Determinants of stillbirth in the Five General Hospitals of Lusaka, Zambia: A Case-Control study
Musonda Makasa
Women and Newborn Hospital, University Teaching Hospitals, Lusaka, Zambia.
Zambia Association of Gynaecologists and Obstetricians, Lusaka, Zambia.
Wilbroad Mutale
Departmnt of Health Policy and Management, School of Public Health, University of Zambia, Lusaka, Zambia.
Mwansa Ketty Lubeya
Women and Newborn Hospital, University Teaching Hospitals, Lusaka, Zambia.
Zambia Association of Gynaecologists and Obstetricians, Lusaka, Zambia.
Department of Obstetrics and Gynaecology, School of Medicine, University of Zambia, Lusaka, Zambia.
Young Emerging Scientists Zambia, Lusaka, Zambia.
Tepwanji Mpetemoya
Young Emerging Scientists Zambia, Lusaka, Zambia.
Lusaka Apex Medical University.
Mukambo Chinayi
Young Emerging Scientists Zambia, Lusaka, Zambia.
Benedictus Mangala
Zambia Association of Gynaecologists and Obstetricians, Lusaka, Zambia.
Musole Chipoya Makasa
Zambia National Public Health Institute, Lusaka, Zambia.
Patrick Kaonga
Department of Epidemiology and Biostatistics, School of Public Health, University of Zambia, Lusaka, Zambia.
Department of International Health, Bloomberg School of Public Health, Johns Hopkins University, Baltimore, Maryland, USA.
DOI: https://doi.org/10.55320/mjz.50.1.395
Keywords: Stillbirth, determinants, case-control, Zambia
ABSTRACT
Objective: We aimed to assess determinants of stillbirths among women who delivered from the five general hospitals of Lusaka city, Zambia.
Methods: We conducted an unmatched case-control study. Cases were consecutively enrolled, and controls were randomly selected within 24 hours of occurrence of a case. A structured questionnaire was used to collect data, and multiple regression was used to assess determinants of stillbirths. A p-value of <0.05 was considered sufficient evidence of an association between stillbirth and independent variables.
Results: A total of 58 cases and 232 controls were included in the analysis. Compared with women who delivered babies with birth weight <2500 grams, the risk of stillbirth for women who had babies with birth weight ≥2500 was higher (AOR= 4.49; 95% CI: 2.84 – 8.99); antepartum haemorrhage (AOR = 3.18; 95% CI: 1.21 – 8.09); previous experience of stillbirth (AOR=3.99; 95% CI: 1.73 – 6.73) compared with their counterparts without. Additionally, women with parity > 2 (AOR = 3.02; 95% CI: 1.07 – 7.54) had higher odds of stillbirth compared to those with parity ≤ 2.
Conclusion: Conclusion: Birth weight ≥2.5 kg, antepartum haemorrhage, previous stillbirth were determinants of stillbirth. Program implementers should consider strategies that can mitigate these determinants to reduce stillbirth.
INTRODUCTION
Stillbirth is the occurrence of foetal demise with a birth weight of ≥1000g or ≥28 completed weeks of gestation (World Health [1] ). Globally, an estimated 2.6 million stillbirths are reported every year since 2000. Recent data suggests that there has been a 25.5% decline from 24.7 to 18.4 per 1000 live births worldwide. Despite this reduction, sub-Saharan Africa (SSA) still recorded the slowest decline, with an estimated stillbirth rate of 28.7 per 1000 live births. Approximately 98% of stillbirths were notably in low- and middle-income countries (LMIC), where south Asia and SSA accounted for 77% of the reported cases [2] .
Stillbirth is associated with several social and economic consequences. Pregnancy comes with the expectation of a baby, not only by the immediate family, but also by society. When a pregnancy suddenly results in a tragic and painful outcome, the negative impact is at many levels. Not only on the family but also on obstetrics care services [3] . There are challenges in family relationships, especially in African settings where stillbirth is stigmatized and affects the psychological well-being of the affected families. Stillbirth has negative social constructs that are deeply rooted in many African societies. As a result, they end up being missed in national vital statistics, especially when it occurs outside a health facility resulting in an underestimation of the magnitude of the problem. Stillbirth is estimated to be more than double the financial cost of a live birth [4] .
