Gastrointestinal malignancies in Zambia: a scoping review.
Pharidah Rajan Ibrahim Omar Sundi
Lusaka Apex Medical University, Zambia.
Pan-African Organization for Health, Education and Research (POHER).
African Association of Future Gastroenterologists.
Nkengeh Tazinkeng
Pan-African Organization for Health, Education and Research (POHER).
African Association of Future Gastroenterologists.
Division of Gastroenterology, Massachusetts General Hospital, USA.
Lisa Liang Philpotts
Treadwell Library, Massachusetts General Hospital, USA.
Ayooluwatomiwa D. Adekunle
African Association of Future Gastroenterologists.
Division of Internal Medicine, St. Luke’s Hospital, Chesterfield MO.
Rodrigue Ndabashinze
Faculty of Medicine, University of Burundi.
Akwi W. Asombang
Pan-African Organization for Health, Education and Research (POHER).
African Association of Future Gastroenterologists.
Division of Gastroenterology, Massachusetts General Hospital, USA.
DOI: https://doi.org/10.55320/mjz.50.3.400
Keywords: Gastrointestinal cancer, Zambia, risk factors, management, clinical outcomes.
ABSTRACT
Background: Gastrointestinal (GI) malignancies account for greater than one-third of cancer-related deaths worldwide. In Zambia, there is a lack of data on epidemiology, diagnosis, management, and outcomes. We sought to review existing literature to determine the extent of research and identify gaps in knowledge pertaining to GI malignancies in Zambia.
Methods: We systematically searched databases including Ovid MEDLINE, CINAHL, Web of Science Core Collection, Cochrane Library via Ovid, Embase, Africa Wide Information via Ebsco, African Index Medicus and African Journals Online, to identify studies on GI malignancies including colorectal (CRC), pancreatic (PC), gastric (GC), esophageal (EC) and liver cancers (LC) in Zambia.
Results: Of 323 studies screened, 27 were included in the final analysis. The included studies assessed an individual GI cancer or more than one GI cancer as follows: GC only (n=10, 37%), EC only (n=5, 18%), LC only (n=5, 18%), CRC only (n=2, 7%), PC only (n=1, 4%), PC, CRC, EC, GC, LC combined (n=1, 4%), CRC, EC, GC, LC combined (n=1, 4%), CRC, EC, GC combined (n=1, 4%) and EC, GC combined (n=1, 4%). Gastric cancer was the most studied (n =14 articles), followed by esophageal (n=9 articles), liver cancer (n=7 articles), colorectal (n=5 articles) and pancreatic cancer (n=2 articles).
Conclusion: There is paucity of published data. Existing studies have focused mainly on prevalence and risk factors. Longitudinal studies examining incidence, prognosis and survival are needed.
INTRODUCTION
Gastrointestinal malignancies such as colorectal, gastric, pancreatic, liver, and esophageal cancers account for 35% of all cancer-related deaths and 26% of all cancer incidence worldwide [1-2] . In 2018, there were 3.4 million attributable fatalities and an estimated 4.8 million new cases across the globe[1] . Despite improvement in therapeutics over the past decade, survival rates remain suboptimal[3] . The observed increase in global incidence of gastrointestinal cancers has been attributed to factors such as lifestyle trends (alcohol and tobacco use), genetics, environmental exposures, diet and obesity[4] . In a prospective study evaluating the relationship between red and processed meat intake and cancer risk, Cross et al found that individuals with the highest red meat consumption had a systematically higher risk of colorectal, esophageal and liver cancers[5] . The consumption of processed meat was also associated with higher risk of colorectal cancer. In developing countries, the high associated mortality has been ascribed to factors including delays in referral and diagnosis, advanced stage at time of diagnosis as well as inadequate access to diagnostic and treatment facilities[6] .
In Zambia, a Southern African country with a total population of 19, 473, 1257, incidence and prevalence of GI cancers has been increasing, particularly among younger patients[8] . According to data from the Global Cancer Observatory, esophageal, liver and gastric cancers are among the top ten most prevalent cancers in Zambia with each having a cumulative 5-year prevalence of 3.09, 2.63 and 2.11 respectively per 100,000 population[9] . It is unclear if the increasing incidence and prevalence in recent years is attributable to an increase in occurrence of these cancers or simply a reflection of better detection. Data regarding this is sparse. There is generally a lack of understanding of the factors driving the observed trends in incidence and mortality of GI cancers in Zambia.
Research plays a significant role in understanding the carcinogenesis process, epidemiology, management and clinical outcomes. Results from published data can be applied towards policy development and public health measures. Public health measures to raise awareness amongst the general population and development of screening/surveillance guidelines rely on the availability of data on the burden of gastrointestinal cancers in Africa. The aim of our study is to assess the state of published data on gastrointestinal cancers in Zambia, Southern Africa and identify any potential gaps in research and recommend areas that need focus.
