Implementation of Enhanced Recovery after Surgery at a General hospital in Zambia
Sergiy Karachentsev
Roan Antelope General Hospital, PO Box 90297, Luanshya, Zambia
Phone: +260212515010
Mobile: +260979275679
Fax: +260212671151
Correspondence: sergek69@yahoo.co.uk
DOI: https://doi.org/10.55320/mjz.50.2.419
Keywords:Enhanced Recovery after Surgery, general surgery
ABSTRACT
Background: Enhanced recovery after surgery (ERAS), with its aim of reducing operative stress and accelerating rehabilitation, became a standard perioperative care in multiple surgical specialties in developed world. However, little is known about the implementation of the fast-track pathways in a low-resource environment. The objective of the study was to describe our experience and share lessons obtained in using ERAS protocol in general surgery patients.
Methods: In this descriptive study, all consecutive patients with no age restrictions undergoing elective and urgent abdominal surgery were assessed for inclusion in ERAS program. A retrospective analysis encompasses 98 patients aged two weeks to 87 years with male to female ratio of 2.3:1. Outcomes were functional recovery, postoperative complications, and length of hospital stay.
Results: All elements of ERAS protocol including minimal incision length laparotomy and accelerated postoperative care were used; however, certain components were modified depending on the availability of the resources and patient’s condition. Postoperative period complicated in 17.4% of cases, seven patients (7.4%) died after urgent operations, and no mortality was recorded after elective procedures. Median length of stay was 4.0 days. Local and systemic septic complications, paralytic ileus and performing of the stoma reversal procedure during the same hospital stay were reasons for delayed discharge.
Conclusion: This study indicates that employment of ERAS program for general surgery population at a second level hospital is feasible and safe. Further larger-scale studies are needed.
INTRODUCTION
Enhanced recovery after surgery (ERAS) is a multidisciplinary program designed to reduce surgical stress and improve recovery of organ function through perioperative optimisation of patient treatment.[1] Originally created for elective colorectal surgery, this protocol is well established now for many specialized surgical populations.[2-4] The program focuses on providing multimodal analgesia, goal-directed fluid therapy, minimally invasive techniques, thromboembolic prophylaxis, and early mobilisation.[5-6] The benefits, safety, and cost-effectiveness of fast-track pathways (FTP) were validated in multiple studies including randomised controlled trials.[7-9] However, in spite of its many successes, ERAS still has a number of issues and implementation of accelerated stay programs remains challenging.[1-10] The reasons are manifold including internal barriers (lack of awareness of current evidence-based literature, disagreement with current findings or belief that a particular hospital cannot support fast-track surgery protocols, etc.) and external barriers (insufficient number of support staff, lack of expertise in FTPs, and financial considerations).[2-11] This is particularly true for hospitals operating in low-resource environment having a reduced surgical workforce density and an urgent need to increase access to safe and timely surgical care.[12] The aims of research were to assess the feasibility of ERAS program for patients with elective and urgent abdominal conditions at our setting and share lessons learned in this process.
MATERIALS AND METHODS
ERAS was systematically introduced for general surgery at Roan General Hospital in March 2021. This is a second level referral hospital in Zambia having a capacity of 164 beds and operating as the main medical centre in the area with the population of around 200,000 people. This observational study included patients operated until September 2022. Participants were identified through operative case logs, perioperative variables were obtained by retrospective review of medical records. All consecutive patients operated for elective and urgent abdominal conditions were assessed to enter the study, no age restrictions applied.
The study was conducted according to the ethical principles for medical research (Declaration of Helsinki).[13] Permission to conduct the study was sought from the Hospital Ethical Committee and confidentiality was maintained in the process of data collection. Informed consent was obtained from all individual participants included in the study.
Patient characteristics reported included age, sex, medical and social history, comorbidities. Fitness of patients to surgery was assessed using American Society of Anaesthesiologists Physical Status classification system (ASA score).[14] Patients were followed up by out-patient reviews during 30-days period after discharge.
