Bowel Obstruction from Complete Transmural Migration of a Gossypiboma into the ileum; A rare occurrence
Horace Ojobo Agada
Department of Surgery, Dalhatu Araf Specialist Hospital, Lafia, Nasarawa State, Nigeria
Yakubu Malgwa Ishaku
Department of Surgery, Dalhatu Araf Specialist Hospital, Lafia, Nasarawa State, Nigeria
Joel Iliya
Department of Surgery, Dalhatu Araf Specialist Hospital, Lafia, Nasarawa State, Nigeria
DOI: https://doi.org/10.55320/mjz.50.3.416
Keywords:Anastomosis, Bowel obstruction, Gossypiboma, laparotomy
ABSTRACT
Gossypibomas are infrequent abdominal pathology associated with increased morbidity and mortality. They are foreign bodies of predominantly cotton material that are erroneously left in body cavities following surgery. They represent an extremely rare but avoidable cause of bowel obstruction and should be considered as a differential diagnosis in patients presenting with bowel obstruction following previous abdominal surgery.
We present the case of a young woman with clinical features in keeping with mechanical bowel obstruction from suspected post-operated adhesion. However, intra-operative finding revealed a complete transmural migration of a Gossypiboma into the terminal ileum. She had segmental ileal resection, extraction of the gossypiboma and primary end-to-end ileo-ileal anastomosis. Her recovery period was uneventful.
INTRODUCTION
Gossypiboma refers to a mass of cotton material unintentionally left in body cavities following surgery. Reported cases are few with incidence in the range of 1 in 1000 to 1500 Surgeries, largely due to the medico-legal dimension of the pathology.[1] They are also referred to as textiloma, arising from operative error with attendant increased morbidity and mortality. They have been reported following gynaecological, cardiothoracic, neurosurgical, urological and general surgical procedures.[2] While humans are not immune to mistakes, such mistakes can be catastrophic, resulting in profound and grave consequences for the patient, surgeon, and institutions. It is paramount therefore to ensure that such mistakes are brought to the minimum through the deployment of preventive measures. Gauze piece, surgical sponge and abdominal towel, remains the most frequently identified retained surgical materials. This could be attributed to their high frequency of use at surgeries, ill-defined shape and relatively small size.[3]
Acute mechanical bowel obstruction is a common cause of acute abdomen requiring operative intervention globally. There is geographical variation in the pattern of bowel obstruction. whereas obstructed hernia is considered the most common cause in low and middle-income countries, post-operative adhesion is the main cause in high- income countries due to the higher frequency of abdominal surgeries. However, recent studies in the low and middle-income countries have shown increasing incidence of post-operative adhesions as the aetiology for mechanical bowel in these regions.[4]
In this case report, we present a rare cause of bowel obstruction from an intraluminal Gossypiboma in a young woman.
CASE PRESENTATION
A 40-year-old woman presented to our emergency department with colicky abdominal pains, vomiting, abdominal distension and relative constipation of 5 days duration. She has had 2 previous abdominal surgeries that included myomectomy and laparotomy for acute abdomen done 2 years and 7 months ago respectively. Physical examination showed an acutely ill-looking young woman in painful distress who was haemodynamically stable. The abdomen was distended, moved with respiration, with intact hernia orifices and a midline scar. It was tympanitic, and non-tender. There was exaggerated bowel sound. Digital rectal examination showed scanty stool in the rectum. A diagnosis of partial bowel obstruction from postoperative adhesion was made. Plain abdominal x-ray demonstrated findings in keeping with small bowel obstruction. Her laboratory investigation results were all within normal values.
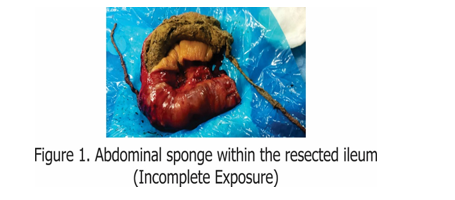
A non-operative protocol was initiated and subsequently abandoned after 48 hours due to worsening symptoms. She was then worked up for and had laparotomy with intra-operative findings of dilated jejunum and proximal ileum, collapsed distal ileum and large bowel, a firm but indentable ileal mass about 45 cm from the ileocaecal junction that measured 10cm.[Figures; 1 and 2] A segmental ileal resection incorporating the mass with a primary end-to-end ileo-ileal anastomosis was effected. [Figure 2]


She subsequently had an unremarkable recovery and was discharged on post-operative day 10.