METHODS
Information Sources and Search Strategy
A comprehensive search for relevant published articles on gastrointestinal cancers in Zambia from inception to 31st March 2022 was conducted by a medical librarian (LP) using several databases including: Ovid MEDLINE, CINAHL, Web of Science Core Collection, Cochrane Library via Ovid, Embase, Africa Wide Information via Ebsco, African Index Medicus and African Journals Online. The search combined keywords and controlled vocabulary for two concepts: Zambia and gastrointestinal cancers. The full search strategies are available in Appendix 1. No language, study type, or date limits were incorporated into the database search strategies.
The search included the use of a combination of relevant keywords. The keywords were used individually or in combination to search for cancer-related publications in English and index terms with appropriate Boolean operators (AND/OR). Medical Subject Headings (MeSH) terms or subject heading in all fields was included, and syntax was modified appropriately for each database if necessary to identify all relevant studies.
Study Selection and Eligibility Criteria
The database search, which initially focused on the titles of the articles and adhering to the inclusion and exclusion criteria was conducted by LP. Potentially relevant articles were exported to Covidence, and duplicates were removed. Two independent reviewers then conducted abstracts and full article screening. Disputes arising between the two reviewers were resolved by a third reviewer. Studies were included if they reported quantitative data on the epidemiological burden (morbidity, incidence, prevalence, and mortality) risk factors, diagnosis, economic burden, and management of the esophageal, gastric, colorectal, pancreatic, liver, and biliary tract cancers in Zambia (including multinational studies that included Zambia). Eligible study designs included case-control, cross-sectional, cohort, randomized controlled trials (RCTs), and case series with a minimum of 10 patients.
We excluded studies not reported in English, non-human studies, abstract-only studies, review articles, comments, editorials, opinions, case reports, and studies whose abstract or full text were unavailable 2 months after an inter-library request was made.
Data Extraction
A data collection form designed by the team was used to extract relevant information from included studies. The following information was extracted from each study: title, surname of the first author, year of publication, country, aim, study design, study setting, sample size, age and gender of the targeted group, type of GI cancer studied, incidence, age standardized incidence rate (ASIR), case fatality rate (CFR), prevalence, risk factors, diagnosis (including screening methods), management, and outcomes (survival, mortality) and any other quantitative findings.
RESULTS
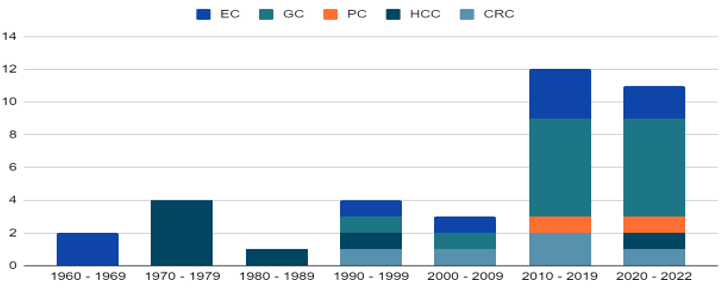
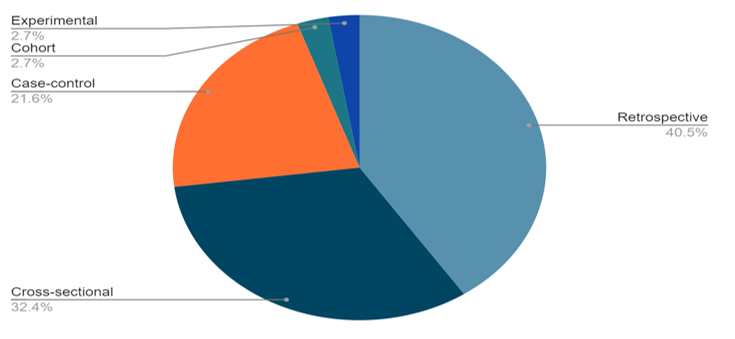
A total of 323 studies were initially identified through database searching, of which 171 duplicates were removed and the remaining 152 studies were reviewed by title and abstract. Eighty-eight studies were irrelevant, and 64 studies were further evaluated for full-text eligibility. Of these, 37 studies were ineligible and 27 studies were eligible for data synthesis. The 27 studies used for data synthesis included studies that assess an individual GI cancer or more than one GI cancer as follows: GC only (n=10, 37%), EC only (n=5, 18%), LC only (n=5, 18%), CRC only (n=2, 7%), PC only (n=1, 4%), PC, CRC, EC, GC, LC (n=1, 4%), CRC, EC, GC, LC (n=1, 4%), CRC, EC, GC (n=1, 4%) and EC, GC (n=1, 4%). The earliest GI cancer related publication from Zambia was study on the radiological appearances of esophageal carcinoma in Zambians, published by Khurana et al in 1967. According to decades most full-text articles on GI cancers in Zambia were published between 2010 - 2019 (Figure 1). Analysis by cancer type showed that the most studied GI cancers were gastric cancer (n=14 articles), esophageal cancer (n=9 articles), liver cancer (n=7 articles), colorectal cancer (n=5) and pancreatic cancer (n=2 articles). The most common study designs were Retrospective (n=12), cross-sectional (n =8), case-control (n=6), cohort (n=1), non-randomized experimental (n=1). (Figure 2)
