A Systematic Review on the Cost-Effectiveness of Intra-Articular Injections for Pain Relief in Symptomatic Patients with Osteoarthritis
Alex Lwando
National Health Insurance Management Authority, Lusaka, Zambia.
Brian Chanda Chiluba
School of Health Sciences and School of Natural Sciences, University of Zambia, Lusaka, Zambia.
DOI: https://doi.org/10.55320/mjz.50.2.421
Keywords:systematic review, osteoarthritis, intra-articular injections, ultrasound, cost-effectiveness.
ABSTRACT
Background: This systematic review aimed to assess the quality of published economic evaluations of ultrasound-guided intra-articular injections for symptomatic management of osteoarthritis, explore their scope and diversity, and determine their cost-effectiveness.
Methods: Relevant electronic databases were systematically searched for studies published from January 2009 to June 2019. Keyword searches and Boolean operators were used to retrieve relevant literature. The PICOTS framework was utilized to define key research questions and guide the literature search. Duplicate removal, title and abstract screening were conducted to exclude irrelevant articles. Data from each study were extracted using a standardized form and summarized in an Excel spreadsheet. The SIGN quality appraisal tool for economic evaluations was employed to assess the quality of each study.
Results: The initial database search yielded 238 articles, with 35 duplicates removed. Following title and abstract screening, an additional 198 articles were excluded due to not meeting the inclusion criteria. Full-text manuscripts of the remaining 5 articles were reviewed. Based on the quality appraisal, 4 out of the 5 studies were excluded. One study was not a primary study, one was still ongoing, and two were not economic evaluations. Due to the limited number of included studies, no subgroups were identified.
Conclusions: This study provides evidence that ultrasound-guided intra-articular injections significantly improve clinical outcomes and enhance cost-effectiveness in the management of osteoarthritic joints. However, the scarcity of relevant studies highlights the need for further research to strengthen this finding.
INTRODUCTION
Osteoarthritis (OA) is the most common disease of the joints and ranks among the top five leading causes of disability worldwide.[1] It is characterized by a complex interplay of constitutional, biomechanical, and genetic risk factors, leading to degeneration of joint structures such as cartilage, subchondral bone, and synovium.[2] Individuals affected by OA experience a range of personal, social, and economic consequences. They often endure joint pain, stiffness, and loss of mobility, resulting in difficulties with activities of daily living, reduced autonomy, and a decline in overall quality of life. Moreover, OA imposes substantial financial burdens at both the individual and societal levels.[3,4,5]
The prevalence of OA is alarmingly high, affecting approximately 13.9% of adults aged above 25 years and 33.6% of individuals aged 65 years and older in the United States.[6] This translates to an estimated 52.5 million people, or 22.7% of the population across all age groups, experiencing the burden of OA.[7] In the United Kingdom, nearly 8.5 million individuals suffer from OA of the spine, contributing to an overall economic impact equivalent to 1% of the Gross National Product (GNP) and resulting in 36 million workdays lost due to reduced productivity, amounting to over £3.2 billion.[8] The global cost of OA in countries such as the UK, France, Australia, USA, and Canada accounts for 1-2.5% of the GNP.[9] Beyond the physical implications, OA is associated with an increased prevalence of comorbidities such as obesity and cardiovascular morbidity due to reduced mobility and the use of analgesic medications with potential cardiovascular side effects.[5]
Intra-articular (IA) injections have emerged as an alternative treatment for pain relief in OA. These injections involve the administration of substances such as hyaluronic acid (HA), stem cells, platelet-rich plasma, or corticosteroids directly into the affected joint. IA injections have shown efficacy in providing short-term pain relief and delaying the need for total joint replacement, making them particularly suitable for patients with comorbidities or those for whom NSAIDs are contraindicated or ineffective.[10-11] Furthermore, the use of ultrasound guidance during IA injections has been found to reduce procedural pain, prolong pain-free periods, decrease reinjection frequency, improve joint function, and increase the accuracy of needle placement within the joint space.[12,13,14]
Despite the documented positive effects of intra-articular injections and the growing body of evidence supporting the efficacy of ultrasound-guided procedures, there is a lack of systematic reviews examining the cost-effectiveness of ultrasound-guided intra-articular injections in OA. This gap in the literature highlights the need for a comprehensive evaluation of the economic implications of this treatment approach.
This systematic review aims to fill this research gap by examining the cost-effectiveness of ultrasound-guided intra-articular injections for pain relief in symptomatic patients with osteoarthritis. By systematically reviewing and appraising published economic evaluations, this study seeks to provide valuable insights for physicians, public health officials, policymakers, and other stakeholders involved in the delivery of intra-articular treatments. The review will employ a best evidence synthesis approach, including the identification and appraisal of relevant literature, reporting of results, and a thematic discussion of the cost-effectiveness findings. The outcomes of this review have the potential to inform clinical practice and healthcare decision-making, ultimately improving patient outcomes and socio-economic indicators related to OA management.
In summary, this systematic review aims to address the knowledge gap regarding the cost-effectiveness of ultrasound-guided intra-articular injections for pain relief in symptomatic patients with osteoarthritis. By examining the existing evidence, this study intends to provide valuable insights into the economic implications of this treatment approach, offering guidance to healthcare practitioners and policymakers in optimizing the management of OA and enhancing patient outcomes.