The determinants of stillbirths are multifactorial, and a significant proportion have unknown aetiology. This can be attributed to limited comprehensive population based surveys regarding the definite cause of stillbirth [5 - 6] . Literature suggests various interlinked determinants of stillbirth are common across most LMICs[7] and may reflect the quality of obstetrics care available during pregnancy and childbirth. Stillbirths occur due to the complex interaction of socio-demographic, behavioural and obstetrics factors [8 - 9] . In high-income countries (HIC), literature shows that some of determinants of stillbirths include placental conditions, foetal/placental pathologies, and antepartum haemorrhage (APH) and a higher proportion are unexplained [10] . Whereas determinants in LMIC include maternal age (less than 20 and above 35 years of age), high birth weight, low education level, increased parity, and poor antenatal care, history preterm birth, APH, and history of stillbirth [11 - 12] . Stillbirth varies across countries and its magnitude fluctuates from time to time. Also, the determinants of stillbirth maybe context-specific, especially in developing countries.
In Zambia, evidence from anecdotal data suggests that stillbirth is a public health challenge with high incidence and prevalence rate. For example, a study conducted in selected health facilities of Lusaka urban more than a decade ago showed that the prevalence of stillbirth was 21 per 1000 live births [13] . It showed that determinants of stillbirth were prior history of stillbirth, APH, extremes of birthweight (<2500g or >4000g), increased maternal age, caesarean and breech deliveries. More recent data estimated 30.5 stillbirths per 1000 live births in certain parts of the country [14] . However, the last Zambia Demographic Health Survey (ZDHS) only reported the perinatal mortality rate for the previous 5-year period under review of 33 per 1000 live births but not specifically stillbirth rate [15] . In response to the challenges in the provision of quality health services and care, the Zambian government established five general hospitals in the year 2018 in Lusaka urban which are equipped with basic obstetric delivery services to improve maternal and perinatal outcomes [16] . One of the priorities set in the Zambia National Health Strategic Plan for 2017 – 2021 is to reduce stillbirth to less than 12 deaths per 1000 live births by 2030 in keeping with WHO target. It is important that the Zambian program implementers prioritized health services that are deemed effective to improve maternal and perinatal outcomes. To reduce stillbirth, assessment of its determinants is key to generate program data that can be utilized for decision-making to fill the gaps in the provision of maternal and perinatal health services and care. Therefore, we aimed to assess the determinants of stillbirths in the five selected general hospitals in Lusaka, Zambia.
METHODS
Study Design and Study Sites
This was a facility based unmatched case-control study conducted between April to June 2022 among women of reproductive age group (15 – 49 years) who gave birth in five general hospitals namely; Kanyama, Chipata, Chawama, Matero and Chilenje in Lusaka urban of Lusaka province. Lusaka city is the capital city of Zambia and is locate in the south central of the country and has eight constituencies with a population of about 1,264 440 million people (312, 255 women of reproductive age group). At the time of data collection, the total number of annual deliveries in the five general hospitals was 120, 000.
Study Population
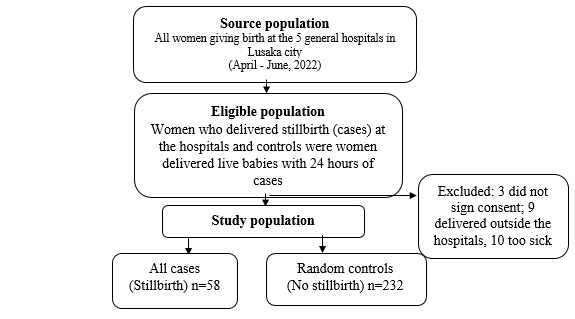
For this study, the stillbirth cases were consecutively enrolled from the five aforementioned general hospitals. The controls were selected from the same hospitals where the cases came from in the ratio one to four (1 case: 4 controls). Cases were from women of child-bearing age (15-49 years), fresh or macerated stillbirth, singleton births, birth weight of 1000 grams and above, or gestation age of 28 completed weeks. Controls were women with the reproductive age group who delivered with 24 hours of stillbirth at the same facility. Four controls were randomly selected from the sampling frame per case. We excluded those who did not sign written informed consent, delivered outside the facility and were too sick to respond to the questionnaire (Figure 1).
