maxillofacial Patients. Traffic Injury Prevention 2009;10(1):70–5.
- Cheema, S. and Amin, F. Incidence and causes of maxillofacial skeletal injuries at Mayo hospital in Labore,Pakistan. British Journal of Oral and Maxillofacial Surgery 2006;44(3):232–4.
- Ogundipe, K. Afolabi, A. and Adebayo, O. Maxillofacial fractures in Owo, South Western Nigeria; four year retrospective review of Pattern and treatment outcome. Dentistry. 2012;2:132–4.
- Natu, S.S. Pradhan, H. Gupta, H. Alam, S. Gupta, S. and Pradhan, R. An Epidemiological Study on Pattern and Incidence of Mandibular Fractures. Plastic Surgery International 2012;1–7.
- Chrcanovic, B.R. Factors influencing the incidence of Maxillofacial fractures. Oral and maxillofacial surgery 2012;16(1):3–17.
- Ahmad, A. Jaber, M. Abu fanas, S. and Karas, M. The pattern of Maxillofacial fractures in Sharjah, United Arab Emirate: a review of 230 cases. Oral surg Oral med Oral Pathol Oral Radiol Endodod 2004;98(2):166–70.
- Oginni F.O, Ugboko V.I, Ogundipe O, Adegbehingbe B.O. Motorcycle-Related Maxillofacial Injuries. Journal of Oral and Maxillofacial Surgery 2006; 64:56-62.
- Solagberu, B.A. Ofoegbu, C.K.P. Nasir, A.A. Ogundipe, O.K. Adekanye, A.O. and Abdul Rahman, L.O. Motorcycle injuries in a developing country and the vulnerability of riders, passengers, and pedestrians. Injury Prevention 2006; 12: 266–268.
- Oluwadiya, K.S. Oginni, L.M. Fadiora, S.O. and Olasinde, O.O. Epidemiology of motorcycle injuries in a developing country. West Africa Journal of Medicine 2004; 23.
- Zargar, M. Khaji, A. and Karbakhsh, M. Pattern of motorcycle-related injuries in Tehran, 1999 to 2000: A study in 6 hospitals. Eastern Mediterranean Health Journal 2006; 12: 81–87.
- Sood, S. Survey of factors influencing injury among riders involved in motorized two-wheeler accidents in India: a prospective study of 302 cases. Journal of Trauma 1988; 28: 530–534.
- Broughton, J. Car Occupant and Motorcyclist Deaths, 1994–2002 Prepared for Road Safety Division. Department for Transport. Transport Research Laboratory, London 2005.
- Latorre G, Bertazzoni G, Zotta D, Van Beeck E, Ricciardi, G. Epidemiology of accidents among users of two-wheeled motor vehicles: a surveillance study in two Italian cities. European Journal of Public Health 2002; 12: 99–103.
- Oluwadiya K.S, Kolawole I.K, Adegbehingbe O.O, Olasinde A.A, Olaide A, Uwaezuoke S.C. Motorcycle crash characteristics in Nigeria: Implication for control. Accident Analysis & Prevention 2009; 41(2): 294-298.
- Barde D, Mudhol A, Madan R. Prevalence and pattern of mandibular fracture in Central India. National Journal of Maxillofacial Surgery 2014; 5(2): 153–156.
- Kale T, Aggarwal V, Kotrashetti S, Lingaraj J, Singh A. Mandibuar Coronoid fractures, how rare? The Journal of Contemporary Dental Practice 2015;16(3):222–6.
- Singh A, Bouckaert M.M, Mchenga J, Perumal C. An investigation into the incidence and istribution of fractures of coronoid process in patients presenting at the Sefako Makgatho Health Sciences University, Oral Health Centre. dental journal in Southern Africa 2015;70:384–7.
- Shen, L. Mandibular Coronoid fractures: treatment options. International Journal of Oral and Maxillofacial Surgery 2013;42:721–6
- Reitzik M, Lownie J.F, Cleaton-Jones P, Austin J. Experimental fractures of monkey mandibles. International Journal of Oral Surgery 1978; 7: 100–103. PMID: 98455.
- Rudderman R.H, Mullen R.L. Biomechanics of the facial skeleton. Clinics in Plastic Surgery 1992; 19: 11–29. PMID: 1537212.
- da Fonseca G.D. Experimental study on fractures of the mandibular condylar process (mandibular condylar process fractures). International Journal of Oral Surgery 1974; 3: 89–101. PMID: 4209422.
- Petzel, J.R, Bulles, G. Experimental studies of the fracture behaviour of the mandibular condylar process. Journal of oral and Maxillofacial Surgery 1981; 9: 211–215. PMID: 6948065.
- Cope M.R, Lawlor, M.G. An unusual mandibular dislocation. British Journal of Oral and Maxillofacial Surgery 1985; 23: 112–117. PMID: 3158331.
- Huelke D.F, Burdi A.R, Eyman C.E. Association between mandibular fractures and site of trauma, dentition and age. Journal of oral surgery, anaesthesia, and hospital dental service 1962; 20: 478–481. PMID: 13955479.
- Huelke D.F. Location of mandibular fractures related to teeth and edentulous regions. Journal of oral surgery, anaesthesia, and hospital dental service1964; 22: 396–405. PMID: 14178798.
- Krimmel M, Reinert S. Mandibular fracture after third molar removal. Journal of Oral Maxillofacial Surgery 2000; 58: 1110–1112. PMID: 11021704.
Medical Journal of Zambia, Vol 50, 3
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.