METHODS
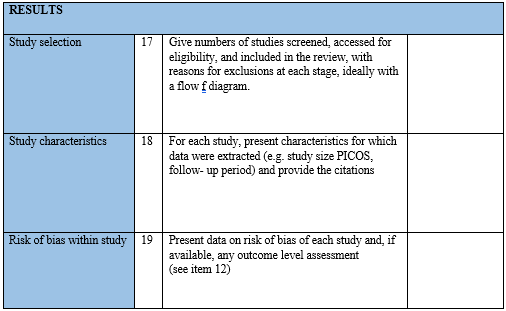
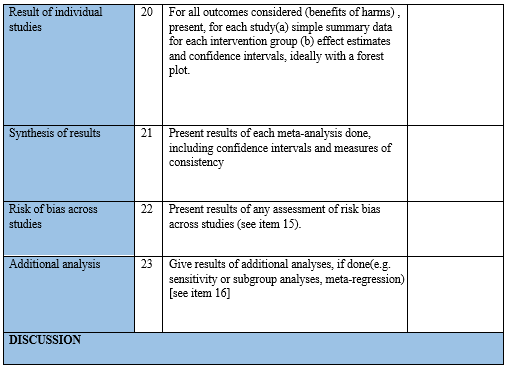
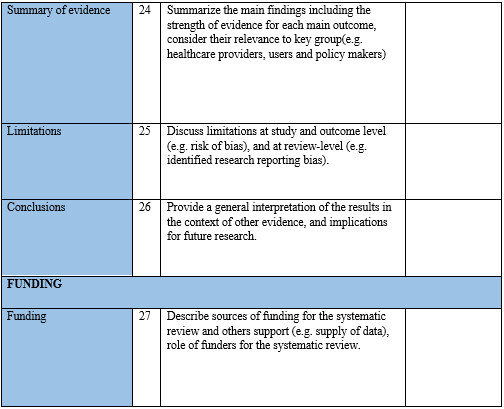
This chapter describes the methods used to retrieve the literature, details on inclusion and exclusion criteria, databases that were searched, and strategies used to search these databases. The chapter concludes with the description of the data extraction and synthesis methods. The methods employed under this section conformed to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) diagram.
Systematic literature review
Computerised search strategies of publications between 2009 and 2019 was developed and implemented across several electronic databases. A combination of keyword searches and Boolean operators was employed to retrieve the most relevant literature. PICOTS (population, intervention, comparator, outcome, time, and setting) was used to define the key questions used in studies and guide literature search.
Database search strategies
Various standard databases in medical and health economic fields were searched for eligible references. Each database was scanned for references for the past 10 years (2009 to 2019). A 10-year margin was applied to studies to maintain relevance to modern day practice of medicine.
Databases searched
Common and relevant databases were searched using relevant keywords and MeSH terms. Databases included PubMed, HINARI and Cochrane Controlled Trials Register. Further, reference mining was conducted to enhance capture of relevant articles.
Data collection
Following electronic database search, records were retrieved and imported to EndNote. Duplicates were initially removed using the EndNote automatic duplicate removal function. Then they were further subjected to manual screening to ensure total removal of duplicates. Title screening was then performed by the researcher. All titles not relevant to the study or its objectives were removed. After title screening, studies were then screened by their abstracts. All studies whose abstracts didn’t fit the inclusion criteria were discarded. Following this, full papers were reviewed in detail for final inclusion. All included full text studies were stored in PDF format for data extraction and quality appraisal.
