Knowledge, attitude and readiness to use contraceptives among postpartum women at a tertiary hospital in southwest Nigeria
Temitope Azeez Olukunle
Department of Obstetrics and Gynaecology, University College Hospital, Ibadan, Nigeria.
Olayinka Oladunjoye Ogunbode
Department of Obstetrics and Gynaecology, College of Medicine, University of Ibadan, Ibadan, Nigeria.
Rukiyat Adeola Abdus-salam
Department of Obstetrics and Gynaecology, College of Medicine, University of Ibadan, Ibadan, Nigeria.
DOI: https://doi.org/10.55320/mjz.50.3.411
Keywords:Post-partum contraception, Family planning, Contraceptive counselling.
ABSTRACT
Background Postpartum family planning is vital in the prevention of unintended pregnancy and closely spaced pregnancies in the first year post-delivery. This study was designed to examine the postpartum women’s knowledge, attitude, belief and readiness to contraceptive use.
Methods: This descriptive cross-sectional study was conducted among one hundred and ninety-four consenting women, six weeks post-delivery, at the University College Hospital, Ibadan, Nigeria using an interviewer-assisted structured questionnaire. Data was analysed using IBM Statistics for Windows Version 23.0. Tests of association was done using chi-square and statistical significance was set at p-value of < 0.05.
Results: Many of the respondents (60.8%) were in the age group 30-39 years and the majority (90.3%) had tertiary level of education. Most of the respondents got their information from health talks at antenatal clinic (42.8%) and health workers (42.3%). The majority (82.5%) of respondents were aware of contraception and 157(80.9%) intended to use contraceptives. The most preferred contraceptive methods were implants (19.1%). Respondents with three or more children alive(p=0.001), had statistically significant associations with prior use of contraception while those with the tertiary level of education(p=0.001), of the Christian religion (p=<0.001) and had contraceptive counselling during pregnancy (p=0.031) had statistically significant associations with good knowledge of contraception.
Conclusion: The knowledge and readiness to use contraceptives was high but only about half were willing to adopt contraception post-delivery. There is therefore the need for the enactment of government policy and legislation that will ensure wide coverage and availability of contraception counselling among pregnant women.
INTRODUCTION
The desire for birth spacing and contraceptive use is as old as humanity. According to the international human right laws, access to contraceptives is one of the basic human rights and to achieve safe motherhood; family planning is one of the six fundamental health interventions[1] . While contraceptive use is important throughout an individual’s and couple’s reproductive life, postpartum family planning focuses on the prevention of unintended and closely spaced pregnancies through the first 12 months following childbirth.[2] It is estimated that of the 210 million pregnancies that occur annually worldwide, about 80 million (38%) are unplanned, and 46 million (22%) ends in abortion.[3]
Globally, 62% of married women aged 15 to 49 years use a method of family planning and 56 percent use modern methods such as the pills, intrauterine devices, implants, injectables, condoms, and sterilization.[4] These rates are two times higher among women living in high-income countries compared to low-income countries due to differences in demand, availability, and access to modern methods of contraception.[4] At country levels, use of any method of family planning among married women varies significantly, ranging from 9% in Eastern Sudan to 90% in Belgium.[5-6]
In Nigeria, despite a high awareness of contraception,[7] the latest Nigeria demographic and health survey (NDHS), in 2018, reported modern contraceptive usage of 17%.[6] This report also showed that from 2013 to 2018 contraceptive use increased from 10 to 12%.[8-9]
Generally, in developing countries, especially in Africa and Asia, the percentage of married women with unmet need for modern contraception ranges from 18-37%[10] and the unmet need for contraceptive use in Nigeria is 19%.[8] The World Health Organization (WHO) technical committee recommends birth spacing with an interval of at least 12 months before couples attempt to become pregnant.[11]
Post-partum women may resume sexual intercourse in the postpartum period before the initiation of uptake of contraceptive and family planning. In South-west Nigeria, about two-thirds of women who had resumed sexual activity were not using any form of family planning.[12] A study done in two local governments in Ebonyi, South-South Nigeria reported that 87% of postpartum women have knowledge of methods of contraception.[13]
Despite good knowledge and awareness, prompt uptake of family planning methods is still suboptimal and affected by several factors. The use of modern contraceptive can be improved by increasing family planning counselling during the antenatal, intrapartum care, improving awareness of the populace about the benefits to the women, family and community; and increase in the government and NGO funding of family planning program, improving access to the services.[14-15]
Exclusive breast-feeding may confer some protection and pregnancy prevention, nursing mothers find it difficult to exclusively breastfeed after resumption of work or while they are students.[16-17] This could result in many cases of unwanted pregnancies. Births that are spaced too closely together pose substantial health risks for the mother and child.