DISCUSSION
Bowel obstruction is a common cause of acute abdomen with varied aetiology. Common causes of bowel obstruction in a post-operative patient includes, paralytic ileus, adhesions, internal hernias and intussusceptions. While Gossypibomas are uncommon clinical condition, their transmural migration with bowel obstruction is extremely uncommon.[5] Factors predisposing to this pathology includes, emergency surgeries, prolonged surgeries, on table change of procedure or team, team fatigue, sudden unexpected occurrences as well as failure of meticulous gauze count.[6]
The clinical presentation of Gossypibomas are usually non-specific and occurring weeks to year’s post-surgery. This has resulted in diagnostic conundrum as in our index patient with delayed definitive treatment and consequent increased morbidity. The presence of these materials may incite an exudative or a fibrotic change with resultant abscesses or inflammatory mass lesion. Reported cases of intraluminal Gossypiboma as an aetiology of bowel obstruction are extremely uncommon.[2,5,7] The mechanism of bowel obstruction arising from a Gossypiboma could be from extrinsic compression or intraluminal impedance following transluminal migration. Transluminal migration is postulated to result from the pressure effect of the mass of cotton material on the bowel wall with subsequent inflammation, necrosis, migration and finally sealing up of the point of entrance.[7] This was the cause in our patient.
Since this condition is of an avoidable nature, important measures aimed at its prevention should be considered. These include avoidance of free gauze intra-peritoneally and meticulous gauze count prior to abdominal wound closure. The majority of cases of gossypibomas are diagnosed intra-operatively, however, the advent of technological advances has helped in the pre-operative diagnosis of this pathology. The use of radio-opaque tags on surgical materials could be detected pre-operatively using image studies. However, such radio-opaque markers disintegrate over time creating challenges with diagnosis following prolonged stay of such material in body cavities. Ultrasonography scan and Computerized tomography scan (CT-Scan) have both being utilized with some successes. CT-Scan is a valuable radiological tool for the pre-operative diagnosis of retained surgical materials. Retained sponges are typically seen as soft tissue density masses and may show a whorled texture or a spongiform pattern containing gas bubbles. However, the radiological appearances of most retained sponges are non- specific.[8] Novel methods of diagnosis include the use of radio-frequency identification microchips and electronic article surveillance system.[6,8,9]
CONCLUSION
Gossypiboma is an uncommon, potentially preventable, and significant complication following surgery.
It commonly presents with diagnostic dilemma with majority of cases being diagnosed intra-operatively. Thus, it should be considered as a differential diagnosis in patients presenting with bowel obstruction following previous surgery.
REFERENCES
- Alef M, Khaoula A, Badreddine A, Jasser Y. Gossypiboma; the failure of a successful intervention. PAMJ 2020; 36: 335
- Mohammed Y, Ali A. Gossypiboma, an overlooked cause of Bowel obstruction; A Case Report and literature Review. East Cent. Afr J Surg 2015;20(1):98
- Moniruzzaman Sarker, Golam Kibari AK, Manzurul Haque MD, Kali Prosad Sarkar, Khaliher Rahman. Spontaneous migration of a retained surgical mop into the small intestinal lumen causing subacute intestinal obstruction; a case report. TAJ 2006; 19;34-37
- Ibrahim UG, Amina IE. Changing pattern of adult intestinal obstruction in Nigeria; A narrative review. Niger J Basic Clin Sci 2021; 18:1-4
- Genocosmangolu R, Inceoglu R. An unusual cause of small bowel obstruction; case report. BMC Surgery 2003; 3:6
- Umunna JI. Gossypiboma and its Implications. J West Afr Coll Surg 2012; 2(4): 95-105
- Patil KK, Patil SK, Gorad KP, Pandial AH, Arora SS, Gautum RP. Intra-luminal migration of Surgical sponge; gossypiboma. Saudi J Gastroenterol 2010; 16(3): 221-222
- Kalovidoris A, Kehagias D, Moulopoulos L, Gouliamos A, Pentea S, Vlahos L. Abdominal retained surgical sponges; CT appearance. Eur Radiol 1999; 9[7]; 1407-1410
- Fabian CE. Electronic tagging of surgical sponges to prevent their accidental retention. Surgery 2005; 137(3) :298-301
Medical Journal of Zambia, Vol 50, 3
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.