Data extraction and management
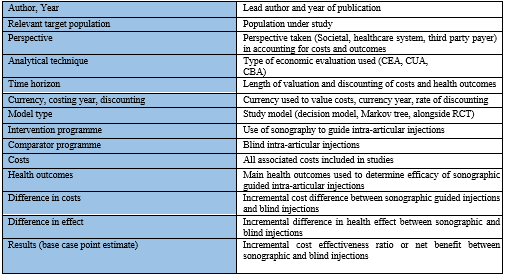
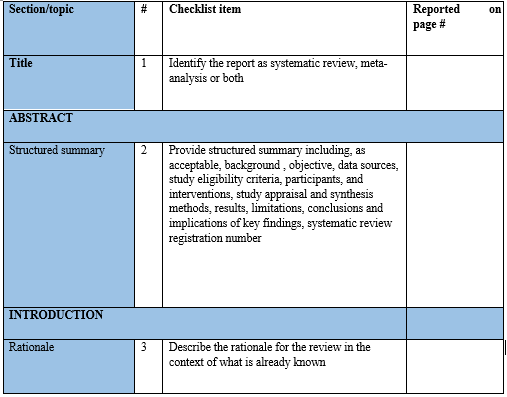
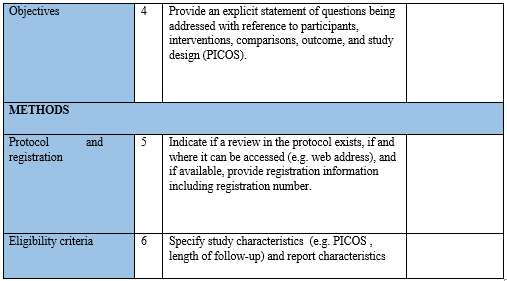
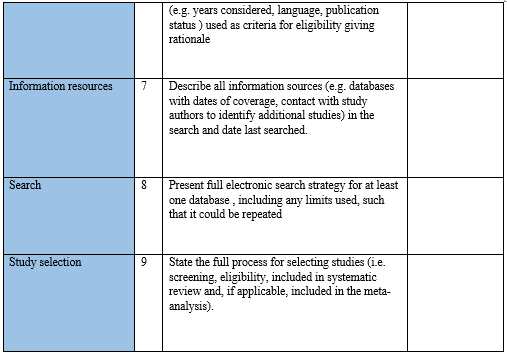
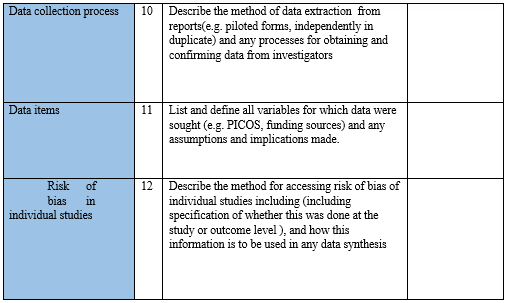
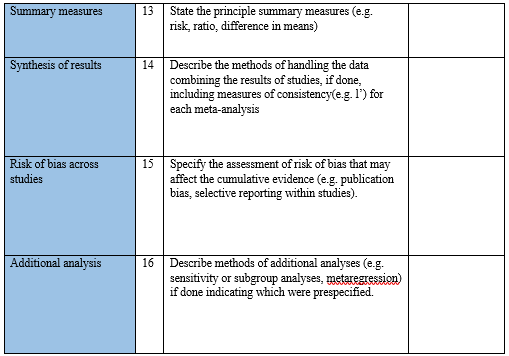
Data were extracted from each study using a standardised form (Table 1) including items related to publication details, study design, setting, participant characteristics, main outcomes, measures, and main findings related to thesis, and summarised in Excel Spreadsheet.
Selection criteria
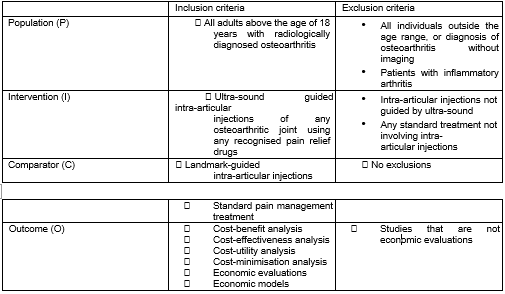
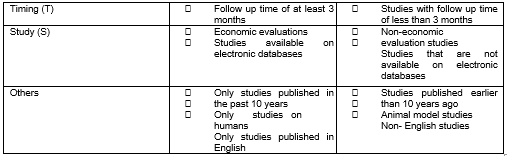
The inclusion criteria for this review were specifically designed to select literature that is relevant to the research objectives and fits within the study design parameters. The review included studies that involved adults aged 18 years and above with radiologically diagnosed osteoarthritis. These studies examined ultrasound-guided intra-articular injections in any osteoarthritic joint using any recognized pain relief drugs, with landmark-guided intra-articular injections as a comparator. The review focused on studies that employed cost-benefit analysis, cost-effectiveness analysis, or cost-utility analysis as the analytical technique. The included studies were required to be available on electronic databases, published in English within the past 10 years (2009-2019), and have conducted economic evaluations. On the other hand, the review excluded studies with participants outside the specified age range or those diagnosed with osteoarthritis without imaging. Studies involving patients with inflammatory arthritis were also excluded. Furthermore, studies that examined intra-articular injections but did not utilize ultrasound guidance were excluded, as were studies that did not use landmark-guided intra-articular injections as a comparator. Studies that did not involve economic evaluations, had a follow-up time of less than 3 months, were not available on electronic databases, focused on animal models, were non-English studies, or were published more than 10 years ago were also excluded.
The PICOTS (Table 2) provides a clear overview of the inclusion and exclusion criteria utilized in the literature search.