This study was designed to assess the intention to adopt postpartum contraception, to examine the postpartum patients’ disposition, attitude, belief and practice to contraceptive use and to determine the contraceptive preferences among postpartum Nigerian women.
METHODS
Study site and design: This descriptive cross-sectional study was done at the University College Hospital (UCH), Ibadan between February1, 2020 and May 31, 2020, among one hundred and ninety-four recently delivered women. The women were recruited at the six-weeks post-delivery clinic visit. Women aged <18years, non-consenting women or those with medical conditions that needed emergency care were excluded from this study.
Sample size calculation: Respondents were selected using the formula for cross-sectional studies by Leslie Fisher formula[18] , n = z2pq/d2, where n is the minimum sample size expected, p is the prevalence of contraceptive use in Nigeria (0.12)[8] , d is the precision of the study which is 0.05 and Z is the area under normal curve corresponding to 95% confidence interval = 1.96. Using a non-response rate of 20% to improve the power of the study, the minimum sample size was 194 respondents.
Sampling technique: The study respondents were selected using purposive sampling technique and consecutive women were recruited into the study after counseling following informed consent.
Data collection instrument: Data was collected using pretested interviewer administered semi-structured questionnaire developed using information from the literature and face validated by experienced gynecologists. The questionnaire was pre-tested among 20 women attending the postnatal clinic of Adeoyo Maternity Teaching, Hospital (AMTH), Yemetu, Ibadan, Nigeria.
The questionnaires were administered shortly before the six-weeks post-delivery clinic visit. It comprised of four sections and the information obtained included socio-demographic data, knowledge about the various methods of contraception, their source of information, the attitude of women towards methods of contraception and misconception towards the methods, readiness to use contraceptives, previous use of contraceptives and side effects known or experienced. The research assistants were trained in the process of data collection.
Outcome variables: Knowledge on contraception was measured by using three questions which include - knowledge of the meaning of contraception, contraceptive methods and side effects of contraceptives. Items under each question were scored 1 except best definition of family planning which was scored 2. Knowledge of types of contraceptive methods was given a score of 1 for every method identified by the respondents. A score of 6 and above is classified as good knowledge and poor knowledge if score is less than 6. Respondents who scored 5 and above on knowledge of side effects of contraceptive had good knowledge while a score of less than 5 had poor knowledge. The overall good knowledge was interpreted as having good knowledge in any two of the variables above while poor knowledge was having one good knowledge only one variable or none.
Attitude towards contraceptive use was determined by asking the respondents if they intended to use any method of contraception. Those with positive attitude intended to use any method of contraception. Readiness to use contraceptive was measured by asking the respondent if they plan to get a contraceptive device at family planning clinic using the opportunity of the six-weeks post-delivery clinic visit for family planning uptake.
Data analysis: This was done using IBM SPSS Statistics for Windows, Version 23.0, Armonk, New York: IBM Corp. Frequencies and proportions were used for categorical variables and test of association between categorical variables was assessed using Chi-square tests. The level of significance was set at p of <0.05.
Ethical consideration: The ethical principles of autonomy, beneficence and non-maleficence were maintained. Ethical approval was obtained from the University of Ibadan, Ibadan and the University College Hospital, Ibadan (UI/UCH), Institutional Review Board.