Sample Size
For the sample size calculation, A G*Power software for power analysis was used. based on the following assumptions: four controls for per case, power of the study 80% (type II error 20%), 95% confidence interval with 5% type I error, proportional of risk factors in the control participants of 0.33% and cases with potential risk factors to stillbirth of two and half times as likely to be exposed to stillbirth compared to controls (odds ratio = 2.5). Therefore, the calculated sample size was 58 cases and 232 controls.
Sampling Technique
Sample from each hospital was based on probability proportion to size after considering the annual stillbirth reports for each facility in the most recent calendar year (January to December 2021). Matero General Hospital 10 cases and 40 controls, Kanyama General Hospital 13 cases and 52 controls, Chilenje General Hospital two cases and eight controls, Chawama General Hospital 21 cases and 84 controls and Chipata General Hospital 13 cases and 52 controls. Cases were consecutively enrolled but controls were randomly sampled within 24 hours of a stillbirth from a sampling frame that was made before women were discharged in each hospital.
Study Variables
The outcome variable was stillbirth coded (1=stillbirth, 0=livebirth), socio-demographic characteristics were age (≤19, 20 – 34, ≥35 years), education level (no education/primary, secondary, tertiary), marital status (married, single), employment status (employed , not employed), Christian denomination (Catholic, Pentecostal, Protestant, other); behavioural characteristics were alcohol (yes, no) smoker (yes, no), Obstetrics characteristic such as time taken to reach the facility, mode of transport (walking, public transport, owner transport) sex of the baby (male, female), mode of delivery (vaginal, caesarean section), parity (≤2, >2) antepartum haemorrhage (yes, no) birth weight (≤2500, >2500) history of pregnancy loss (yes, no), preeclampsia (yes, no), hypertension (yes, no) HIV status (positive, negative), history of preterm (yes, no), antenatal booking (≤12 weeks, >12 weeks) and history of stillbirth (yes, no).
Data Collection Tool
We developed a questionnaire based on previous studies. One of the principal investigators created an electronic questionnaire with the XLS Form tool and uploaded on ONA server. Data was collected using Open Data Kit (ODK) application which allows collection of data using Android-based tablets in real-time; and ODK Aggregate facilitated data storage. The investigators were constantly conducting data monitoring and management in real-time. At the end of data collection, it was downloaded in excel format and cleaned for analysis.
Data Analysis
Data was collected through mobile applications (i.e., Open Data Kit) using tablets and served on ONA server. Data was later downloaded into excel spreadsheet then exported into Stata 16 software (Stata Corp; College Station, Texas, USA) for analysis. Summary proportions and frequencies for cases and controls were obtained from descriptive statistical analyses. Univariate analysis was conducted to obtain the crude association between stillbirth and independent variables. A p-value of ≤0.2 was used as a cut-off for independent variables to be selected for the multivariable logistic regression model. Evidence of association was determined using p < 0.05 for multivariable logistic analyses, in order to assess the independent determinants of stillbirth among the study participants. We utilized a sequential elimination of candidate determinants by checking on the strength and significance of the variable with stillbirth. Also, discrimination and calibration of the model were checked. Variables such as age and birth weight although they were collected as continuous variables were introduced in the model as categorical variables since this is more intuitive from a clinical point of view. To assess the ability of the model to allocate the appropriate risk, we calibrated the model using Hosmer and Lemeshow goodness of fit test [17] . The interpretation of Hosmer and Lemeshow goodness of fit test was considered an accurate prediction when it yielded a non-significant p- value (p>0.05). For model stability, measured by discrimination and differentiated participants with stillbirth from those without, was assessed by using area under the receiving characteristics curve. We considered an area under the curve of more than 0.7 as acceptable [18] . We utilized Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines in reporting this study [19] .
Ethical Oversight
Ethical approval for this study was obtained from University of Zambia Biomedical Research Ethics Committee (reference number: 1463-2021) and further permission was obtained from the Zambia National Research Health Authority (reference number: 000050/30/03/2022). Confidentiality and privacy were maintained for the women. Women were informed that they were free to withdraw from the study at any time without affecting their healthcare.