The PICOTS table for inclusion/exclusion criteria
Quality appraisal
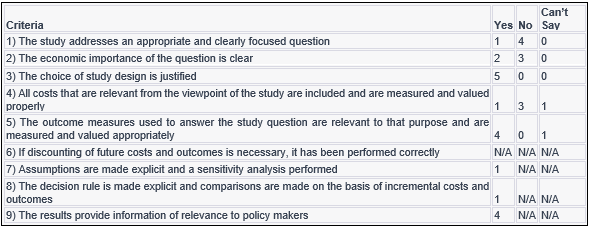
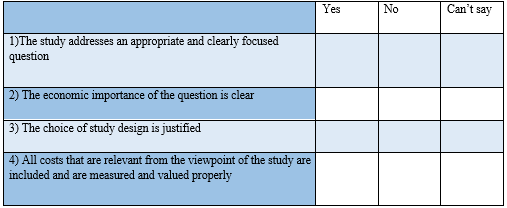
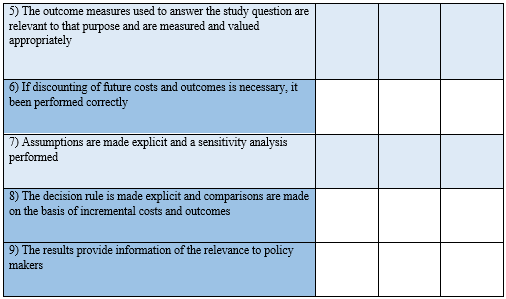
The SIGN quality appraisal tool for economic evaluations was utilized to assess each study included in the analysis. The tool consists of nine close-ended questions that require "yes," "no," or "can't say" responses. The questions address various aspects of the study, such as the appropriateness and clarity of the research question, the economic importance of the question, the justification of the study design, the inclusion and proper measurement and valuation of relevant costs, the relevance and appropriate measurement and valuation of outcome measures, the correct application of discounting if necessary, the explicitness of assumptions and the performance of a sensitivity analysis, the explicitness of the decision rule and the basis for comparing incremental costs and outcomes, and the provision of information relevant to policy makers. The SIGN tool provides guidance on the internal validity of each study by examining aspects such as study design, costing, discounting, and sensitivity analysis. While each question in the tool is relevant, high-quality studies are expected to answer affirmatively to questions 4, 5, and 7.
Literature synthesis
Due to the heterogeneous nature of economic evaluations, the best-evidence synthesis and qualitative approach was used to summarise findings and identify common themes and conclusions. Costs and outcomes were not quantitatively pooled via meta-analysis as outcomes were not comparable across economic evaluations that use different designs, settings, interventions, objectives and perspectives.
RESULTS
This section reports results from the literature search and quality appraisal, and presents the former in a flow diagram. Included economic evaluations are summarised in tabular form.
Search results
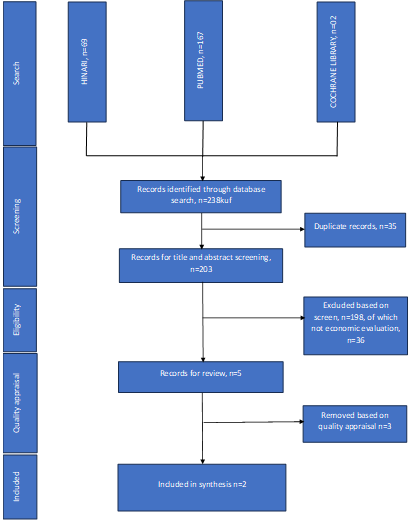
A literature search of peer-reviewed databases yielded 238 articles, with 35 duplicates removed. Following title and abstract screening, 198 articles were excluded as they did not meet the inclusion criteria. Full-text manuscripts of the remaining five articles were retrieved and reviewed. One article addressed osteoarthritis but did not involve ultrasound-guided injections.[15] Berkoff et al.[16] was identified as a non-primary study, and another study did not include an economic evaluation component.[17] The study selection process is depicted in the flow diagram (Figure 1).
RESULTS
A quality appraisal was conducted for five studies using the SIGN checklist[18] to determine their admissibility. Of the five studies, three were deemed inappropriate for the analysis as they were not economic evaluations.[19,20,21] One study was identified as an ongoing study without published results.[22] Full-text manuscripts of these studies were retrieved based on their mention of cost or cost-effectiveness in their abstracts and their focus on ultrasound-guided intra-articular injections in osteoarthritis.
Two studies addressed the economic importance question[23,22] while the remaining three studies did not. The chosen study designs were justified in all five studies. Only one study appropriately included and measured all relevant costs,[23] while the costs for the ongoing study could not be verified due to the lack of published results.[22] The outcome measures used in the four studies included in the appraisal were relevant and appropriately measured and valued.[19,20,21,22] However, there was insufficient information regarding the measurement and valuation of outcomes in the fifth study.[22]
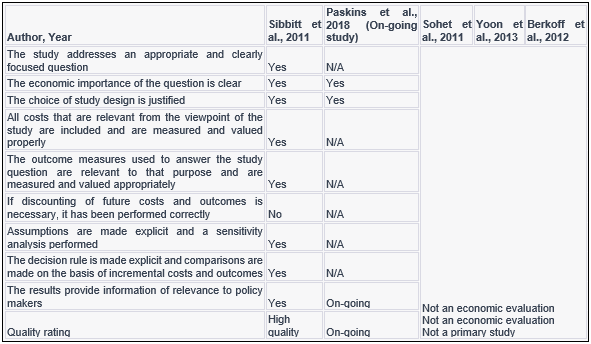
Discounting of future costs and outcomes was not necessary in any of the studies, as one study was conducted alongside a clinical trial,[23] and the protocol of the ongoing study indicated that economic evaluations would be done alongside a clinical trial.[22] None of the studies performed a sensitivity analysis, and only one study provided explicit decision rules and made comparisons based on incremental costs and outcomes.[23] Furthermore, four studies provided results relevant to policy makers.[19,20,21,22] However, only one study presented health economic results, while the other three studies focused on clinical efficacy results for intra-articular injections in pain management of osteoarthritic joints.[19,20,21,23] Table 3 shows the results of the SIGN checklist, and table 4 summarises the detailed results of the SIGN checklist.