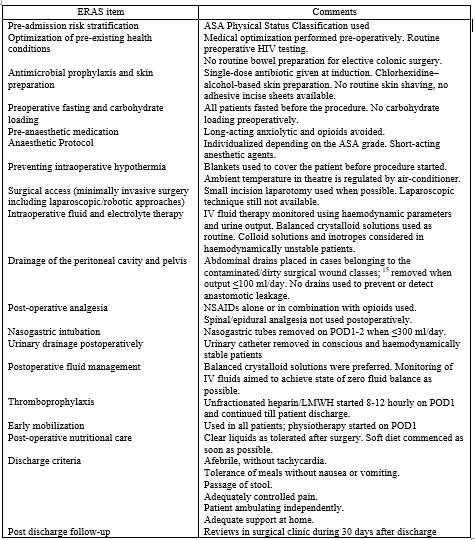
In the study participants, corresponding components of ERAS were used in accordance with interdisciplinary consensus review[5] starting from preoperative assessment and including final recommendations to the patients at the time of discharge from clinical care (Table 1). Preoperative management of patients depended on their clinical needs. Evaluation of patients scheduled for an elective procedure comprised of revealing and correcting coexistent medical morbidity, while management of patients admitted as an urgent case focused on immediate optimisation of their conditions. The plan for the intervention was discussed in details with anaesthesiologist and we sought consensus in every case. When indicated, local anaesthesia was given by infiltration of subcutaneous tissues and muscles of anterior abdominal wall at the site of incision with lignocaine 0.5% 200-250 mg.
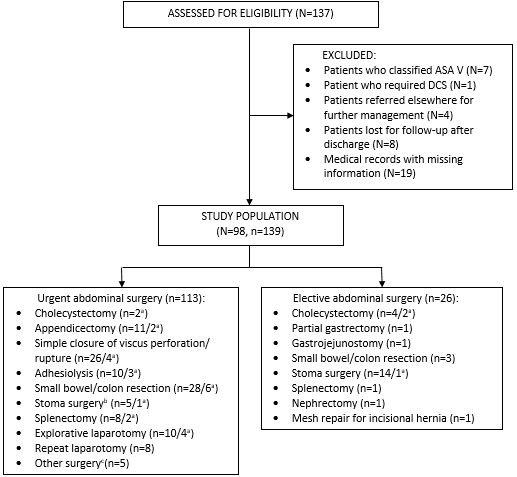
In selective group of the patients, we practiced a mini-laparotomy surgical approach (MLS) to abdominal cavity (Figure). Mini-laparotomy was defined as a skin incision of less than or equal to 12 cm in length performed by using traditional surgical techniques and instruments. We considered small-incision laparotomy in clinical situations when preoperatively we were able to establish the diagnosis and locus of intra-abdominal pathology. A decision to use mini-laparotomy was taken after critical assessment of possible risks and expected benefits for every particular patient. We did not attempt small incisions in obese patients with body mass index of above 28, in cases of generalised peritonitis, abdominal malignancy and for repeat laparotomy procedures.
N, number of patients; n, number of operations; ASA, American Society of Anaesthesiologists;
DCS, damage control surgery
a performed using small-incision laparotomy approach
b defined as closure or creation of an end/diverting colostomy or ileostomy
c included suturing of the liver/kidney, inguinal herniorrhaphy
Except those caused intestinal obstruction
b Included splenomegaly, hydronephrosis, pelvic inflammatory disease, post-operative peritonitis.
c 1 patient had 4 operations, 3 patients had 3 operations and 11 patients had 2 operations as separate cases, these 15 patients therefore represent 35 operations.
After the operation, patients were managed at Intensive Care Unit or surgical ward depending on their clinical condition. Thromboembolic prophylaxis included early mobilisation and administration of unfractionated or low-molecular weight heparin starting from 6-12 hours postoperatively. We mobilise the patients with the help of specially trained hospital staff. Mobilisation started on postoperative day (POD) 1 with in-bed exercises and chest physiotherapy, and continued thereafter with encouraging ambulation as tolerated.
The primary outcomes were: functional recovery, intra- and postoperative complications according to Clavien-Dindo (C-D) classification[16] and hospital length of stay (LOS). Functional recovery was assessed by a resumption of oral intake, return of bowel function, and sufficient mobilisation. Morbidity was defined as per operations when they represent a separate case; a patient could undergo several procedures, both urgent and elective (Table 2) at different stages of surgical management with intervals ranging from seven days to eleven months. For example, reversal of the stoma considered as a different case from the index procedure even if these two operations performed during the same hospital admission (as it was done in three of our patients). In cases of re-operations performed in the immediate postoperative period, complication rates have been adjusted so that they only can be attributed as a result to the last of a patient’s operations. The similar calculation demonstrated by Timan et al.[17] in a study on emergency surgery from Sweden and suggested in a review report on the global surgery metrics[18] in order to avoid distortion of morbidity data. Postoperative mortality was categorised according to the Safe Surgery Saves Lives initiative of WHO’s Patient Safety Programme[19] as death following surgery and before discharge from hospital or within 30 days of surgery, whichever is sooner, expressed as percentage. LOS was counted from the day of surgery until the day of discharge. The discharge criteria were clearly outlined and standardised (Table 1); the pillars for the decision-making included the optimal pain control, appropriate bowel function and adequate care support at home. If any of these factors seemed questionable, the patients remained in the hospital until the safe discharge is guaranteed. Readmissions were documented from the day of discharge until 30 days postoperatively.
