Body Packer Syndrome: a case report on the health hazard of deglutitioned controlled drugs
K Saasa
GP and HIV/Aids Consultant.
MSS Patel
Consultant Pathologist.
DOI: https://doi.org/10.55320/mjz.50.1.397
Keywords:body packer syndrome, drug courier, drug trafficking, drug deglutition, drug death
ABSTRACT
A case of an accidental overdose in a body packer or drug courier is reported. It highlights a health hazard of deglutitioned controlled drugs. A clinicopathological aspect of the body packer syndrome is discussed.
INTRODUCTION
A thriving black market makes drug trafficking a major dilemma for law enforcing agents[1] . Drug couriers are undeterred by criminality or airport security and take grave personal risks for lucrative pecuniary gains.
There are international statutes governing surveillance of controlled drugs to prevent drug trafficking from prospering. In Zambia, illicit production, supply and possession of controlled drugs is prohibited and carries applicable penalties. There is also provision for prevention of drug abuse, treatment and rehabilitation of offenders.
Opium is a narcotic drug derived from dried poppy plant juice (papaver somniferum) which also contains other natural alkaloids such as morphine, codeine and papaverine from which heroin (diacetyl morphine) and hydrocodeine can be synthesised[2] . Heroin is well absorbed parenterally but unlike morphine it is readily taken up from gastrointestinal tract[3] . It is rapidly hydrolysed to 6-monoacetyl morphine and converted to morphine which activates a toxic pharmacological event.
Heroin which is abused is mostly nonpharmaceutical and imported as crude opium base for modification as heroin in an intermediate country. It is thereafter exported worldwide, including Africa in heavily cut form of concentrated drug.
CASE REPORT
A middle aged African had come to Europe a few days prior to his death. He was found lifeless in bed by the hotel manager who became concerned when there was no response to incoming telephone calls. A hotel cleaner had been to the room several hours earlier but presumed that the deceased was asleep.
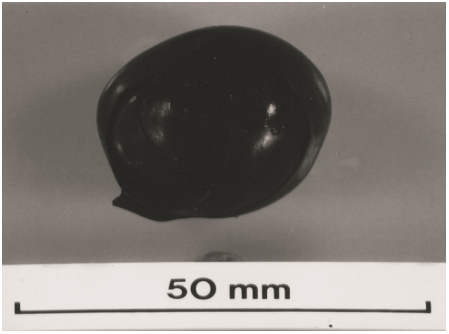
The Police were informed and a search of the sceneof-death revealed a single rolled ball of black insulating tape (Figure 1). It was next to the body and imparted a faecal smell. A clear plastic bag containing brownish powder was found in a pocket of his jacket.
A quantity of laxative suppositories was discovered among his belongings. It was suspected to have been for inducing defaecation to retrieve controlled drugs concealed in alimentary canal.
A thanatopsy showed early postmortem decomposition. There were no external characteristic signs of drug abuse. The gastric contents showed partially digested meal mixed with forty 2.5cm sized balls of black insulating tape containing a clear plastic bag holding brownish powder (Figure 2).
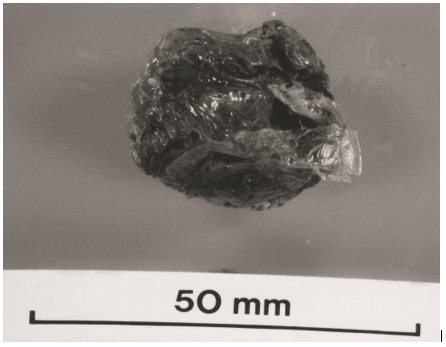
A couple of the packages had burst and several others had some unravelled insulating tape. There were no packages found distally beyond the stomach.
The lungs showed deep congestion and gross pulmonary oedema. There was hepatic steatosis but other organs were unremarkable and showed nonspecific visceral congestion.