Characteristics of included economic evaluations
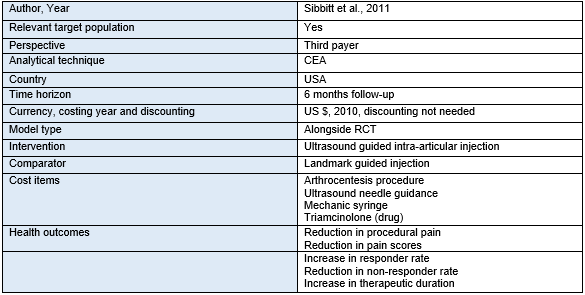
Based on the quality appraisal, four of the five studies were excluded[19,20,21,22] One study was not a primary study,[22] one study was still ongoing[23] and two studies were not economic evaluations.[21,19] Due to the small number of included studies, no subgroups were identified. The only study that met the inclusion criteria was a randomized controlled trial conducted by Sibbitt et al.[23] This study, conducted in the USA, included 92 participants with knee osteoarthritis who were equally randomized to receive landmark-guided or ultrasound-guided intra-articular injections. The study included individuals with radiographically diagnosed osteoarthritis ranging from Brandt Grade 1 to 3, persistent pain requiring injection clinic referral, significant pain with a visual analogue scale (VAS) score of 5 cm or greater, pain limiting exercise and unresponsive to analgesics, and patients recommended for intra-articular injections by their attending physicians.
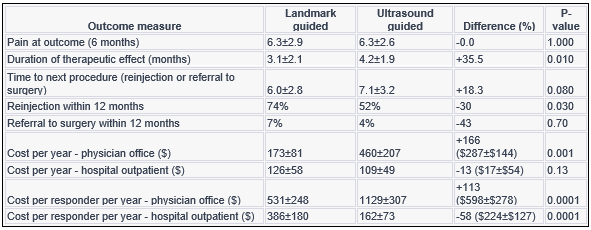
The outcome measures in this study were pain reduction and cost-effectiveness of ultrasound-guided intra-articular injections using corticosteroids as the treatment drug. Pain was assessed using the standardized 0- to 10-cm VAS, with significant pain defined as a VAS score of 5 cm or greater. Pain was evaluated at three points: baseline, procedural (during needle insertion), and injection (during treatment drug administration). The primary outcome was the pain score at 2 weeks, and the secondary outcome was the pain score at 6 months. Responders were defined as individuals with a VAS score less than 2 cm, and non-responders had a VAS score of 2 cm or greater. The duration of therapeutic response was measured in months, and the time to the next injection or referral for surgery was determined based on patient interviews and chart review at 12 months.
The study found that landmark-guided intra-articular corticosteroid injections reduced pain by 69% at 2 weeks. The duration of therapeutic effect was approximately 3.1 months, and the time to reinjection was 6.0 months. Ultrasound-guided injections showed minimal differences in pre-procedure pain compared to landmark-guided injections but were significantly less painful during the procedure and injection. At the primary outcome, ultrasound-guided intra-articular injections demonstrated superior results compared to landmark-guided injections, with lower pain scores, higher responder rates, and longer duration of therapeutic effect and time to the next procedure. Procedural costs for hospital outpatient care were modestly reduced, leading to lower costs per patient per year and costs per responder per year. Ultrasound guidance improved short- and long-term outcomes without increasing the overall costs.
The cost-effectiveness of ultrasound-guided injections was based on balancing the increased costs of ultrasound guidance with the reduced use of other healthcare resources such as re-injections or referrals for surgery. Ultrasound-guided injections were found to be cost-effective, as they provided better outcomes with lower costs in a hospital outpatient setting. The inclusion of ultrasound guidance in hospital-based care reduced costs per patient per year and costs per responder per year compared to landmark-guided injections.
Study limitations
1. The study was limited to a hospital outpatient setting, and the conclusions may not be applicable to private physician offices due to differences in access, medical care, and reimbursement rates. To determine the cost-effectiveness of ultrasound guidance in a physician office, real data from private physician offices are needed.
2. The analysis did not include certain expenses such as the acquisition and maintenance of ultrasound machines, image storage, ultrasound supplies, and increased procedure time. These costs primarily affect the proceduralist/ institution's profit or loss and are not directly borne by third parties.
3. The study truncated the therapeutic duration and time to the next injection, which could underestimate the cost-effectiveness estimate. True cost-effectiveness may be even more favourable for ultrasound guidance than the study findings.
4. The cost-effectiveness of different forms of intra-articular injections may vary due to differences in the cost of the injectable drugs. For example, hyaluronic injections are more expensive than corticosteroid injections. Therefore, the increased responder rate and prolonged therapeutic response associated with ultrasound guidance could result in greater cost savings and cost-effectiveness, particularly for more expensive injections.