We used descriptive statistics to report data obtained. Due to skew distribution of the variables, continuous parameters were expressed as median and ranges. Categorical data were presented as absolute figures and percentages.
RESULTS
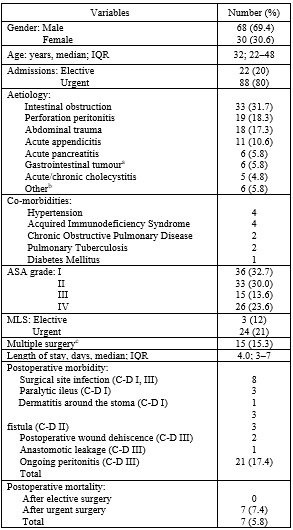
A total of 98 patients aged two weeks to eighty-seven years with male to female ratio 2.3:1 met the inclusion criteria. Demographics and clinical variables of the population are presented in Table 2. As our patients were generally young, medical comorbidities were uncommon (N=9, 9.2%). Because of this, 63% of patients were classified as ASA scores I-II. However, one third of emergency admissions were in complicated conditions of sepsis or/and shock. As a result, a noticeable proportion of the participants were classified as ASA score IV (Table 2).
Operations performed are depicted in the Figure. As a surgical approach, small-incision laparotomy with the median length of 10.5 cm (range 6-12 cm) was used in 27 operations performed in 26 patients. Incisions used were midline (upper n=9, median n=6, and lower n=6), oblique in right (n=3) and left (n=1) hypochondrium, in right (n=1) and left (n=1) iliac fossae. In four cases, MLS was converted to a standard laparotomy incision due to technical difficulties in intraabdominal assessment and manipulation.
We did not encounter any life-threatening intraoperative events, and eight of the patients required blood transfusion during and/or immediately after the procedure. Post-operative complications occurred in 21 patients (17.4%) (Table 2), and most of them (N=17) were recognized during the stay in the hospital. Four patients were re-admitted with complications developed within 30 days after discharge: post-operative wound infection (N=1), high-output colostomy (N=1), both managed medically, and adhesive intestinal obstruction (N=2) which required laparotomy and adhesiolysis in one patient and responded to conservative treatment in the other. Seven patients died after surgery, all deaths occurred after urgent procedures. The causes of in-hospital death recorded were as follows: anastomotic leakage with ongoing peritonitis, sepsis and multiple organ failure (N=1), septic shock without leakage (N=2), non-correctable hypotension and respiratory failure in medically compromised patients (N=2), acute renal failure (N=1). One patient died on day 4 after uncomplicated adhesiolysis procedure performed for intestinal obstruction, and the cause of death remains unknown, as autopsy was not performed. LOS for survived patients ranged from 1 to 47 days, with median of 4.0 days.
The reasons for prolonged stay in the hospital were: septic complications of the post-operative wound and abdominal cavity, paralytic ileus and performing of the stoma reversal procedure during the same admission.
DISCUSSION
The study describes our experience in employing ERAS methodology at a second level surgical hospital. Among the different steps of the implementation process described, [20] we were particularly interested in two principal aspects, namely 1) fidelity, which shows how the innovation corresponds to the originally designed protocol, and 2) adaptation, which refers to modifications made to the initial program during performance. In other words, we aimed to investigate whether it is possible to reproduce the original protocol of ERAS for general surgery population managed in a resource-scarce setting, and if we could prioritize certain items of the FTP and omit the others with the hope for the better outcome in a particular case.