Colorectal cancer
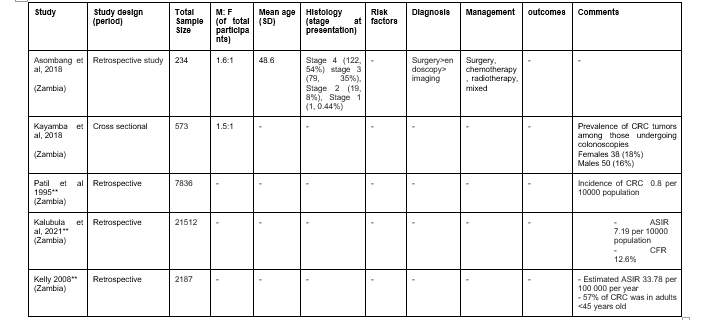
There was a total of 5 published studies on CRC; 4 retrospective studies and 1 cross-sectional study. (Table 1) CRC was more common in males than females in both studies that compared gender distribution of CRC[10-11] . Age-standardized incidence rate of CRC was reported across three studies; 0.8 per 100,000 in 1995, 33.78 per 100,000 in 2008 and 7.19 per 100,000 in 2021 [12-14] . Only two studies report age distribution of CRC cases[10-14] . A study by Asombang et al reported the mean age of CRC in Zambia at 48.6 years while another study by Kelly et al. reported that 57% of CRC was found in adults <45 years old. Only one study comprehensively evaluated the clinical profile of CRC patients in Zambia[10] . In this study, most patients presented at stage 4 of disease. Majority of patients were diagnosed through surgery, with a smaller proportion being diagnosed using endoscopy or imaging. Management options included surgery, chemotherapy, and radiotherapy. In a study published by Kayamba et al in 2018, 18% of females and 16% of males presenting for colonoscopy were diagnosed with CRC[11] . No studies conducted in Zambia have assessed risk factors of colorectal cancer and the clinical outcomes of CRC such as survival and mortality.
Esophageal cancer
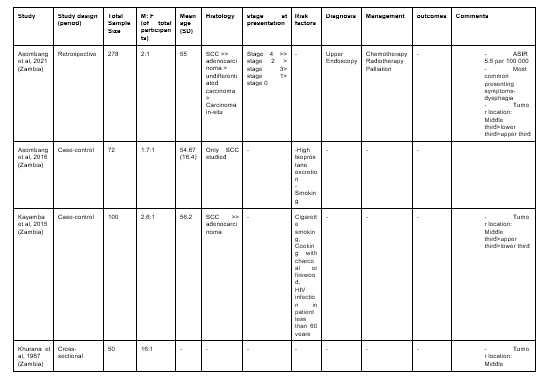
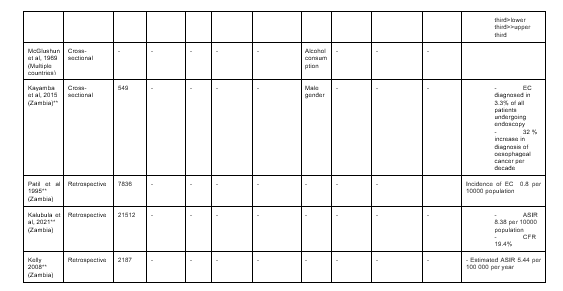
A total of nine full-text articles published data on esophageal cancer in Zambia (Table 2). Of these, 4 were retrospective studies, 3 Cross-sectional studies, and 2 case-control studies. Age-standardized incidence rate of EC has been on the rise in Zambia; 0.8 per 100,000 in 1995, 5.44 per 100 000 in 2008, 5.5 - 8.38 per 100 000 in 2021[12-15] . The mean age of EC observed in three studies, lies between 54 - 57 years [15-17] . All four studies that evaluated gender distribution of EC showed a higher prevalence in males than females[15-18] . Squamous cell carcinoma was the most common histopathological subtype of EC in Zambia, followed by adenocarcinoma[15-17] . In majority of patients, diagnosis was made by upper endoscopy and histopathology[15] . Staging revealed that most patients presented at stage 4 of the disease[15] . Across all three studies describing tumor location, most esophageal tumors were found in the middle third of the esophagus[15,17,18] . The lower third was the second most common site in two studies and the least common site in one study. The upper third was the second most common site in one study and the least common site in two studies. Treatment options for EC patients in Zambia included chemotherapy, radiotherapy and palliative care[15] . The case fatality rate of EC in Zambia was 19.4%[13] . Four studies assessed the risk factors of EC in Zambia[16,17,19,20] . Risk factors include, smoking, alcohol consumption, cooking with charcoal or firewood, high Isoprostane excretion, HIV infection in patients less than 60 years, and male gender. A study by Kayamba et al in 2015, reported that EC was diagnosed in 3.3% of all patients undergoing upper endoscopy, and that there is a 32 % increase in diagnosis of esophageal cancer per decade in Zambia[20] . There were no studies on the mortality and survival rates for EC in Zambia.