5. Reimbursement rates vary between years and countries, leading to heterogeneity in cost-effectiveness estimates.
The HIP Injection Trial (HIT) is an ongoing study in the UK that is worth mentioning.[24] It is a pragmatic, three-parallel group, single-blind, superiority randomized controlled trial focusing on patients with moderate-to-severe hip osteoarthritis. The study aims to enrol a total of 204 patients within a 29-month enrolment period. Using a societal perspective and cost-utility analysis, the study will assess the cost-effectiveness of ultrasound-guided intra-articular injections for pain management in osteoarthritis.[24] The trial protocol and its inclusion in this dissertation are important due to the limited availability of relevant studies addressing the cost-effectiveness of these interventions.
DISCUSSION
Osteoarthritis has many personal, social, economic and public health effects on affected individuals and the society as a whole. Individuals affected by the disease suffer various consequences including loss of income, while society incurs costs of reduced or loss of productivity of patients, increased healthcare use, cost of caregivers, and disability living allowances.[25,26,27] The pathophysiological processes underlying this disease are poorly understood, hence no established disease-modifying treatment to date exists, and the management of OA still relies on pharmacologic and non-pharmacologic methods aimed at relieving symptoms of pain and preserving joint function.[28] The most commonly used, efficacious and safest pharmacological method are intra-articular injections, delivered either by landmark anatomical guidance or with the aid of ultrasound.
Owing to this, this thesis set out to systematically review and appraise the quality of published economic evaluations of ultrasound guided intra-articular injections for symptomatic management of osteoarthritis, describe their scope and diversity, and discuss and determine their cost-effectiveness. The present research is the first study to examine outcome and cost-effectiveness of ultrasound guidance for injection of osteoarthritis of any affected joint with potential relevance for society, third-party payer, policy-makers, the clinician and the design of future clinical trials. This systematic review considered recent relevant research to answer the study objectives. From 238 studies found on electronic databases, full-text manuscripts were retrieved for 5 studies, and only 1 study was found to be relevant. This study had low to very low risk of bias, describing cost-effectiveness of ultrasound guided intra-articular injections in the symptomatic management of knee osteoarthritis. The study demonstrated cost-effectiveness of using ultrasound to guide intra-articular injections. The study showed that intra-articular injections of the osteoarthritic knee performed with ultrasound guidance can significantly and meaningfully improve outcomes and enhance cost-effectiveness.[29]
Whereas this thesis notes many studies which have considered efficacy of different types of pain relief drugs used in intra-articular injections of osteoarthritic joints, the topic of cost-effectiveness with regards ultrasound guided injections has rarely been studied. Therefore, the main limitation to this review was the lack of relevant cost-effectiveness studies. The thesis findings only provide evidence for cost-effectiveness of ultrasound-guided intra-articular injections from one study.[29] The strength of this review lies in the quality of this study, giving some confidence in the conclusion around the cost-effectiveness of ultrasound guided intra-articular injections. This review did not find any similar reviews to compare findings with, further emphasizing the lack of cost-effectiveness studies regarding the topic under study, despite the massive public health effect and major costs associated with the treatment of osteoarthritis.
Implications and transferability of findings
This study examines the cost-effectiveness of ultrasound-guided intra-articular injections in osteoarthritis pain management. The findings have implications for public health agencies, health economists, healthcare professionals, and individuals. Ultrasound guidance improves clinical outcomes, reduces procedural pain, and saves costs. However, the limited number of studies included in this review restricts the transferability of the findings. Further research and economic evaluations are necessary to enhance confidence in the results.
Limitations of this research
A possibility exists that some studies may not have been captured in the search strategy and, therefore, not included in the review. Serious attempts were made to access Embase and Medline, but due to restricted access to these databases (no library accessible to me had open access to these databases), content was not accessed. However, owing to the repetitiveness of studies looking at intra-articular injections and osteoarthritis on accessible databases, and complete access to all studies identified through reference mining, it is highly unlikely that any relevant study was missed. Another possibility exists that some studies could have been missed during title and abstract screening. This, too, is a remote chance looking at the small number of identified studies and the vigorous screening conducted by the researcher.
The major limitation of this review was the small number of relevant studies to review. This could be due to a lack of research interest or due to the relative novelty of ultrasound use in everyday musculoskeletal clinical practice,[30] despite massive evidence supporting its relevance and superiority in accessing joint spaces.[31,32,33,34,35,36,37,38,39,40] Further research is needed to determine the reasons behind the scarcity of such literature.
CONCLUSION
The present study has provided evidence that intra-articular injections of osteoarthritic joints performed under the guidance of ultrasound significantly improve clinical outcomes and enhance cost-effectiveness. There is clear need for more studies to be done to cement this finding as very few relevant studies on the subject matter currently exist.
RECOMMENDATIONS
There is no doubt that sonography and diagnostic imaging are becoming integral parts of modern medicine, and thus outcome and cost-effectiveness studies are needed to justify this practice transformation.[41] The present study is the first to review cost-effectiveness of ultrasound guidance for intra-articular injections in osteoarthritis of any joint. This study recommends that future research be conducted to address the cost-effectiveness of ultrasound image guidance in intra-articular injections with regards pain management in osteoarthritis. Available relevant literature is too little to offer any significant guidance to policy makers, clinicians, payers and patients.
REFERENCES
- Murray CJ, Lopez AD. Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study. The Lancet. 1997;349(9063):1436-42.