RESULTS
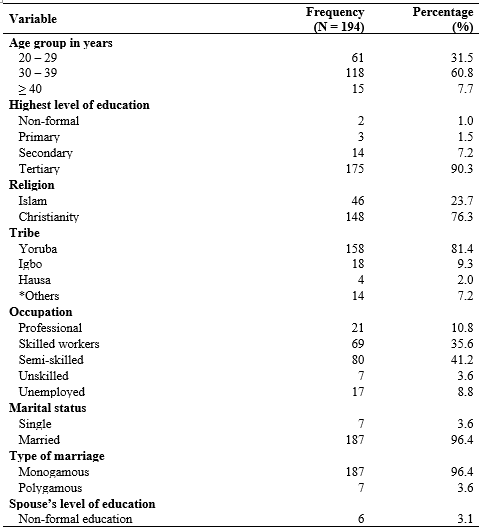
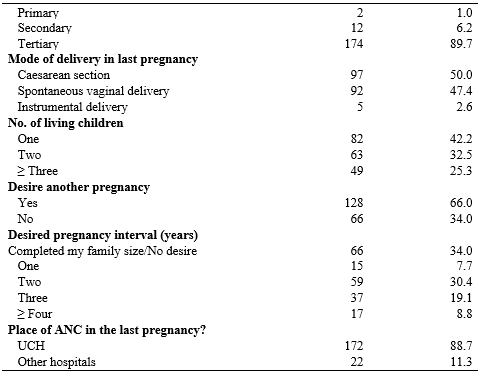
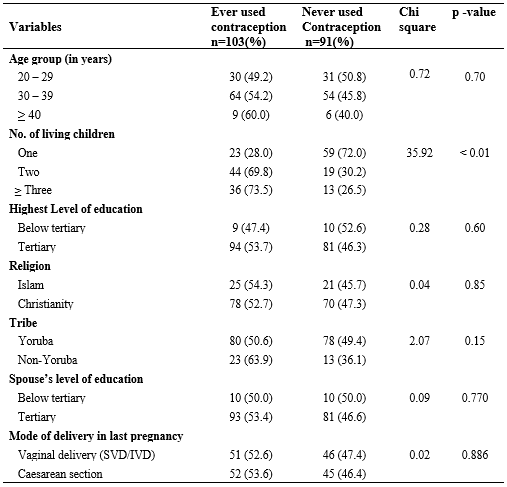
Many of the respondents (60.8%) were in the age group 30-39 years, while the majority were married (96.4%), had tertiary level of education (90.3%) in monogamous relationships (96.3%) and had their antenatal care in the last pregnancy at UCH Ibadan. This is shown in table 1.
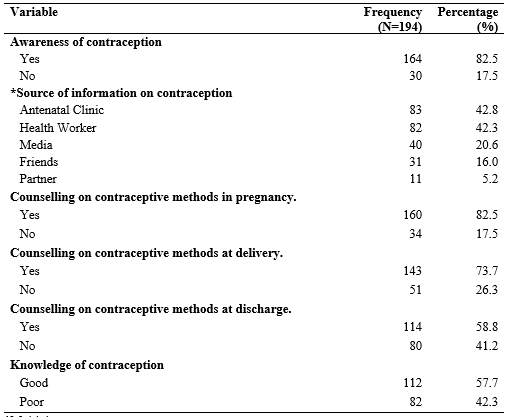
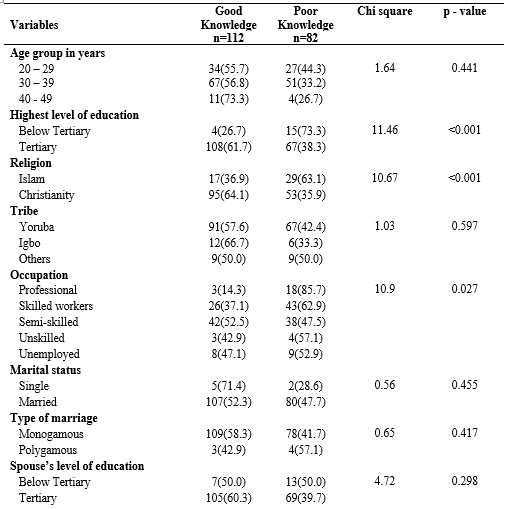
One hundred and sixty-four (82.5%) respondents were aware of contraception. The commonest sources of information were from antenatal clinic (42.8%) and health workers (42.3%). One hundred and twelve (57.7%) respondents had good knowledge of contraception. This is shown in Table 2.
