Diastolic dysfunction due to bedaquiline: A Case Report from Lusaka, Zambia
Ireen Chanda Bwalya
Department of Infectious Diseases, HIV and TB unit, Levy Mwanawasa University Teaching Hospital, Lusaka, Zambia.
DOI: https://doi.org/10.55320/mjz.50.3.412
Keywords:tuberculosis, drug resistant, laboratory, diagnosis, case report
ABSTRACT
Background: There is no published case of diastolic dysfunction arising due to bedaquiline treatment for Multi-Drug Resistant Tuberculosis (MDR-TB). Diastolic dysfunction is not listed as a potential complication of treatment with bedaquiline. This case report is the first to link bedaquiline to diastolic dysfunction. Clinicians should be aware of this potential complication, and ensure that patients are monitored and investigated appropriately.
Case Presentation: A 47 year old female presented with fever, productive cough and drenching night sweats for more than 2 weeks prior to presentation. There was no hemoptysis, chest pains or weight loss. She however, felt breathless after a heavy bout of coughing. Fever was intermittent, and most pronounced at night. The patient denied any weight loss over the past month. The patient had no history of HIV, diabetes, hypertension or heart disease. There were no previous episodes of TB. There was history of contact with a patient with MDR-TB patient. The patients’ son, who shared a house and all living spaces with the patient, was being treated for MDR-TB at the time of presentation. The patient did not drink or smoke. There was no history of illicit drug use. She worked as a restaurant manager. Due to the history of very close contact with MDR-TB, the patient was commenced on the longer, oral only regimen for MDR-TB which includes bedaquiline. Four weeks after commencement of bedaquiline, the patient complained that both feet were swelling. There were no other symptoms or signs of cardiovascular disease. An Echocardiogram done during the fifth month showed an ejection fraction of 71% and diastolic dysfunction. The patient was commenced on diuretics and continued on MDR-TB treatment. An echocardiogram that was repeated at month 15 review showed an ejection fraction of 64%, normal left ventricle and normal systolic and diastolic function.
Conclusions: Diastolic Dysfunction has not previously been reported in patients on bedaquiline. This is the first case report to link bedaquiline to diastolic dysfunction. More studies need to be done to determine conclusively whether bedaquiline can cause diastolic dysfunction.
INTRODUCTION
Multi Drug Resistant Tuberculosis (MDR-TB) refers to tuberculosis that is resistant to both Isoniazid and Rifampicin, two of the key drugs that are used in managing drug susceptible TB. Globally, the prevalence of multi-drug resistant TB has been increasing. This is due, in part, to improved diagnosis of TB using Cepheid Gene X-pert machines. Inappropriate treatment regimes, poor compliance and loss to follow up have also contributed to the increase in the global prevalence of MDR-TB. In Zambia, the prevalence of MDR-TB is estimated to be 0.3% in new patients, and 1.8% in previously treated patients [1] .
Bedaquiline (BDQ) is one of the key drugs being used to treat MDR-TB. It acts by disrupting mycobacterial Adenosine Triphosphate (ATP) Synthase [2] , resulting in death of the mycobacterium [3] . Bedaquiline is known to cause Electrocardiographic (ECG) changes that can be life threatening, in some instances. The commonest ECG change associated with bedaquiline is prolongation of the QT interval [4] . To my knowledge, there is no report of diastolic dysfunction in patients on bedaquiline. This case presentation describes a patient who developed diastolic dysfunction while on bedaquiline treatment for MDR-TB.
CASE PRESENTATION
A 47 year old female presented to our clinic with history of fever, cough and drenching night sweats for more than 2 weeks prior to presentation. The cough was productive of white sputum. There was no hemoptysis. There were no chest pains. She however, felt breathless after a heavy bout of coughing. Fever was intermittent, and most pronounced at night. The patient denied any weight loss over the past month. Her appetite had been poor the week prior to presentation. She did not notice any swellings in the neck, armpit, groin, or on any other part of the body. There was no history of headache, dizziness or blurring of vision. There was no weakness or numbness of any of the limbs. She denied having abdominal pains, diarrhoea or vomiting. There were no urinary symptoms. Patient denied having any palpitations of feeling tired easily. There was no breathlessness on exertion or on lying flat. There was no swelling of legs. There was no significant past medical history. The patient had no history of HIV, diabetes, hypertension, heart disease, seizure disorder. There were no previous episodes of TB. There was history of contact with a patient with MDR-TB patient. The patients’ son, who shared a house and all living spaces with the patient, was being treated for MDR-TB at the time of presentation. The patient did not drink or smoke. There was no history of illicit drug use. She worked as a restaurant manager at a busy restaurant in the central business district within the capital.