It is well-known that components of the ERAS pathway positively affect all elements of preoperative investigation, decision-making process, intraoperative management and postoperative care.[5-6] Some alterations to perioperative management standards are minimal or not to be changed like, for example, antibiotic- or thromboprophylaxis,[7] and this alleviates the implementation of the FTP into everyday clinical practice. Other changes require more determined attempts, for instance, reducing pre-operative fasting, early postoperative nutrition and restricted use of drains,[21] and need to be encouraged and controlled. Due to fast development of the medical science, industry and operative technique in the recent decades, mini-invasive procedures became an integral part of surgical practice.[22-23] These novel techniques include not only, and should not be limited by, laparoscopic and robotic procedures.[24] At our hospital, we practice MLS in elective and urgent abdominal surgery. Naturally, employment of mini-laparotomy requires sufficient level of surgical competence and this technique has its contraindications, disadvantages and challenges.[25] However, this component of ERAS should not be eliminated in resource-constrained environment, in absence of modern mini-invasive surgical equipment.[26-27] Clinical benefits of minimal approach for the patients have already described in the literature.[11-25] What is particularly important from the patient’s perspective, mini-invasive procedures make a vital contribution to positive effects of ERAS program[1-28] and our humble experience confirms this.
With this in mind, there is a risk that mini-invasive procedures can be considered as the solely decisive factor in improving morbidity in surgery bypassing other elements of the ERAS protocol.[7,24,27] It is therefore crucial to realize that clinical success of accelerated stay program depends first of all on the quality of multidisciplinary collaboration between patient and all care providers involved,[10] and different components of the FTP are in fact equally valuable for faster return to baseline physiological function. According to Malik et al.,[4] the applied perioperative management interventions can have a synergic effect on shortening the recovery time. Similarly, Wijk with colleagues[2] in an international multicentre study of more than 2000 patients made a conclusion that it is the combination of all the different elements of ERAS protocol that makes an effective regimen in improved outcomes after surgery. On the other hand, because of the variety of disciplines in which ERAS protocols are used, individuality of the patient, their clinical condition and the type of procedure being performed should also be factors in whether FTP is utilized. Some researchers[1-29] do not recommend use of enhanced recovery protocol in emergent abdominal procedures for obstruction, perforation and ischaemia. Similarly, others,[21-30] while acknowledging the benefits of accelerated stay program, mentioned certain clinical issues in emergency surgery that are not easily amenable to ERAS principles. Indeed, in patients presented in acute surgical condition, preoperative counselling and education, called otherwise prehabilitation,[31] is usually limited or impossible because of lack of time. Besides, use of FTP in emergency setting may face some challenges postoperatively. Patients undergoing major abdominal procedures may require a period of prolonged ventilation and circulation supports which would limit early mobilisation, early removal of drains and tubes and early enteral nutrition. It was opposed by Hajibandeh et al.[8] and Sethi et al.[32] indicating that most components of ERAS pathways can be applicable and appropriate in acute general surgery population. Likewise, in a review article, Bugada and co-authors[28] suggested that as emergency operations carry a mortality rate at least ten times higher than many similar elective procedures, fast-track surgery strategies may be of even greater advantage in such kind of setting. In our study, we offered ERAS components to both elective and urgent surgical population. Prevalence of urgent procedures over elective surgery (3.7:1) reflects the real-life situation with surgery in Zambia and is consistent with data from other research done in sub-Saharan Africa.[33] In elective surgical patients, commonly reported limitations for use of FTP include immobility, alcohol dependence, poorly controlled psychiatric disorders, lack of social support, and inability to follow-up for postoperative visits or complications.[11] Certainly, the multimodality of the ERAS pathway can limit its complete incorporation into routine practice, and despite its many benefits, ERAS still has a number of issues that need addressing in the future.
One of the valid concerns while using the FTP is patients’ safety after enforced early discharge.[29] Advantages of accelerated stay program should be carefully weighed against the risk of missing postoperative complications. This is especially true in a setting where transport is difficult and local nursing staff might be not sufficiently qualified. It is well known that early hospital discharge without sufficient recovery and lack of competent support can increase both patient and family anxiety, and may lead to readmission.[11] In our work, despite the priority was given to early discharge of the patients, we allowed them to go home only when they are considered to be safe with strict recommendations given on the timing and the process of follow-up. We had four readmissions because of developed postoperative complications, and interestingly enough, rehospitalisation of two of these patients actually followed prolonged stay in the hospital when they were chosen to be observed for a few days more after the procedure. Thus, late discharge cannot guarantee uneventful postoperative recovery in patients who underwent abdominal surgery. By contrast, among the patients discharged early, incidence of complications requiring readmission was low (2/61, 3.3%). The similar phenomenon is reported by Delaney et al.[22] suggesting that it is not the early discharge in itself that prevents the complication, rather late complications are likely to be developed in patients who are not doing well postoperatively in one or another way. It seems that selection of appropriate candidates for early discharge requires substantial surgical expertise in addition to the use of standardised discharge criteria.