Gastric Cancer
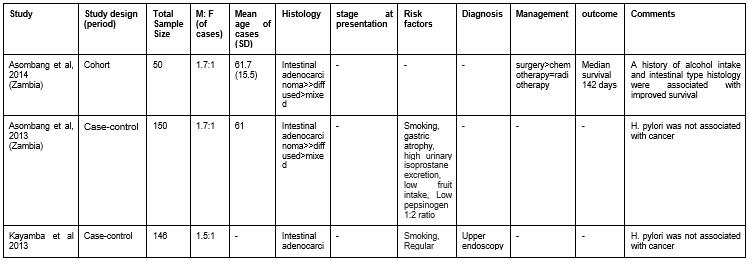
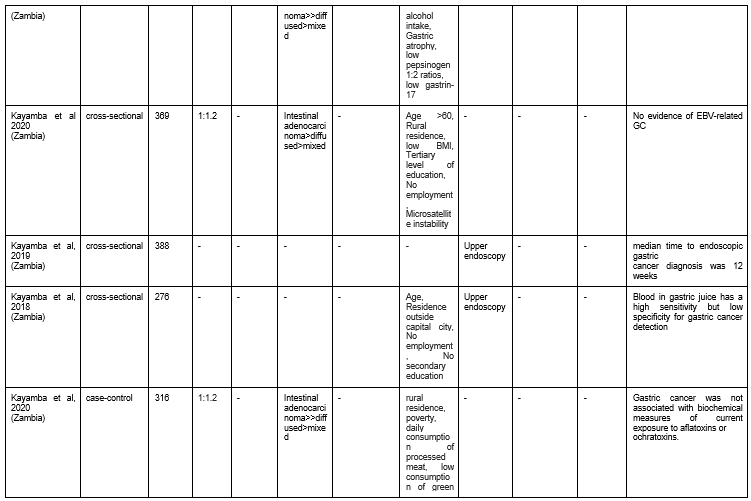
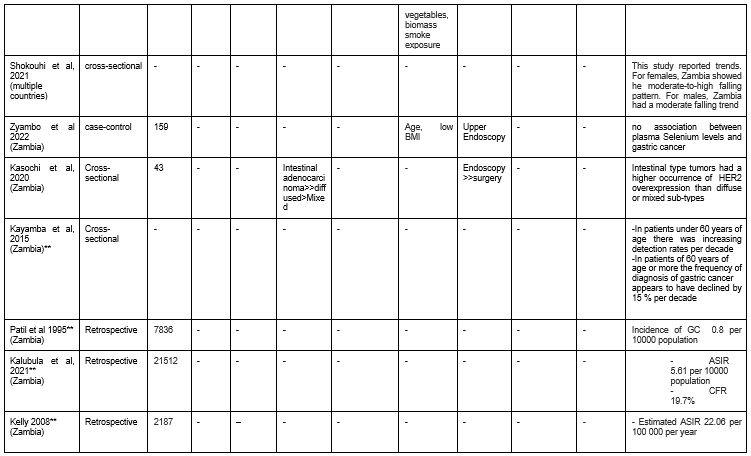
A total of 14 full-text articles published data on gastric cancer in Zambia (Table 3). This included 6 Cross-sectional studies, 4 case-control studies, 3 retrospective studies, and 1 cohort study. Age-standardized incidence rate of GC was reported in three studies: 0.8 per 100000 populations in 1995, 22.06 per 100 000 in 2008, and 5.61 per 100 000 populations in 2021[12-14] . The mean age of GC reported in two studies by Asombang et al was 61 years. Six studies reported similar findings on the histopathological subtypes of gastric cancer, using the Lauren classification. Intestinal adenocarcinoma made up the greatest proportion of gastric cancers, with a smaller proportion being diffused or mixed type GC[21-26] . Upper GI endoscopy was the most common mode of diagnosis seen in five studies[6,23,26,28] . In a study by Kayamba et al in 2018, blood in gastric juice was found to have a high sensitivity but low specificity for gastric cancer detection[27] . A single study looked at the management and outcomes of GC in Zambia[21] . In this study by Asombang et al, most GC patients were treated surgically and the median survival for GC was 142 days. They also observed that the intestinal type histology was associated with improved survival. Six studies described risk factors of GC in Zambia[22,25,27,28] . Risk factors of GC in Zambia include: smoking, alcohol consumption, low consumption of fruits and vegetables, gastric atrophy, age > 60 years, low socioeconomic status (poverty, unemployment, rural residence), low body mass index (BMI), Low pepsinogen 1:2 ratio, high urinary isoprostane excretion, low gastrin-17, and microsatellite instability. Two studies observed no significant association between H. pylori infection and gastric cancer[22-23] . In a study by Kayamba et al in 2019, median time to endoscopic gastric cancer diagnosis was 12 weeks from onset of symptoms. No study on GI cancers in Zambia mentioned the stage of disease at diagnosis.