On examination, the patient appeared fatigued and restless. She was sweating. There was no pallor or jaundice. Temperature was 36.90C, Blood pressure was 137/84mmHg, pulse was 88 beats per minute, Respiratory rate was 20 breaths per minute. Oxygen saturation was 99%. There were no lymph nodes palpable. There was no edema. The chest was clear. There were no rhonchi or crepitations. Heart sounds were normal. Abdominal examination was unremarkable.
Sputum examination by gene Xpert did not detect Mycobacterium Tuberculosis (MTB). Hemoglobin (Hb) was 14.8g/dl, Aspartate Amino Transferase (AST was 26.7 U/l, creatinine was 61.83 micromoles/l.
Due to the history of very close contact with MDR-TB, the patient was commenced on the longer, oral only regimen for MDR-TB. The patient was commenced on Bedaquiline (BDQ) 400mg daily for two weeks, Linezolid 600mg daily, Levofloxacin 750mg daily and clofazimine 100mg daily. She was also given vitamin B6 supplements at 100mg per day. Baseline corrected QT interval (QTc) was 436. The patient was reviewed in chest clinic 2 weeks after commencement of MDR -TB treatment. She was feeling better. She felt stronger, but cough was still present. There was no fever. Bedaquiline dose was reduced to 200mg three times a week.
The patient was reviewed again 4 weeks after the initial presentation. Cough had subsided. There was no fever. She complained that her feet were beginning to swell. There was no numbness or pain in the feet. The patient attributed her symptoms to prolonged standing in the restaurant where she worked. The swelling subsided when she elevated her limbs.
During the 2nd, 3rd and 4th months of treatment, the patient experienced joint pains, which were attributed to bedaquiline. There was no swelling of the feet. By the fifth month, swelling of the feet recurred. There were no other symptoms of cardiovascular disease. An Echocardiogram showed an ejection fraction of 71% and diastolic dysfunction. Her blood pressure was in the range 103-142 systolic, and 73-82 for the diastolic blood pressure.
The patient was commenced on furosemide 40mg once daily, and continued on MDR-TB treatment. At the 6 and 7th monthly reviews, the patient experienced occasional swelling of both feet. There were no other symptoms. BDQ was discontinued at the end of the 6th month. At the 11th monthly review, joint pain and swelling completely stopped. An echocardiogram that was repeated at month 15 review showed an ejection fraction of 64%, normal left ventricle and normal systolic and diastolic function. Furosemide was discontinued. A summary of the patient’s test results is shown in the table 1 below. The patient has remained asymptomatic throughout the rest of her treatment.
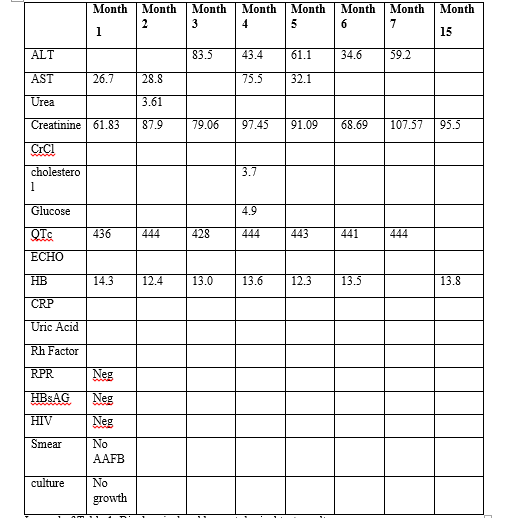
Legend of Table 1: Biochemical and haematological test results
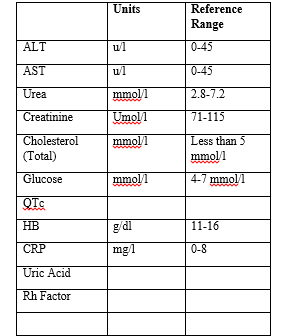
Legend of Table 2: Reference ranges and Units
DISCUSSION
Diastolic Dysfunction has not previously been reported in patients on bedaquiline. Our patient was treated with diuretics, as they have been shown to be useful in patients with heart failure and preserved ejection fraction [5] . There are several limitations in this case report. We did not measure natriuretic peptides in this patient, as the tests were not available locally. Creatinine and liver function tests could not be done consistently during the course of treatment, due to lack of reagents. Sputum culture results were only available on two occasions, despite samples being submitted for analysis on a monthly basis. This was also due to lack of reagents. This case clearly highlights the challenges of managing MDR-TB in resource constrained settings.