Acknowledging unique physiological and psychological characteristics of paediatric patients, we include seventeen operated children into the study. Review of the literature shows that ERAS interventions in paediatrics contribute to improved outcome for patients and positively impact parent’s satisfaction with the surgical process,[3] and we anticipated clinical benefits for the children from inclusion into the program. We understand that standard FTP principles applicable to the adult patients may not be completely translatable to paediatric population. For example, no clear recommendations were found on use of perioperative pharmacological thromboprophylaxis in children, so we focused on early mobilisation and restricted use of drains and tubes. At the same time, other components of ERAS program may have exceptional weight in this population, and we applied them correspondently. It concerns, for instance, providing parents with full and timely information about the management process as well as reducing preoperative fasting time and early resumption of postoperative feeding.[3]
Despite this is our preliminary experience with FTP in abdominal surgery and the study design was not intended to demonstrate efficiency of ERAS protocol in this setting, obtained figures for LOS and morbidity/mortality appear to be comparable with the literature findings.[8,17,18] We saw that implementation of accelerated stay program for our patients was associated with sufficiently low rate of complications and readmissions and provided benefits for the patients and for the hospital likely enabling efficient management of resources. By contrast to some studies published,[9,21,29] but in accordance with others,[7] we offered elements of ERAS program to patients having ASA scores III and IV on preoperative assessment. We rationalised inclusion of these critical patients by the following. First, flexible employment of fast-track surgery components can give the critically ill patient an additional chance to recover. For example, use of mini-laparotomy with local anaesthesia and conscious IV sedation allowed us to avoid intraoperative complications and achieve uneventful recovery in three of our high-risk patients who were deemed to be poor candidates for a general anaesthetic. Second, proportion of patients presented with severe systemic disease including sepsis and shock is quite high among the urgent admissions (in our study it was 29.6%) and eliminating these patients from the study may distort the real results of the surgery. Nonetheless, we have to admit that we eliminated cases with ASA score V as these moribund patients routinely need postoperative intensive care and application of FTP elements in them can be difficult or even impossible. Third, apart from ASA score V, we did not see in our patients a strong association between the Physical Status score and postoperative mortality, as four out of eight deceased patients were scored I and II, while mortality among the ASA score IV sub-cohort was as low as 12% (3/23). We acknowledge, however, that our study is too weak to make assumptions about correlation relationship. On note, Horvath et al.[14] in a review article on evolution of ASA Classification System indicated that “ASA Physical Status is not intended and should not be used as predictor of operative risk, certainly not in individual patients”, and we see a clear rationale behind this conclusion. In our opinion, challenges with predicting post-operative morbidity could serve as an additional argument in favour of wider application of the ERAS program components to the management of high-risk patients.
Taking these observations into account, an answer to our research question is yes, ERAS pathway is a right choice of perioperative management employed at a peripheral hospital. Implementation of elements of ERAS program is in line with both recommendations of the Lancet Commission and Global Surgery Foundation to improve access to safe and affordable surgical and anaesthetic care in low- and middle-income countries (LMIC)[34] and Zambia’s first National Surgical, Obstetric, and Anaesthesia Strategic Plan.[12] At the time of our study, ERAS society (www.erassociety.org) produced targeted guidelines for hospitals in LMIC,[35] and we became particularly encouraged to intensify our efforts to refine protocol of perioperative care in accordance with new recommendations. We see the incorporation of FTP into routine surgical practice in low-resource environment as an incredible opportunity to standardise care, improve outcomes, save lives and reduce healthcare costs. Our study tells us that patient-centred individual approach with flexible application of ERAS components could increase chances for faster recovery in every particular patient. Therefore, implementation of ERAS protocols into clinical practice of hospitals operating in resource-scarce setting like ours would be mandated. In this respect, we agree with Fawcett et al.[11] that ‘ERAS does not make bad surgery good, but it does make good surgery optimal’.
LIMITATIONS
There are some limitations to this study that warrant mentioning. This was a retrospective record review and some data have inevitably been missed. Lack of a control arm and patient randomisation to participate in the protocol reduced the internal validity of the study and therefore no causal inferences were made from the data obtained. The research was based on a database from a single centre and after application of exclusion criteria not all patients operated in our hospital entered the study. There is a risk that some patients – potential participants – may not survive the transfer to our hospital, or be admitted in a critical condition with ASA score V and consequently excluded from the study. At the same time, we transferred four of our patients in complicated conditions to a higher referral institution. As a result, morbidity/mortality figures may be underreported. Additionally, the data obtained did not allow us to assess the compliance rate of the patients and surgical teams to FTP, so there is a possibility of variation in the implementation. The research was designed and controlled by a single investigator (without blinding) and this could lead to subjective assessments of the data. Clearly defined exclusion criteria and objective outcome measures, detailed description of the demographics, intervention and processing of the data aimed to reduce the selection and observer biases.