BMI - Body Mass Index
Liver Cancer
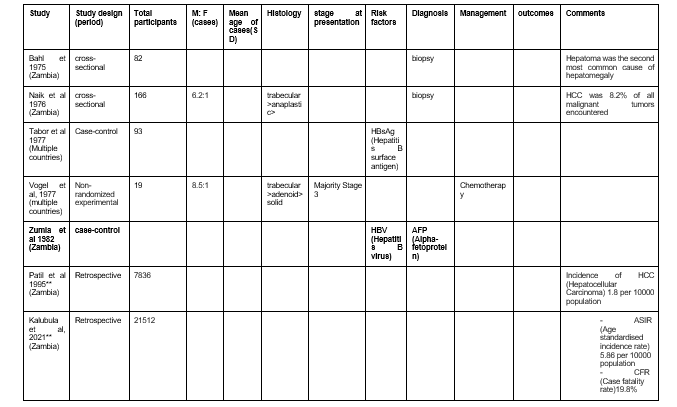
There was a total of 7 studies published on liver cancer in Zambia; two cross-sectional studies, 2 retrospective studies, 2 case-control studies, and 1 non-randomized experimental study. (Table 4) Age-standardized incidence rate of LC was reported in two studies; 1.8 per 100, 000 population in 1995 and 5.86 per 100 000 population in 2021[12-13] . Two studies reported the gender distribution of liver cancer in Zambians[29-30] . Males were at least six times more affected by liver cancer than females. The most common histopathological subtype of LC was the trabecular type[29-30] . Diagnosis of LC was made by biopsy and alpha fetoprotein levels[30-32] . Most cases of LC were diagnosed at stage 3 and treated with chemotherapy[30] . Hepatitis B infection was the main risk factor of LC in 2 studies[32-33] . No studies conducted in Zambia have assessed the clinical outcomes of LC in Zambia.
Pancreatic cancer
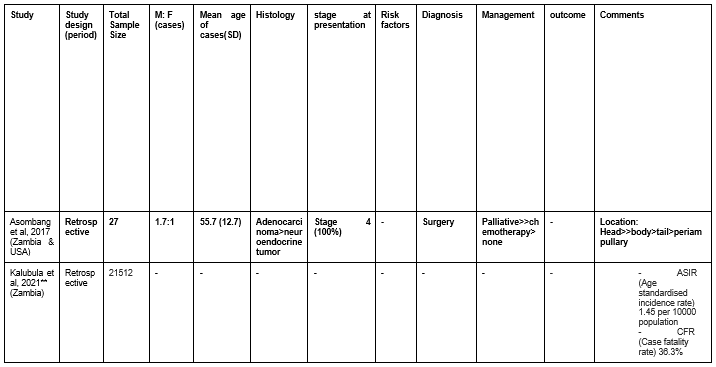
There were two published studies on PC, both retrospective studies (Table 5). In a study by Asombang et al, Pancreatic cancer was more common in males than females[34] . The mean age (SD) of patients with PC at the time of diagnosis was 55.7 (12.7). All patients were diagnosed at stage 4, and pancreatic adenocarcinoma was the most common histopathological subtype. Most tumors were found in the head of the pancreas, followed by the body, tail and peri-ampullary. Majority of patients were diagnosed via surgery and received palliative care. In a second study by Kalubula et al, the ASIR of PC was 1.45 per 100 000 populations and the case fatality rate (CFR) was 36.3%[13] . No studies conducted in Zambia have assessed risk factors of pancreatic cancer and clinical outcomes such as survival and mortality.
DISCUSSION
GI cancers impose a significant medical and financial burden globally. Publications on gastrointestinal cancers in Zambia are scarce. Efforts directed at increasing cancer research are hampered by several obstacles throughout the continent, such as a lack of infrastructure, trained personnel, and research funding[35] . Africa has very few active researchers and a deficit of skilled healthcare workers due to immigration to more developed countries[36] .
This study highlights the extent of gastrointestinal research in Zambia has focused on prevalence, risk factors, symptoms, potential screening methods, treatment modalities, and outcomes. Dietary patterns are significantly associated with all GI cancers in Zambia. Therefore, dietary and lifestyle modifications could potentially reduce risk of GI malignancies[37] . A study by Liu et al, evaluated the trends in the incidence of primary liver cancer caused by different etiologies and found a negative trend in nations with high socio-demographic indices, indicating that targeted strategies needed to be established[38] . Chronic Hepatitis B virus (HBV) infection is the main cause of liver cancer in Sub-Saharan Africa. Several additional exposures to aflatoxin B1, co-infection with human immunodeficiency virus (HIV) and alcohol use are common and may exacerbate the risk in HBV-infected individuals[39] . Hepatitis C virus (HCV), non-alcoholic steatohepatitis/non-alcoholic fatty liver disease (NASH/NAFLD) are other leading causes[40] .