One hundred and fifty-seven (80.9%) respondents intended to use contraception, out of which 54(34.4%) were willing to take contraception at the six weeks postnatal clinic visit. The most preferred contraceptive methods were implants (19.1%) and the fear of side effects (40.5%) was the most frequent reason for not intending to use any form of contraception. This is shown in Table 3.
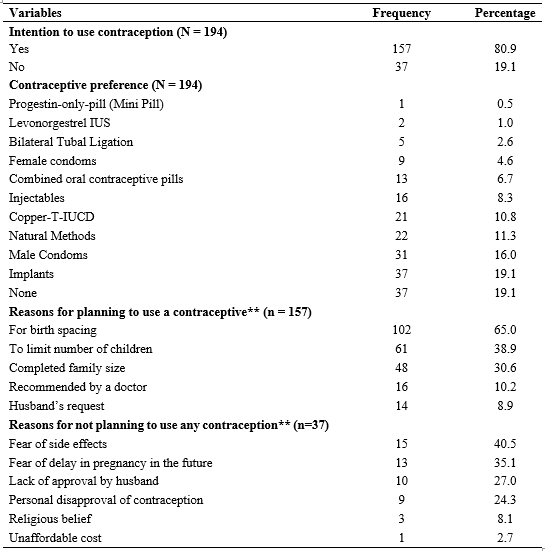
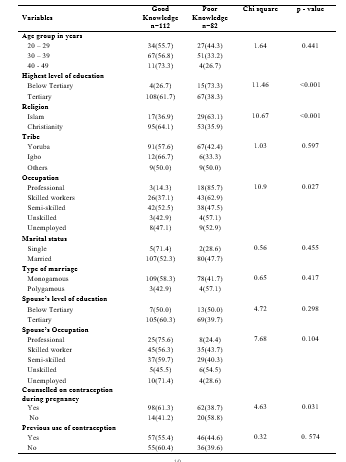
Table 4a shows that women with two or more children had statistically significant associations with prior use of contraception (p=<0.001). Respondents with the tertiary level of education(p=<0.001) and of the Christian religion (p=<0.001) had statistically significant associations with good knowledge of contraception. This is shown in Table 4b.
DISCUSSION
In this study the respondents were postpartum women who delivered at least six weeks prior to the study, mostly aged 20-29years, with tertiary education, more than half were married, and one-third had completed their family size. About four in five women, were counselled on family planning during antenatal care; three-quarter and half of the respondents received family planning counselling at delivery and at the time discharge respectively.
This study shows that 82.5% of the respondents are aware of at least a method of contraception and only 58% demonstrated good knowledge on contraception majority of whom are of tertiary education (61.7%) This may be because most of the respondents attended ANC during their last pregnancy, had tertiary level of education and had received information on contraception at least once during the antenatal period and prior to discharge. Previous studies demonstrated the role of age and education in the knowledge, awareness and positive attitudes to the use of contraceptives.[13-19] Women who are educated demonstrated a higher level of awareness and knowledge of contraception.[13,19,20] This pattern of awareness and knowledge of contraception is similar to the finding of a study done in India which reported high awareness of 90% and 90.8% respectively.[21-23] However another study in India documented that though respondents demonstrated high level of awareness of 70%, only about 30% had correct knowledge on contraceptive use.[24] This shows the need for health talk to be strengthened across health centers as it is a major source of information.
The majority of the respondents in this study got their information from health talks at antenatal clinic and health workers. This is in contrast to a study done by Mao J et al, who reported that most postnatal women got information from their friends.[25] Bajracharya et al reported the media as the main source of information.[22] The findings from these various studies shows that all the possible sources of information are important so efforts should be made to ensure that these sources are adequately equipped with the right information.