A toxicological analysis showed lethal concentration of free blood morphine (1.8µg/ml) which is in the upper range of heroin fatalities. Acetyl codeine and monoacetyl morphine were also detected. An analysis of the. ingested drug packages showed a mixture of heroin, acetyl codeine and papaverine with 82% dry purity.
The overall findings were entirely consistent with over dosage of controlled drugs. An absence of drug packages beyond the gastric contents indicated that the contraband found at the scene-of-death could have been prior deglutition as a trial bolus.
DISCUSSION
The short case illustrates a health hazard of deglutition controlled drugs in body packers or drug couriers.
There is great potential for sudden deaths from misuser of controlled drugs. This may be evident from drugs paraphernalia retained at the scene-of death. There may external stigmata of drug abuse although drug addicts of today are more discrete about tell-tale signs of a drug habit [4] . Drugs couriers are less likely to arouse interest at immigration checkpoints if external signs of drug abuse are not visible, and favoured by drug barons recruiting them as international human vehicles.
Drug dealers on the street are known to secrete illicit drug supply in the oral cavity and anal cleft. The practice is relatively safe unless there is hurried deglutition of drugs to avoid detection when searched by police[1] .
The packaging of controlled drugs for trafficking may be rudimentary and offer poor protection from gastric acidity. The sophisticated multi-layered types evolved through past experiences of drug couriers also may perish and release drugs[1-5]
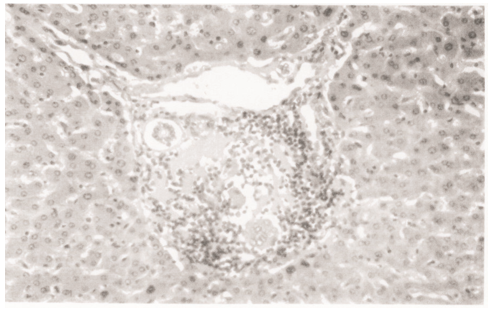
The clinical aspect of the body packer syndrome is reviewed elsewhere [6] . A pathological internal examination constantly shows residual damaged contraband packages and gross pulmonary oedema with deep congestion of the lungs. There may be evidence of infections such as endocarditis, hepatitis and AIDS associated with long term drug abuse. Microscopy may show foreign body giant cells seen in the photomicrograph (figure 3), in reaction to drug adulterants.
Toxicology analyses glucoronide and morphine as metabolite of heroin. A rapid test for morphine indicates a colour change to blue with ferric chloride and quantitatively yellow-orange-red with nitric acid[2] . A drop of sulphuric acid and formalin in equal parts will instantly turn dry residue purple and rapidly turn blue for morphine[2] .
The cause of death was attributed to opiate poisoning from deglutition of self-secreted controlled drug, and the manner of death recorded as misadventure.
REFERENCES
- Patel F. A high fatal post-mortem blood concentration of cocaine in a drug courier. Forensic Science International 1996;79:167-174
- Simpson K. and Knight B. Analgesics, hypnotics, tranquillisers and narcotic poisons. In: Simpson K. and Knight B. (editors) Forensic Medicine -9th edition. Chapter 8. 1985. London. Edward Arnold
- Green M.A. Opioids. In: Polson C.J. Green M.A. and Lee M.R. (editors) Clinical Toxicology -3th edition. Chapter 8. 1983. London. Pitman
- Patel F. Death on a needle. Journal of Clinical Forensic Medicine 2001;8:166-168
- Lancashire M.J. Legg P.K. Lowe M. Davidson S.M. and Ellis B.W. Surgical aspects of international drug smuggling. British Medical Journal 1988;296:1035-1037
- Booker R.J. Smith J.E. and Rodger M.P. Packers, pushers and stuffers -managing patient with concealed drugs in UK emergency departments: a clinical and medicolegal review. Emergency Medicine Journal 2009;26:316-320
STATUTE
Zambia Narcotic Drugs and Psychotropic.
Substances Act 2021.
Medical Journal of Zambia, Vol 50, 1
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.