RESULTS
In this study, there was a total of 290 participants, 58 cases and 232 controls with ratio of one to four respectively. More than three-quarters of the cases (77.6%) and about slightly below three quarters of the controls (74%) belonged to age group 20 – 34 years. Slightly above half in both cases (52.6%) and controls (51.1%) had secondary education as their highest education level. Those who were not employed were 73.7% and 70.7% in the cases and controls respectively. Majority (64.7%) in the cases and 80.6% in the controls were married. More than four-fifth in cases (80.7%) and controls (85.5%) were not taking alcohol. Slightly below half (48.2%) of the cases and 52.0% of the controls were walking to the facility to access antenatal care. Majority in both cases (82.7%) and controls (92.5%) had vaginal delivery. More than three-quarters of the cases (79.2%) and control (52.4%) had less than or equal to two children. More than one-tenth (14.1%) of the cases and less than one-fifth of the controls experience vaginal bleeding. More than two-thirds of the cases (72.7%) and less than one-third of the controls (28.3%) delivered babies less than or equal to 2500 grams. In both cases and controls, less than one-fifth 17.5% and 10.7% were HIV positive respectively. Almost a quarter (24.1%) in the cases and 12.3% in the controls had history of pregnancy loss (Table 1).


Determinants of Stillbirth
The association between each independent variable and stillbirth was assessed using binary logistic regression model. The regression showed that marital status, parity, antenatal booking, birth weight, history of pregnancy loss, history of stillbirth and antepartum haemorrhage had enough evidence of association with stillbirth. In multivariable regression model, parity, birth weight, history of pregnancy loss and history of stillbirth had enough evidence of association with stillbirth. Women who had more than two children were 3 times more likely to have stillbirth than those who had less than two children (AOR = 3.02; 95% CI: 1.07 – 7.54). Women who delivered babies with birth weight equal to or more than 2500 grams were 4.45 times more likely to have stillbirth than their counterparts who had babies less than 2500 grams. (AOR = 95% CI: 2.84 – 8.99) Those who reported a history of stillbirth were 4 times more likely to have stillbirth compared to women who had no history of stillbirth (AOR = 3.99; 95% CI: 1.73 – 9.73). Women who reported experiencing antepartum haemorrhage in the current pregnancy were 3 times more likely to have stillbirth compared to those without antepartum haemorrhage. (AOR = 3.02; 95% CI: 1.18 - 6.46) as shown in Table 2


DISCUSSION
This unmatched case-control study focused on the determinants of stillbirths among women who delivered in five general hospitals in Lusaka district, Zambia. The results showed that parity of greater than two, babies with birth weight of above 2500 grams, history of stillbirths and history of antepartum haemorrhage were significant determinants of stillbirth.
In this study the odds of experiencing stillbirth were found to be four and half times higher among women who gave birth to babies with birth weight equal or more than 2500 grams compared to women who gave birth to babies to babies less than 2500 grams. This finding is in keeping with previous studies [20 - 21] . Stillbirth among normal birth weight babies is associated with inadequate prenatal care which may result into missed detection of foetal infection during pregnancy especially in resource-poor settings [7] . The increased risk in the latter may be explained by difficulty in delivery of a large or abnormal presentation of the infant, leading to prolonged labour, foetal distress and death [22] .
This study found that presence of antepartum haemorrhage was a determinant factor for stillbirth. This is in agreement with a study from Ethiopia which strengthens the presence of antepartum haemorrhage could be due to placenta praevia and placental abruption which are risk factors for stillbirth [23] . The association of antepartum haemorrhage and stillbirth could reflect poor quality care during childbirth or inadequate maternity services [24 - 25] . In addition, bleeding in pregnancy may result in preterm labour and delivery, foetal death due to inadequate blood supply. Therefore, an active heighten and persistent monitoring strategy should be in place to identify women who are likely to experience APH especially that it may occur without warning signs.
Our study showed that history of stillbirth was a risk factor for stillbirth. Previous studies have reported that history of stillbirth is known to increase the recurrence of stillbirth [20 - 21] due to potential placental vascular disorders [26] and women with such experience should undergo vigorous prenatal care in succeeding pregnancies [21] .
Evidence suggests that pregnant women, who start antenatal care early, within the first trimester, have reduced odds of experiencing stillbirth than those who start after the first trimester [27 - 28] . This was in line with our finding though did not reach statistical significance; probably our study was not powered for this variable. A plausible explanation could be that late antenatal initiation does not offer sufficient time to screen and detect risks and appropriate interventions by health care professionals to prevent stillbirth[29 - 30] .