This study revealed that many of the respondents (80.9%) exhibited positive attitudes to contraceptive use with about 87.9% preferring modern contraceptives. Similar result was reported by Nagedo et al[26] however, Sharma et al reported a lower percentage of 28.2% of respondents that showed positive attitude to contraception.[20] In this study, implants (23.4%) was the most preferred contraceptive, followed by male condom (19.8%) while minipill (0.6%) was the least preferred. A study by Rita et al revealed these similar findings however Gupta et al reported barrier methods as the most commonly used contraceptive among postpartum women.[13-27] This may be because most of the participants in the latter study had between two and four children necessitating the need for long-acting reversible contraception and since implants require a single visit for insertion, it may be more convenient for the respondents. The condom is also cheap, readily available and may be a better choice for the partners of the respondents who do not want to take any form of chemical agent as contraception.[28]
In this study, a little over one-third of the respondents (34.4%) were ready to adopt a method at at six-weeks post-delivery. Most of those respondents who were not ready to adopt at the visit cited the fear of side effects and delayed return to fertility, but an important proportion also mentioned lack of approval by their husband. This shows the role husbands play in decision making on contraception and the need to involve them during antenatal period. This could be achieved through the distribution of pamphlets on contraception to pregnant women to be given to their husband at home. A few respondents cited religious beliefs so there is need to further educate the religious leaders or organizations on the benefits of contraception and to promote any contraceptive choice acceptable by couples including traditional methods.
This study revealed that the number of children per women were significantly associated with women’s readiness to adopt any method of contraception after delivery. Women that married at age group 16-24 and women with three or more children had highest level of readiness of 44.9% and 18.3% respectively. Women that married early tend to agree to birth spacing due to their long reproductive period than those that married late, who might want to complete their desired number of children within the shortest possible time due to possible age limit and the wrong notion that contraceptives delay pregnancy. Also, multiparous women most especially with three or more children have good attitude and more readiness as reported in this study. Studies done in Zimbabwe and India also supports the fact that parity as a positive impact on contraceptive uptake.[29-30]
Women with two or more children had statistically significant associations with prior use of contraception (p=<0.001). This is similar to other studies, especially in countries with low levels of contraceptive uptake, which reported that the higher the number of children per family the more likely the practice of contraception.[12-14] Respondents with the tertiary level of education(p=<0.001), semi-skilled workers (p=0.027), of the Christian religion (p=<0.001) and counselled on contraception during pregnancy(p=0.031) had statistically significant associations with good knowledge of contraception. This shows the importance of the antenatal and intrapartum counselling and that those with higher education more easily understands the information being passed. This may imply that adopting other forms of communication using visuals and local languages may help to endure better understanding among the women.
LIMITATION
The limitation of this study is that it did not assess the background knowledge of contraception and perception of the women before pregnancy as this could have helped in evaluating the contribution of counselling during pregnancy to the demonstrated good knowledge and the readiness to accept contraception postdelivery. It also assessed their readiness which may not necessarily translate to practice of contraception.
CONCLUSION
The results of this study demonstrated high knowledge and readiness to use any method of contraception among respondents but lower than 50% were ready to adopt a method on the day of discharge at postnatal clinic. This study also showed that the majority of respondents demonstrated positive attitude to contraceptive use and over half of the respondents had previously used a contraceptive method.
The antenatal and postnatal period provides an opportunity for family planning counselling. There is a need for the enactment of government policy and legislation that will ensure wide coverage and availability There is therefore the need for the enactment of government policy and legislation that will ensure of contraception counselling among pregnant women or women of reproductive age group across all levels of healthcare. Additionally, training and retraining of health care workers to ensure appropriate and updated counseling of women will be helpful to enhance the willingness to use contraceptives.
ACKNOWLEDGEMENTS
We acknowledge the contributions of the participants who consented to this study, and the nursing staff and doctors at the Adeoyo Maternity Teaching Hospital, Yemetu, Ibadan and the University College Hospital, Ibadan, for their co-operation during this study.