- Salmon JH, Rat AC, Sellam J, et al. Economic impact of lower-limb osteoarthritis worldwide: a systematic review of cost-of-illness studies. Osteoarthritis and Cartilage. 2016;24(9):1500-8.
- Chen A, Gupte C, Akhtar K, et al. The global economic cost of osteoarthritis: how the UK compares. Arthritis. 2012;2012:698709.
- CDC (Centers for Disease Control and Prevention). Prevalence of doctor-diagnosed arthritis and arthritis-attributable activity limitation — United States, 2010-2012. Morbidity and Mortality Weekly Report. 2013;62(44):869-73.
- Salmon JH, Rat AC, Ravaud P, et al. Economic impact of lower-limb osteoarthritis: a systematic review of cost-of-illness studies. Osteoarthritis and Cartilage. 2017;25(9):1407-17.
- Lawrence RC, Felson DT, Helmick CG, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States: Part II. Arthritis & Rheumatism. 2008;58(1):26-35.
- CDC (Centers for Disease Control and Prevention). Prevalence of doctor-diagnosed arthritis and arthritis-attributable activity limitation — United States, 2010-2012. Morbidity and Mortality Weekly Report. 2013;62(44):869-73.
- Arthritis in the UK. Information Centre, Department for Work and Pensions. Arthritis and disability: research evidence No. 2. 2008.
- March LM, Bachmeier CJ. Economics of osteoarthritis: a global perspective. Baillière's Clinical Rheumatology. 1997;11(4):817-34.
- Cooper C, Rannou F, Richette P, et al. Use of intra-articular hyaluronic acid in the management of knee osteoarthritis in clinical practice. Arthritis Care & Research. 2017;69(9):1287-96.
- Delbarre A, Amor B, Bardoulat I, et al. Comparison of ultrasound-guided versus landmark-guided intra-articular corticosteroid injections in patients with knee osteoarthritis. Joint Bone Spine. 2017;84(6):677-81.
- Sibbitt WL Jr, Kettwich LG, Band PA, et al. Does ultrasound guidance improve the outcomes of arthrocentesis and corticosteroid injection of the knee? Scand J Rheumatol. 2011;40(1):66-72.
- Matzkin EG, Suslavich KS, Curry EJ. Can local corticosteroid injection still be considered first-line treatment for rotator cuff disease?: A systematic review and meta-analysis. The American Journal of Orthopedics. 2017;46(1):E1-E9.
- Jones T, Ostergaard M, Conaghan PG, et al. Ultrasonographic assessment of joint inflammation in rheumatoid arthritis: results of an interobserver reliability study of the EULAR-OMERACT ultrasound task force. Ann Rheum Dis. 2005; 64(2):179-84. doi: 10.1136/ard.2004.022277.
- Sohet A, Ye X, Rannou F, Marty M, Taccoen A, Vanneste D, et al. Injection therapy for osteoarthritis of the knee: a comparative study of hyaluronic acid and corticosteroid. Osteoarthritis Cartilage. 2011;19(S1):S171-2.
- Berkoff DJ, Miller LE, Block JE. Clinical utility of ultrasound guidance for intra-articular knee injections: A review. Clin Interv Aging. 2012;7:89.
- Yoon HS, Kim SJ, Yoon YC, Huh YH, Kim HJ. Comparison of intraarticular injections of hyaluronic acid and corticosteroid in osteoarthritic knee joints. Scottish Intercollegiate Guidelines Network. SIGN 50: A Guideline Developer's Handbook. Edinburgh: SIGN; 2015.
- Sohet A, Ye X, Rannou F, Marty M, Taccoen A, Vanneste D, et al. Injection therapy for osteoarthritis of the knee: a comparative study of hyaluronic acid and corticosteroid. Osteoarthritis Cartilage. 2011;19(S1):S171-2.
- Yoon HS, Kim SJ, Yoon YC, Huh YH, Kim HJ. Comparison of intraarticular injections of hyaluronic acid and corticosteroid in osteoarthritic knee joints. Ann Rehabil Med , Volume 43(2); 2019.
- Berkoff DJ, Miller LE, Block JE. Clinical utility of ultrasound guidance for intra-articular knee injections: A review. Clin Interv Aging. 2012;7:89.
- Paskins Z, Unwin J, et al. Intra-articular steroid injections in hip osteoarthritis: exploratory study with randomised controlled trial phase. Rheumatology Advances in Practice. 2018;2(Suppl_1): i9.
- Sibbitt WL, Kettwich LG, Band PA, et al. Does ultrasound guidance improve the outcomes of arthrocentesis and corticosteroid injection of the knee? Scand J Rheumatol. 2011;40(1):66-72.
- Paskins Z, Sanders T, Croft PR, Hassell AB. The HIP Injection Trial: A randomised controlled trial of ultrasound-guided intra-articular corticosteroid injection for hip osteoarthritis. Rheumatology. 2018;57(Supplement_3):key075.126. doi:10.1093/rheumatology/key075.126
- Chen A, Gupte C, Akhtar K, Smith P, Cobb J. The Global Economic Cost of Osteoarthritis: How the UK Compares. Arthritis. 2012; 2012:698709. doi:10.1155/2012/698709.