Examining the epidemiology, risk factors, classification, genomic traits, and treatment approaches in a study found the development and occurrence of gastric cancer to be a multifactorial disease that was influenced by both environmental and genetic factors[41] . The mean age of patients with GC at the time of diagnosis, which increased steadily with age, was 61 years[21-22] . Lyons K et al, evaluated the clinical and environmental factors that affected the prevalence of gastric cancer and covered the various intervention strategies that could be used to not only raise awareness of the disease but also increase screening in an effort to lower the risk[42] . The main risk factor was Helicobacter pylori infection. Geographical location, age, sex, smoking, socioeconomic status, dietary habits, and genetics were additional risk factors. The risk of gastric cancer can be decreased through primary and secondary prevention methods like dietary changes and screenings. Interventions with some promise as a preventive measure include the elimination of H. pylori through chemoprevention studies[42] .
Globally, colorectal cancer is the third most common cancer in women and the fourth most common cancer in men. There is limited data regarding colorectal cancer in Zambia and sub-Saharan Africa due to recognized challenges of the database that result in incomplete or lower reported data[10] .
When the endoscopic service originally started, in 1977, healthcare in Zambia was completely subsidized by the government and provided free at the point of care. Cost-sharing user fees were implemented at government hospitals after 1991, when the majority of the state's assets were being privatized and the economy could no longer afford universal, free healthcare[20] .Currently children, the elderly and immunocompromised (HIV seropositive, TB) receive free medical care and all diagnostic services attractive fees. Endoscopy presently costs 150 Zambian Kwacha (approximately USD 22), which a significant barrier to investigation is given that 60.5% of Zambia's population lives in poverty and can hardly afford it[20] .
Over the past forty years, there has undoubtedly been a change in public perception of the endoscopic service, which may contribute to the increased prevalence of esophageal cancer diagnosed. Awareness of the endoscopy services across the nation has certainly changed and this may explain the raising diagnostic rate[20] . Increased cancer research is essential for addressing the existing and anticipated rise in the cancer burden as well as serving as the basis for the creation and effective use of evidence-based approaches to disease prevention and control. However, efforts to increase the production of cancer research are hampered across the continent by issues such as a lack of infrastructure, qualified employees, research funding, and the constantly rising demand for limited resources[43] . Training and financing for cancer research have not always been given primary attention.
However, there is promise for improving cancer research in Africa as a number of domestic and foreign partners are working in this direction. One illustration is the African Organization for Research and Training in Cancer. African Organization for Research and Training in Cancer was founded to increase cancer research in Africa, advance oncology training programs, assist African oncology research, and address the difficulties of developing effective cancer prevention campaigns to raise Awareness[44] . In addition, a number of international funding organizations have made appeals for promoting cancer research in Africa, particularly among early career researchers[45] . Training and financing for cancer research have not historically been top priority for many African nations. However, there are instances of nations that have just started implementing national research funding programs[46] .
The issue of competent employees relocating to more developed areas is still a problem in Africa, where there is a lack of clinical researchers[36] . Therefore, there is need to curb the African brain drain, several funding mechanisms are set up to encourage skilled African researchers to accept positions in institutions in their home countries and contribute to improving local capacity[47] . Another tactic that has been successful in increasing the retention of African graduates is funding research training at African institutions[48] . Journals specializing in oncology in global health have emerged, including the ASCO's JCO Global Oncology, to promote cancer manuscripts from low resource countries[49] .
Limitations encountered in this study were that some studies could not be retrieved due to a lack of full-text, and we only included studies that were in English which makes it possible that some non-English Studies were omitted. We analyzed gastrointestinal cancers publications in Zambia, our review does draw attention to the relatively low output of cancer-related research showing the need to employ deliberate efforts aiming at encouraging and facilitating cancer publications in Zambia.
CONCLUSION
In conclusion, this review highlighted the gaps in GI cancer research in Zambia. Future research should examine the barriers to research in Zambia. The authors suspect the limited funding of non-HIV-related research to be one of these barriers.
ACKNOWLEDGEMENTS
We would like to acknowledge the help of Mouhand Mohamed in providing inputs for the first draft of our manuscript.
Competing interests
All authors declare no conflict of interests.
Authors’ contributions
Protocol development: Pharidah Rajan Ibrahim Omar Sundi, Lisa Philpots, Nkengeh Tazinkeng, Rodrigue Ndabashinze Akwi Wasi Asombang. Data collection analysis and interpretation: Pharidah Rajan Ibrahim Omar Sundi, Lisa philpots, Nkengeh Tazinkeng, Rodrigue Ndabashinze, Ayooluwatomiwa D. Adekunle and Akwi Wasi Asombang. Manuscript writing and approval of final draft: Pharidah Rajan Ibrahim Omar Sundi, Lisa philpots, Nkengeh Tazinkeng, Rodrigue Ndabashinze, Ayooluwatomiwa Deborah Adekunle and Akwi Wasi Asombang
All the authors have read and agreed to the final manuscript.
REFERENCES
- Arnold M, Abnet CC, Neale, RE et al. Global burden of 5 major types of gastrointestinal cancer. Gastroenterology. 2020; 159(1), pp.335-349
- Pourhoseingholi MA, Vahedi M and Baghestani AR. Burden of gastrointestinal cancer in Asia; an overview. Gastroenterology and hepatology from bed to bench. 2015; 8(1), p.19.