There are several limitations to this study. First, there was no clinical examination of the cases reported. Therefore, the potential risk factors for antepartum stillbirth, such as placental insufficiency could not have been identified and recorded that way. For instance, women with hypertensive disorders during pregnancy are more likely to have placental compromise, and thus a higher risk for foetal death. Secondly, this is a case-control study, which can only show the association between the various risk factors but cannot show a causal relationship. Thirdly, there is a possibility that maternal medical conditions were not thoroughly examined during clinical assessment prior to admission and thus risk factors like hypertensive disorders in pregnancy, diabetes may not have been properly documented. Fourth, this was a hospital-based study, thus, the background characteristics of the women with stillbirths might not be the same at the population level therefore, our study cannot be generalized.
In conclusion, the study suggests that the determinants of stillbirth are birth weight greater than 2500 grams, parity greater than two, antepartum haemorrhage and history of stillbirth. Therefore, it is recommended that active surveillance during antenatal care for women likely to develop antepartum haemorrhage and those with previous record of stillbirth should be enforced to reduce stillbirth. In addition, women should be encouraged to have fewer children.
ACKNOWLEDGMENTS
We appreciate the great contribution of women who participated in this study especially the cases despite the emotional experience of losing their babies. We acknowledge the immense time and contribution by Dr Mpundu Makasa, Co-PI, PRICE project, University of Zambia, School of Public Health for her critical thinking and suggestions during the initial conceptualizing stage of the study. We are also grateful to Dr Alice Hazemba, Lecturer at the University of Zambia, School of Public Health for her insight and comments during the thought process of the study. In addition, our special thanks go to the data collectors from YES Zambia and staff of the five general hospitals where the study was conducted for their active participation during data collection.
CONFLICT OF INTEREST
All authors declare no conflict of interest
AUTHORS' CONTRIBUTIONS
MM: conceptualization of the study, study design, data collection and manuscript writing. WM: supervision, study design, data collection and manuscript writing. TM: study design, data collection and manuscript writing. MC: study design, data collection and manuscript writing. MCM: conceptualization, study design, data collection and manuscript writing. MKL: conceptualization of the study, study design, data collection, monitoring of the data collection process, and manuscript writing. PK: conceptualization of the study, study design, data collection, monitoring of the data collection process, data analysis, supervision and manuscript writing. All authors read and approved the final version of the manuscript.
REFERENCES
- Organization WH. Perinatal and neonatal mortality. Journal. 2006;281(6254):1567-.
- Blencowe H, Cousens S, Jassir FB, Say L, Chou D, Mathers C, et al. National, regional, and worldwide estimates of stillbirth rates in 2015, with trends from 2000: a systematic analysis. The Lancet Global Health. 2016;4(2):e98-e108.
- Gopichandran V, Subramaniam S, Kalsingh MJ. Psycho-social impact of stillbirths on women and their families in Tamil Nadu, India - a qualitative study. BMC Pregnancy and Childbirth. 2018;18(1):1-13.
- Burden C, Bradley S, Storey C, Ellis A, Heazell AEP, Downe S, et al. From grief, guilt pain and stigma to hope and pride - a systematic review and meta-analysis of mixed-method research of the psychosocial impact of stillbirth. BMC Pregnancy and Childbirth. 2016;16(1):1-12.
- McClure EM, Garces A, Saleem S, Moore JL, Bose CL, Esamai F, et al. Global Network for Women ’ s and Children ’ s Health Research : probable causes of stillbirth in low- and middle-income countries using a prospectively defined classification system. 2018:131-8.
- Seaton SE, Field DJ, Draper ES, Manktelow BN, Smith GCS, Springett A, Smith LK. Socioeconomic inequalities in the rate of stillbirths by cause: a population-based study. BMJ Open. 2012;2(3):e001100-e.
- Goldenberg RL, Saleem S, Pasha O, Harrison MS, McClure EM. Reducing stillbirths in low‐income countries. Acta obstetricia et gynecologica Scandinavica. 2016;95(2):135-43.
- Akombi BJ, Renzaho AM. Perinatal mortality in sub-saharan africa: A meta-analysis of demographic and health surveys. Annals of Global Health. 2019;85(1):1-8.