AUTHORS CONTRIBUTION
Temitope Azeez Olukunle (TAO), Olayinka Oladunjoye Ogunbode (OOO) and Rukiyat Adeola Abdus-salam (RAA) had substantial contributions to the conception, design, acquisition of data, data analysis and interpretation of data. TAO, OOO and RAA also contributed to the drafting, revising and approval of this manuscript.
CONFLICTS OF INTEREST:
Authors declared they have no conflicts of interest.
FUNDING
This study was self-sponsored by the authors.
REFERENCES
- World Health Organization (WHO). Programming strategies for postpartum family planning. WHO 2013 ISBN :97892 4150649. https://www.who.int/publications/i/item/9789241506496
- Nibret Mihretie G, Simegn A, Dereje A, Gebrehana H, Getie A, Getnet B, Degu A. Postpartum Modern Contraceptive Utilization and Associated Factors Among Women Who Gave Birth in the Last 12 Months in Addis Zemen, South Gondar, Ethiopia: Community-Based Cross-Sectional Study. Int J Womens Health. 2020 Dec 24; 12:1241-1251. https://www.dovepress.com/getfile.php?fileID=65161
- Monjok E, Smesny A, Ekabua JE, Essien E.J. Contraceptive Practices in Nigeria. Literature review and Recommendation. Dove Medical Press. 2010; 1:9-22. https://www.dovepress.com/getfile.php?fileID=6243
- Family Planning Data Sheet. Population Reference Bureau USA.2019.
- Ali AA, Okud A. Factors affecting unmet need for family planning in Eastern Sudan. BMC Public Health. 2013; 13(102): 1- 5.
- World Family Planning 2020 Highlights: Accelerating action to ensure universal access to family planning. United Nations Department of Economic and Social Affairs, Population Division, United Nations, New York. 2020; 1-46.
- Oye-Adeniran BA, Adewole IF, Umoh AV, Oladokun A, Badagesin A, Ekanem EE, Et al. Community based study of contraceptive behaviour in Nigeria. Afri J Reprod Health.2006; 10:90–104.
- National Population Commission [Nigeria] and ICF. Nigeria Demographic and Health survey 2018. Abuja, Nigeria, and Rockville, Maryland. USA: NPC and ICF International.2019. https://dhsprogram.com/pubs/pdf/FR359/FR359.pdf
- Brown W, Druce N, Bunting J, Radloff S, Korona D, Gupta S, Etal. Developing the “120 by 20” Goal for the Global FP 2020 Initiative.2014.
- Singh, S., Darroch J. Adding it all up: The cost and benefits of investing in family planning - estimates for 2012 New York: Guttmacher Institute and United Nations Fund for Population Activities.2012. https://www.guttmacher.org/sites/default/files/pdfs/pubs/AIU-2012-estimates.pdf
- WHO: Programming strategies for postpartum family planning. ISBN 978 92 4 150649 6 (NLM classification: WA 550). Geneva: World Health Organization. 2013. https://www.who.int/publications/i/item/9789241506496
- Adedokun B, Abdus Salam RA, Babawarun T, Morhason Bello I, Ojengbede O. Resumption of Sexual Intercourse and Family Planning use Among Postpartum Women Attending Infant Welfare Clinics in Ibadan, Southwest Nigeria – A Cross Sectional Study. Nigerian Journal of Clinical Practice. 2021. 23(12) :1648-1655
- Anaba R, Ugwa EA, Agbor IE, Nwali MI, Orji B. Knowledge, Attitude, and Contraceptive Preferences Among Postpartum Women in Izzi, Ezza South, and Ikwo Local Government Areas of Ebonyi State, Nigeria. Hospital Practices and Research. 2018; 3(1):11-15.
- Mruts KB, Tessema GA, Gebremedhin AT, Scott JA, Pereira G. The role of family planning counselling during maternal and child health services in postpartum modern contraceptive uptake in Ethiopia: A national longitudinal study. PLOS Glob Public Health. 2022; 2(8): 1- 15.