- Marusawa H, Jenkins BJ. Inflammation and gastrointestinal cancer: an overview. Cancer letters. 2014; 345(2), pp.153-156.
- Kayamba V, Heimburger, DC, Morgan DR, Atadzhanov M. and Kelly P. Exposure to biomass smoke as a risk factor for oesophageal and gastric cancer in low-income populations: A systematic review. Malawi Medical Journal. 2017; 29(2), pp.212-217.
- Cross AJ, Leitzmann MF, Gail MH, Hollenbeck AR, Schatzkin A. and Sinha R. A prospective study of red and processed meat intake in relation to cancer risk. PLoS medicine 2007; 4(12), p. e325.
- Kayamba V, Kelly P. Delayed referral for diagnostic endoscopy is a contributing factor to late gastric cancer diagnosis in Zambia. The health press. 2019; 3(2), p.14.
- The World Bank: Bank website to get population data for individual African countries. https://www.imf.org/en/Publications/SPROLLs/world-economic-outlook-databases#sort=%40imfdate%20descending.
- Kayamba V, Asombang AW, et al. Gastric adenocarcinoma in Zambia: a case-control study of HIV, lifestyle risk factors, and biomarkers of pathogenesis. S Afr Med J. 2013 19; 103(4):255-9. PMID: 23547703
- Sung, H, Ferlay J, Siegel RL et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians 2021; 71(3), pp.209-249.
- Asombang AW, Madsen R, Simuyandi M et al. Descriptive analysis of colorectal cancer in Zambia, Southern Africa using the national cancer disease hospital database. The Pan African Medical Journal. 2018; 30.
- Kayamba V, Nicholls K, Morgan C and Kelly P. A seven-year retrospective review of colonoscopy records from a single centre in Zambia. Malawi medical journal. 2018; 30(1), pp.17-21.
- Patil P, Elem B and Zumla A. Pattern of adult malignancies in Zambia (1980-1989) in light of the human immunodeficiency virus type 1 epidemic. The Journal of Tropical Medicine and Hygiene.1995; 98(4), pp.281-284.
- Kalubula M, Shen H, Makasa M and Liu L. Epidemiology of cancers in Zambia: a significant variation in cancer incidence and prevalence across the nation. Malawi Medical Journal. 2021; 33(3), pp.186-195
- Kelly P, Katema M, Amadi B et al. Gastrointestinal pathology in the University Teaching Hospital, Lusaka, Zambia: review of endoscopic and pathology records. Transactions of the Royal society of Tropical Medicine and Hygiene. 2008; 102(2), pp.194-199.
- Asombang AW, Kasongo N, Muyutu J et al. Descriptive analysis of esophageal cancer in Zambia using the cancer disease hospital database: young age, late stage at presentation. Pan African Medical Journal. 2021; 39(1).
- Asombang AW, Kayamba V, Lisulo MM et al. Esophageal squamous cell cancer in a highly endemic region. World Journal of Gastroenterology. 2016; 22(9), p.2811.
- Kayamba V, Bateman AC, Asombang AW et al. HIV infection and domestic smoke exposure, but not human papillomavirus, are risk factors for esophageal squamous cell carcinoma in Zambia: a case–control study. Cancer medicine. 2015; 4(4), pp.588-595.
- Khurana KM. A radiological study of carcinoma of the oesophagus. Central African Journal of Medicine.1967; 13(3), pp.62-64.
- McGlashan, ND. Nitrosamines in South African drinks in relation to esophageal cancer. South African medical journal= Suid-Afrikaanse tydskrif vir geneeskunde. 1969; 43(25), p.800.
- Kayamba V, Sinkala E, Mwanamakondo S et al. Trends in upper gastrointestinal diagnosis over four decades in Lusaka, Zambia: a retrospective analysis of endoscopic findings. BMC gastroenterology. 2015; 15(1), pp.1-9.
- Asombang AW, Kayamba V, Turner-Moss E et al. Gastric malignancy survival in Zambia, Southern Africa: A two year follow up study. Medical Journal of Zambia. 2014; 41(1), pp.13-18.
- Asombang AW, Kayamba V, Mwanza-Lisulo M et al. Gastric cancer in Zambian adults: a prospective case-control study that assessed dietary intake and antioxidant status by using urinary isoprostane excretion. The American of Clinical Nutrition. 2013; 97(5), pp.1029-1035.
- Kayamba V, Asombang AW, Mudenda V et al. Gastric adenocarcinoma in Zambia: a case-control study of HIV, lifestyle risk factors, and biomarkers of pathogenesis. South African Medical Journal. 2013; 103(4), pp.255-259.
- Kayamba V, Zyambo K, Mulenga C et al. Biomass smoke exposure is associated with gastric cancer and probably mediated via oxidative stress and DNA damage: a case-control study. JCO Global Oncology. 2020; 6, pp.532-541.