Among advantages of the study, this work represents a provincial initiative to change surgical care according to the principles of evidence-based medicine aiming to improve patient outcomes. As our hospital is peripheral, the sample investigated can be considered as being representative of the wider, predominantly rural, population of the country. This is a clinical study, so our results are close to those obtained in routine surgical practice and they might be considered as being sufficiently relevant. Besides, in-depth knowledge of the question and familiarity with clinical aspects of the cases enrolled by a well-motivated author of the manuscript could reinforce adherence to the treatment regimen and enhance the external validity of the study. Employing a short inclusion period (of 18 months in our study), according to Kooistra et al.,[36] can minimise changes over time in interventions reducing risk of chronology bias. In general, selecting a descriptive, “how-we-do-it”, design for the research, we focused on practical aspects of the ERAS program implementation and gained a valuable experience during this work. We hope that our findings could be of some interest for medical society. We also expect that this paper could be found useful to define areas for future larger-scale clinical trials and experimental studies.
CONCLUSIONS
Patients undergoing abdominal surgery in a resource-scarce setting constitute a serious challenge, as most of them admitted in emergent and/or complicated condition. In our institution, the introduction of ERAS program was associated with a change in the management of surgical patients towards an increased use of fast-track surgery pathway. Preliminary outcomes are promising, but further studies with a higher level of evidence are needed to verify the data presented and to develop recommendations for surgeons working in smaller hospitals.
What is already known on this topic?
• ERAS is a multimodal approach to the perioperative management of patients designed to improve the overall quality of care
• The program includes interventions that focus on anaesthesia, goal-directed fluid therapy, minimally invasive techniques, thromboembolic prophylaxis, nutrition, and early postoperative mobilisation
What this study adds
• Employment of ERAS protocol for general surgery population at second level hospital is feasible and safe
• Incorporation of FTP into routine surgical practice in low-resource environment could standardise care, has the potential to improve outcomes and reduce healthcare costs
ACKNOWLEDGMENTS
The current manuscript is the product of a multidisciplinary work with direct involvement of a large number of our hospital staff: primary care physicians, surgeons, anaesthetists, nurses, pharmacists, physiotherapists, dietician, information officers and management of the hospital, and I acknowledge all the contributors to this study.
Competing Interests
The author declares that he has no competing interests.
REFERENCES
- DeBarros M, Steele SR. Perioperative Protocols in Colorectal Surgery. Clin Colon Rectal Surg 2013;26:139-45; doi:10.1055/s-0033-1351128.
- Wijk L, Udumyan R, Pache B, Altman AD, Williams LL, Elias KM, McGee J, Wells T, Gramlich L, Holcom K, et al. International validation of Enhanced Recovery After Surgery Society guidelines on enhanced recovery for gynecologic surgery. Am J Obstet Gynecol 2019;221:237.e1-11; https://doi.org/10.1016/j.ajog.2019.04.028.
- Roberts K, Brindle M and McLuckie D. Enhanced recovery after surgery in paediatrics: a review of the literature. BJA Education 2020;20(7):235-41; doi:10.1016/j.bjae.2020.03.004.
- Malik K, Poletto G, Musto L, Giustiniano E, Cecconi M, and Civilini E. Implementation of a perioperative protocol to enhance open aortic repair. J Vasc Surg 2021;74:434-41; https://doi.org/10.1016/j.jvs.2020.12.102.
- Feldheiser A, Aziz O, Baldini G, Cox BPBW, Fearon KCH, Feldman LS, Gan TJ, Kennedy RH, Ljungqvist O, Lobo DN, et al. Enhanced Recovery After Surgery (ERAS) for gastrointestinal surgery, Part 2: consensus statement for anaesthesia practice. Acta Anaesth Scand 2016;60:289-334; doi:10.1111/aas.12651.
- Memtsoudis SG, Fiasconaro M, Soffin EM, Liu J, Wilson LA, Poeran J, Bekeris J, and Kehlet H. Enhanced recovery after surgery components and perioperative outcomes: a nationwide observational study. Br J Anaesth 2020;124(5):638-47; doi:10.1016/j.bja.2020.01.017.