- Salmon JH, Rat AC, Sellam J, et al. Economic impact of lower-limb osteoarthritis worldwide: a systematic review of cost-of-illness studies. Osteoarthritis Cartilage. 2016;24(9):1500-1508. doi:10.1016/j.joca.2016.05.005.
- UK DLA. Disability Living Allowance: Annual Report 2007/2008. https://www.gov.uk/government/collections/disability-living-allowance-annual-report. Published 2007. Accessed July 10, 2023.
- Cooper C, Rannou F, Richette P, et al. Use of Intraarticular Hyaluronic Acid in the Management of Knee Osteoarthritis in Clinical Practice. Arthritis Care Res (Hoboken). 2017;69(9):1287-1296. doi:10.1002/acr.23285.
- Sibbitt WL Jr, Peisajovich A, Michael AA, et al. Does sonographic needle guidance affect the clinical outcome of intraarticular injections? J Rheumatol. 2011;38(5):976-982. doi:10.3899/jrheum.100981.
- Kane D, Balint PV, Sturrock RD. Ultrasonography is superior to clinical examination in the detection and localization of knee joint effusion in rheumatoid arthritis. J Rheumatol. 2003;30(5):966-971.
- Delaunoy JP, Marmo E, Bozonnat MC, et al. Comparison of clinical examination, ultrasound, and radiography in assessing inflammatory and destructive changes in fingers and toes of patients with rheumatoid arthritis. Radiology. 2003;229(2):562-570. doi:10.1148/radiol.2291020329.
- Balint PV, Kane D, Wilson H, McInnes IB, Sturrock RD. Ultrasonography of entheseal insertions in the lower limb in spondyloarthropathy. Ann Rheum Dis. 2002;61(10):905-910. doi:10.1136/ard.61.10.905.
- Qvistgaard E, Rogind H, Torp-Pedersen S, Terslev L, Danneskiold-Samsøe B, Bliddal H. Quantitative ultrasonography in rheumatoid arthritis: evaluation of inflammation by Doppler technique. Ann Rheum Dis. 2001;60(7):690-693. doi:10.1136/ard.60.7.690.
- Pendleton A, Millner P, Gilmore R, Scott O, Barr A. Bone bruising detected by magnetic resonance imaging following lateral ankle sprains. Foot Ankle Int. 2008;29(7):671-676. doi:10.3113/FAI.2008.0671.
- Raza K, Filer A. The therapeutic window of opportunity in rheumatoid arthritis: does it ever close? Ann Rheum Dis. 2006;65 Suppl 3:iii27-iii32. doi:10.1136/ard.2006.059909.
- Eustace JA, Brophy DP, Gibney RP, Bresnihan B, FitzGerald O. Comparison of the accuracy of steroid placement with clinical outcome in patients with shoulder symptoms. Ann Rheum Dis. 1997;56(1):59-63. doi:10.1136/ard.56.1.59.
- Naredo E, Moller I, Moragues C, et al. Interobserver reliability in musculoskeletal ultrasonography: results from a "Teach the Teachers" rheumatologist course. Ann Rheum Dis. 2006;65(1):14-19. doi:10.1136/ard.2005.038349.
- Sibbitt WL Jr, Kettwich LG, Band PA, et al. Does sonographic needle guidance affect the clinical outcome of intraarticular injections? J Rheumatol. 2009;36(9):1892-1902. doi:10.3899/jrheum.090063.
- Naredo E, Moller I, de Miguel E, et al. High prevalence of ultrasonographic synovitis and enthesopathy in patients with psoriasis without psoriatic arthritis: a prospective case-control study. Rheumatology (Oxford). 2011;50(10):1838-1848. doi:10.1093/rheumatology/ker178.
- Parker L, Nazarian LN, Carrino JA, et al. Musculoskeletal imaging: medicolegal considerations. Radiology. 2008;246(3):675-682. doi:10.1148/radiol.2463062184.
APPENDICES
Appendix 1: Search strategies
PUBMED Search Strategy
Search: Cost-effectiveness AND intra-articular injections AND ultrasound-guided OR sonograph* guided AND osteoarthritis [MeSH Major Topic].
MeSH terms:
Cost-benefit analysis; injections; intra-articular; osteoarthritis; ultrasonography; ultrasonics.
Filters: Publication date from 01/01/2009 to 20/06/2019; Humans only; English only.
HINARI Search strategy
1. Osteoarthritis
2. Cost-effectiveness
3. Intra-articular injections
4. Ultrasound guided injections OR
5. Ultra-sound guided injections OR
6. Ultrasound-guided injections OR
7. Ultra-sound-guided injections
8. Sonographic guided injections OR
9. Sonographic-guided injections
10. 1 AND 2 AND 3 AND 4 OR 5 OR 6 OR 7 AND 8 OR 9
HINARI limiters: Boolean/Phrase search; English language only; January 2009 to June 2019
Human only.
Cochrane Library search:
1. Cost-effectiveness AND
2. Ultrasound guided OR sonographic guided AND
3. Intra-articular injections AND
4. Osteoarthritis
Limits: trials; humans; 01/01/2009 to 20/06/2019
Medical Journal of Zambia, Vol 50, 2
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.