- Chandra-Mouli V, Akwara E. Improving access to and use of contraception by adolescents: What progress has been made, what lessons have been learnt, and what are the implications for action?, Best Practice & Research Clinical Obstetrics & Gynaecology. 2020; 66: 107-118.
- Ogbonna C, Pam IC. Postpartum contraception: A study of a cohort of nursing mothers in Jos University Teaching Hospital, Jos, Plateau State. Nig Q J Hosp Med.1999, 9:293–5.
- World Health Organization. Medical Eligibility Criteria for Contraceptive Use, 5th edition, 2015.
- Araoye, M. Subjects Selection. in Research methodology with statistics for health and social sciences Nathadex Publishers 2004: 115–29.
- Akinlo A, Bisiriyu A, Esimai O. Use of maternal health care as a predictor of postpartum contraception in Nigeria. Afr Popul Stud. 2014;27(2):288-300. doi:10.11564/27-2-475.
- Blackstone SR, Iwelunmor J. Determinants of contraceptive use among Nigerian couples: evidence from the 2013 Demographic and Health Survey. Contracept Reprod Med. 2017; 2:9. doi:10.1186/s40834-017-0037-6. https://contraceptionmedicine.biomedcentral.com/articles/10.1186/s40834-017-0037-6
- Ogboghodo EO, Adam VY, Wagbatsoma VA. Prevalence and determinants of contraceptive use among women of child-bearing age in a rural community in southern Nigeria. Journal of Community Medicine and Primary Health Care. 2017;29(2):97-10.file:///C:/Users/yinka/Downloads/ajol-file-journals_221_articles_162455_submission_proof_162455-2629-420670-1-10-20171102.pdf
- Bajracharya A. Knowledge, Attitude and Practice of Contraception among Postpartum Women Attending Kathmandu Medical College Teaching Hospital. Kathmandu Univ Med J. 2015;52(4):292-7. https://pubmed.ncbi.nlm.nih.gov/27423277/
- Kaushal SK, Saxena SC, Srivastava VK, Gupta SC., Nigam S. KAP study on contraceptive methods in Kanpur district of UP. Indian Journal of Community Health. 2010 ;22(1): 33-38. https://iapsmupuk.org/journal/index.php/IJCH/article/view/164
- Sharma J, Dorairajan G, Chinnakali P. Knowledge and attitude towards contraceptive methods for spacing and decision-making factors regarding its use in postpartum women. Int J Reprod Contracept Obstet Gynecol. 2015; 4:750-4. https://www.ijrcog.org/index.php/ijrcog/article/view/1997
- Mao J. Knowledge, Attitude and Practice of Family Planning. A Study of Tezu Village, Manipur (India). Int J Biological Anthropol. 2006;1(1): 1-6.
- Gejo NG, Anshebo AA, Dinsa LH. Postpartum modern contraceptive use and associated factors in Hossana town. PLOS ONE. 2019;14(5): E0217167
- Gupta N, Sinha R, Mangal A. Knowledge, attitude and practice study on immediate postpartum intrauterine contraceptive device method of family planning. Int J Community Med Public Health. 2017; 4:2981-4. https://www.ijcmph.com/index.php/ijcmph/article/view/1544
- Britton LE, Alspaugh A, Greene MZ, McLemore MR. CE: An Evidence-Based Update on Contraception. Am J Nurs. 202;120(2):22-33.
- Ngome E, Odimegwu C. The social context of adolescent women's use of modern contraceptives in Zimbabwe: a multilevel analysis. Reprod Health. 2014; 11:64. https://reproductive-health-journal.biomedcentral.com/articles/10.1186/1742-4755-11-64
- Edmeades J, Pande R, Macquarrie K, Falle T, Malhotra A. Two sons and a daughter: sex composition and women's reproductive behaviour in Madhya Pradesh, India. J Biosoc Sci. 2012;44(6):749–64.
Medical Journal of Zambia, Vol 50, 3
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.