- Nelson G, Kiyang LN, Crumley ET, Chuck A, Nguyen T, Faris P, Wasylak T, Basualdo-Hammond C, McKay S, Ljungqvist O, et al. Implementation of Enhanced Recovery After Surgery (ERAS) Across a Provincial Healthcare System: The ERAS Alberta Colorectal Surgery Experience. World J Surg 2016 Feb; doi:10.1007/s00268-016-3472-7.
- Hajibandeh S, Hajibandeh S, Bill V, and Satyadas T. Meta-analysis of Enhanced Recovery After Surgery Protocols in Emergency Abdominal Surgery. World J Surg 2020 Jan; doi:10.1007/s00268-019-05357-5.
- Saurabh K, Sureshkumar S, Mohsina S, Mahalakshmy T, Kundra P, Kate V. Adapted ERAS Pathway Versus Standard Care in Patients Undergoing Emergency Small Bowel Surgery: a Randomized Controlled Trial. J Gastrointest Surg 2020 May; https://doi.org/10.1007/s11605-020-04684-6.
- Tanious MK, Ljungqvist O, Urman RD. Enhanced Recovery After Surgery: History, Evolution, Guidelines, and Future Directions. Int Anesth Clinics 2017;55(4):1-11; doi:10.1097/AIA.0000000000000167.
- Fawcett WJ, Mythen MG and Scott MJ. Enhanced recovery: joining the dots. British J Anaesth 2021;126(4):751-5; doi: 10.1016/j.bja.2020.12.027.
- Mukhopadhyay S, Lin Y, Mwaba P, Kachimba J, Makasa E, Lishimpi K, Silverstein A, Afshar S, and Meara JG. Implementing World Health Assembly Resolution 68.15: national surgical, obstetric and anesthesia strategic plan development—the Zambian experience. Bull Am Coll Surg 2017; 102(6):28-35.
- World Medical Association Declaration of Helsinki Ethical Principles for Medical Research Involving Human Subjects. JAMA Nov 2013; 310(20):2191-4; doi:10.1001/jama.2013.281053.
- Horvath B, Kloesel B, Todd MM, Cole DJ, Prielipp RC. The Evolution, Current Value, and Future of the American Society of Anaesthesiologists Physical Status Classification System. Anesth 2021; 135:904-19; doi:10.1097/ALN.0000000000003947.
- Surgical Site Infection Event: Center for Disease Control. 2010; http://www.cdc.gov/nhsu/PDFs/pscManual/9pscSSIcurrent.pdf?agree=yes&next=Accept. Updated Jan 2015. Accessed October 06, 2022.
- Dindo D, Demartines N, and Clavien P-A. Classification of Surgical Complications A New Proposal with Evaluation in a Cohort of 6336 Patients and Results of a Survey. Ann Surg 2004; 240:205-13; doi:10.1097/01.sla.0000133083.54934.ae.
- Timan TJ, Hagberg G, Sernert N, Karlsson O, and Prytz M. Mortality following emergency laparotomy: a Swedish cohort study. BMC Surg 2021;21:322; https://doi.org/10.1186/s12893-021-01319-8.
- Watters DA, Wilson L. The Comparability and Utility of Perioperative Mortality Rates in Global Health. Curr Anesth Reports 2021; 11:48-58; https://doi.org/10.1007/s40140-020-00432-3.
- World Alliance for Patient Safety. Global patient safety challenge 2007-08: Safe Surgery Saves Lives, 2007. World Health Organisation, Geneva. http://www.who.int/patientsafety/challenge/safe.surgery/en/. Accessed 20 October 2022.
- Durlak JA, DuPre EP. Implementation Matters: A Review of Research on the Influence of Implementation on Program Outcomes and the Factors Affecting Implementation. Am J Community Psychol 2008; 41:327-50; doi: 10.1007/s10464-008-9165-0.
- Ugarte-Sierra B, Landaluce-Olavarria A, Cabrera-Serna I. Enhanced recovery after emergency surgery: Utopia or reality? Cir Esp 2021; 99:258-66.
- Delaney CP. Outcome of Discharge within 24 to 72 Hours after Laparoscopic Colorectal Surgery. Dis Colon Rectum 2008; 51:181-5; doi: 10.1007/s10350-007-9126-y.