Joint pains are known to be a common complication of treatment with bedaquiline [6] . The patient experienced joint pain even after discontinuation of bedaquiline treatment, probably due to the long half-life of bedaquiline, which is approximately 4-5 months [7] .
Even though the patient had other risk factors for heart failure with preserved ejection fraction, namely obesity and female gender [8] , the patient’s diastolic dysfunction can be attributed to Bedaquiline, as cardiac function returned to normal after cessation of bedaquiline. This is the first case report to link bedaquiline to diastolic dysfunction. More studies need to be done to determine a conclusively whether bedaquiline can cause heart failure with preserved diastolic dysfunction.
LIST OF ABBREVIATIONS
AAFB - Acid alcohol fast bacilli
ALT - Alanine Aminotransferase
AST - Aspartate Aminotransferase
ATP- Adenosine Triphosphate
BDQ - Bedaquiline
CRP - C-reactive protein
ECG - Electrocardiogram
ECHO - Echocardiogram
FBC - Full blood count
HB - Hemoglobin
HBsAg - Hepatitis B Surface Antigen
MDR - Multi-drug resistant
MTB - Mycobacterium Tuberculosis
Neg - Negative
Rh - Rheumatoid
RPR - Rapid Plasma Reaginin
DECLARATIONS
Consent to Participate
Consent was obtained from the patient prior to preparation of the manuscript. A signed consent form is available for scrutiny.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Availability of Data and Material
All the relevant information related to the case is summarised in the manuscript. The original medical record is kept in the hospital registry.
Competing Interests
None.
Funding
Not applicable.
Acknowledgments
Special thanks to patient POM for granting consent to use the case for publication.
REFERENCES
- Kapata N et al. Multidrug-resistant TB in Zambia: Review of national data from 2000 to 2011. Tropical Medicine & International Health 2018; 18(11): 1386-1391.
- Chahine EB, Karaoui LR, Mansour H. Bedaquiline: a novel diarylquinoline for multidrug-resistant tuberculosis. Annals of Pharmacotherapy 2014; 48(1): 107-15.
- Nagabushan H and Roopadevu HS. Bedaquiline: A novel antitubercular drug for multidrug-resistant tuberculosis. J Postgrad Med 2014; 60: 300-302.
- Gao J et al. Bedaquiline-containing regimens in patients with pulmonary multi-drug resistant tuberculosis in China: focus on the safety. Infectious Diseases of Poverty 2021; 10(32): 1-10.
- Gazewood JD and Turner PL. Heart Failure with preserved ejection fraction: Diagnosis and Management. American Family Physician 2017; 96(9): 582-588.
- Goulooze SC, Cohen AF and Rissman R. New Drug Mechanisms: Bedaquiline. British Journal of Clinical Pharmacology 2015; 80:2.
- Deoghare S. Bedaquiline: a new drug approved for treatment of multidrug-resistant tuberculosis. Indian Journal of Pharmacology 2013; 45(5):536-537.
- Oghlakian GO, Sipahi I and Fang JC. Treatment of Heart Failure with Preserved Ejection Fraction: Have we been pursuing the wrong paradigm? Mayo Clinic Proc 2011; 86(6): 531-539.
Medical Journal of Zambia, Vol 50, 3
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.