- Kayamba V, Butt J, Waterboer T et al. Molecular profiling of gastric cancer in a population with high HIV prevalence reveals a shift to MLH1 loss but not the EBV subtype. Cancer Medicine. 2020; 9(10), pp.3445-3454.
- Kasochi C, Julius P, Mweemba I and Kayamba V. Human epidermal growth factor receptor 2 overexpression in gastric and gastroesophageal junction adenocarcinoma in patients seen at the University Teaching Hospital, Lusaka, Zambia. African Health Sciences. 2020; 20(4), pp.1857-64.
- Kayamba V, Zyambo K and Kelly P. Presence of blood in gastric juice: A sensitive marker for gastric cancer screening in a poor resource setting. Plos one. 2018; 13(10), p. e0205185.
- Zyambo K, Kelly P and Kayamba V. Evaluation of the association between gastric cancer and plasma selenium in Zambian adults: a case–control study. 2022; ecancermedicalscience, 16.
- Naik KG. Primary carcinoma of the liver in Zambia. Med J Zambia. 1976 Dec-1977 Jan; 10(6):146-51. PMID: 190819.
- Vogel CL, Bayley AC, Brooker RJ, Anthony PP and Ziegler JL. A phase II study of Adriamycin (NSC 123127) in patients with hepatocellular carcinoma from Zambia and the United States. Cancer. 1977; 39(5), pp.1923-1929.
- Bahl V, Mistry CM and Obineche EN. Hepatomegaly in Lusaka. Medical Journal of Zambia. 1975; 9(5), pp.135-137.
- Zumla A and Voller AA. Serological study on Primary Hepatocellular Carcinoma in Zambia. Transactions of the Royal Society of Tropical Medicine and Hygiene. 1982; 76(4), pp.546-551.
- Tabor E, Gerety RJ, Vogel CL et al. Hepatitis B virus infection and primary hepatocellular carcinoma. Journal of the National Cancer Institute. 1977; 58(5), pp.1197-1200.
- Asombang AW, Madsen R, Simuyandi M et al. Pancreatic cancer: Patterns in a low-to middle-income population, Zambia. Medical Journal of Zambia. 2017; 44(4), pp.212-217.
- Adewole I, Martin DN, Williams MJ, et al. Building capacity for sustainable research programmes for cancer in Africa. Nat Rev Clin Oncol. 2014; 11:251-259
- Simpkin V, Namubiru-Mwaura E, Clarke L, et al. Investing in health R&D: Where we are, what limits us, and how to make progress in Africa. BMJ Glob Health. 2019; 4: e001047
- Xie Y, Shi L, He X and Luo Y. Gastrointestinal cancers in China, the USA, and Europe. Gastroenterology Report. 2021; 9(2), pp.91-104
- Liu Z, Jiang Y, Yuan H et al. The trends in incidence of primary liver cancer caused by specific etiologies: results from the Global Burden of Disease Study 2016 and implications for liver cancer prevention. Journal of hepatology. 2019; 70(4), pp.674-683.
- Riebensahm C, Chitundu H, Muula G et al. Screening for hepatocellular carcinoma among adults with HIV/HBV co-infection in Zambia: a pilot study. International journal of infectious diseases. 2022; 116, pp.391-396.
- Choi S, Kim BK, Yon DK et al. Global burden of primary liver cancer and its association with underlying aetiologies, sociodemographic status, and sex differences, 1990-2019: a DALYs-based analysis of the Global Burden of Disease 2019 study. Clinical and Molecular Hepatology. 2019
- Machlowska J, Baj J, Sitarz M, Maciejewski R and Sitarz R. Gastric cancer: epidemiology, risk factors, classification, genomic characteristics and treatment strategies. International journal of molecular sciences. 2020; 21(11), p.4012.
- Lyons K, Le LC, Pham YTH et al. Gastric cancer: epidemiology, biology, and prevention: a mini review. European Journal of Cancer Prevention. 2019; 28(5), pp.397-412.
- Kayamba V, Mutale W, Cassell H, Heimburger DC and Shu XO. Systematic review of cancer research output from Africa, with Zambia as an example. JCO global oncology. 2021; 7, pp.802-810.
- African Organisation for Research and Training in Cancer: African organization for research and training in cancer https://aortic-africa.org.
- Vogel AL, Freeman JA, Duncan K, et al. Advancing cancer research in Africa through early-career awards: The BIG Cat Initiative. J Glob Oncol 5:1-8, 2019
- Karikari TK, Amoateng P: Kenya and Ghana set up national research funding schemes. Nature 557:166, 2018
- IIE: Carnegie African diaspora fellowship programme. https://www.iie.org/Programs/Carnegie-African-Diaspora-Fellowship-Program/How-to-Apply/Types-of-Fellowships.
- Mutale W, Nzala S, Cassell HM, et al: HIV research training partnership of the University of Zambia and Vanderbilt University: Features and early outcomes. Ann Glob Health 85:129, 2019
- JCO Global Oncology. https://ascopubs.org/go/about/about-go
Medical Journal of Zambia, Vol 50, 3
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.