- Ceresoli M, Pisano M, Abu‑Zidan F, Allievi N, Gurusamy K, Biffl WL, Tebala GD, Catena F, Ansaloni L, Sartelli M, et al. Minimally invasive surgery in emergency surgery: a WSES survey. World J Emerg Surg 2022;17:18; https://doi.org/10.1186/s13017-022-00419-x .
- Enrique EL, Hamdy KA. Minilaparotomy without general anesthesia for the treatment of sigmoid volvulus in high-risk patients: A case series of 4 patients. Inter J Surg Case Reports 2017; 34:23-6; doi:10.1016/j.ijscr.2017.02.055.
- Zhao JJ, Syn NL, Chong C, Tan HL, Ng JLX, Yap A, Kabir T, Goh BKP. Comparative outcomes of needlescopic, single-incision laparoscopic, standard laparoscopic, mini-laparotomy, and open cholecystectomy: A systematic review and network meta-analysis of 96 randomized controlled trials with 11,083 patients. Surg 2021;000:1-10; https://doi.org/10.1016/j.surg.2021.04.004.
- Van der Naald N, Prins MI, Otten K, Kumwenda D, Bleichrodt RP. Novel Approach to Treat Uncomplicated Sigmoid Volvulus Combining Minimally Invasive Surgery with Enhanced Recovery, in a Rural Hospital in Zambia. World J Surg 2017 Dec; https://doi.org/10.1007/s00268-017-4405-9.
- Balasubramanian A, Cheddie S, Naidoo NM, Singh B. An evaluation of mini-laparotomy cholecystectomy in the laparoscopic era: a rural experience. S Afr J Surg 2018;56(2):36-40; http://dx.doi.org/10.17159/2078-5151/2018/v56n2a2287.
- Bugada D, Bellini V, Fanelli A, Marchesini M, Compagnone C, Baciarello M, Allegri M, and Fanelli G. Future Perspectives of ERAS: A Narrative Review on the New Applications of an Established Approach. Surg Res Pract 2016; http://dx.doi.org/10.1155/2016/3561249.
- Chestovich PJ, Lin AY, and Yoo J. Fast-Track Pathways in Colorectal Surgery. Surg Clin N Am 2013;93:21-32; http://dx.doi.org/10.1016/j.suc.2012.09.003.
- Quiney N, Aggarwal G, Scott M, and Dickinson M. Survival After Emergency General Surgery: What can We Learn from Enhanced Recovery Programmes? World J Surg 2016; 40:1283-7; doi: 10.1007/s00268-016-3418-0.
- Boukili IE, Flaris AN, Mercier F, Cotte E, Kepenekian V, Vaudoyer D, Glehen O, and Passot G. Prehabilitation before major abdominal surgery: Evaluation of the impact of a perioperative clinical pathway, a pilot study. Scand J Surg Apr-June 2022:1-9; doi: 10.1177/14574969221083394.
- Sethi A, Debbarma M, Narang N. Impact of targeted preoperative optimization on clinical outcome in emergency abdominal surgeries: a prospective randomized trial. Anesth Essays Res 2018; 12:149-54.
- Sincavage J, Msosa VJ, Katete C, Purcell LN, Charles A. Post-operative Complications and Risk of Mortality Following Laparotomy in a Resource-Limited Setting. J Surg Res 2021 April; 260:428-35; doi:10.1016/j.jss.2020.11.017.
- Meara JG, Leather AM, Hagander L, Alkire BC, Alonso N, Ameh EA, Bickler SW, Conteh L, Dare AJ, Davies J. Global Surgery 2030: Evidence and solutions for achieving health, welfare, and economic development. Lancet 2015;386:569-624; http://dx.doi.org/10.1016/S0140-6736(15)60160-X.
- 35. Oodit R, Biccard B, Panieri E, Alvarez AO, Sioson MRS, Maswime S, Thomas V, Kluyts H-L, Peden CJ, de Boer HD, et al. Guidelines for Perioperative Care in Elective Abdominal and Pelvic Surgery at Primary and Secondary Hospitals in Low-Middle-Income Countries (LMIC’s): Enhanced Recovery After Surgery (ERAS) Society Recommendation. World J Surg 2022;46:1826-43; https://doi.org/10.1007/s00268-022-06587-w.
- Kooistra B, Dijkman B, Einhorn TA, and Bhandari M. How to Design a Good Case Series. J Bone Joint Surg Am 2009;91 Suppl 3:21-6; doi:10.2106/JBJS.H.01573.
Medical Journal of Zambia, Vol 50, 2
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.