- Kelly K, Meaney S, Leitao S, O’Donoghue K. A review of stillbirth definitions: A rationale for change. European Journal of Obstetrics & Gynecology and Reproductive Biology. 2021;256:235-45.
- Reinebrant HE, Leisher SH, Coory M, Henry S, Wojcieszek AM, Gardener G, et al. Making stillbirths visible: a systematic review of globally reported causes of stillbirth. BJOG: An International Journal of Obstetrics and Gynaecology. 2018;125(2):212-24.
- Aminu M, Unkels R, Mdegela M, Utz B, Adaji S, van den Broek N. Causes of and factors associated with stillbirth in low- and middle-income countries: a systematic literature review. BJOG : an international journal of obstetrics and gynaecology. 2014;121(4):141-53.
- Saleem S, Tikmani SS, McClure EM, Moore JL, Azam SI, Dhaded SM, et al. Trends and determinants of stillbirth in developing countries : results from the Global Network ’ s Population-Based Birth Registry. 2018;15(Suppl 1).
- Stringer EM, Chibwesha C, Stoner M, Vwalika B, Joseph J, Chi BH, et al. A population‐based cohort study of stillbirth among twins in Lusaka, Zambia. International Journal of Gynecology & Obstetrics. 2015;130(1).
- Serbanescu F, Goodwin MM, Binzen S, Morof D, Asiimwe AR, Kelly L, et al. Addressing the first delay in saving mothers, giving life districts in Uganda and Zambia: Approaches and results for increasing demand for facility delivery services. Global Health Science and Practice. 2019;7:S48-S67.
- Central Statistics Office MoH. Zambia Demographic and Health Survey. 2018. Report No.: 9788578110796.
- Japanembassy. Statement of Mr. Hidenobu Sobashima, Ambassador of Japan to the Republic of Zambia at the Groundbreaking Ceremony at Chipata First Level Hospital, of the Project for Upgrading Lusaka Health Centres to District Hospitals Phase 2. Lusaka; 2018.
- Hosmer DW. Statistics eBook - Hosmer, Lemeshow - Applied Logistic Regression.pdf. 2000.
- Kleinbaum DG, Klein M. Survival analysis: a self-learning text: Springer; 2012.
- Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, Initiative S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Annals of internal medicine. 2007;147(8):573-7.
- Dube K, Lavender T, Blaikie K, Sutton CJ, Heazell AEP, Smyth R. Identification of factors associated with stillbirth in Zimbabwe–a cross sectional study. BMC pregnancy and childbirth. 2021;21(1):1-14.
- Nijkamp JW, Ravelli ACJ, Groen H, Erwich JJHM, Mol BWJ. Stillbirth and neonatal mortality in a subsequent pregnancy following stillbirth: a population-based cohort study. BMC Pregnancy and Childbirth. 2022;22(1):1-9.
- Chuwa FS, Mwanamsangu AH, Brown BG, Msuya SE, Senkoro EE, Mnali OP, et al. Maternal and fetal risk factors for stillbirth in Northern Tanzania: A registry-based retrospective cohort study. PloS one. 2017;12(8):e0182250-e.
- Macheku GS, Philemon RN, Oneko O, Mlay PS, Masenga G, Obure J, Mahande MJ. Frequency, risk factors and feto-maternal outcomes of abruptio placentae in Northern Tanzania: a registry-based retrospective cohort study. BMC pregnancy and childbirth. 2015;15(1):1-10.
- Kc A, Nelin V, Wrammert J, Ewald U, Vitrakoti R, Baral GN, Målqvist M. Risk factors for antepartum stillbirth: a case-control study in Nepal. BMC pregnancy and childbirth. 2015;15(1):1-10.
- Hirst JE, Villar J, Victora CG, Papageorghiou AT, Finkton D, Barros FC, et al. The antepartum stillbirth syndrome: risk factors and pregnancy conditions identified from the INTERGROWTH-21st Project. BJOG: An International Journal of Obstetrics & Gynaecology. 2018;125(9):1145-53.
- Monari F, Pedrielli G, Vergani P, Pozzi E, Mecacci F, Serena C, et al. Adverse Perinatal Outcome in Subsequent Pregnancy after Stillbirth by Placental Vascular Disorders. PLOS ONE. 2016;11(5):e0155761-e.
- Ota E, K SL, Middleton P, Flenady V, Wmv W, Mo R, et al. Antenatal interventions for preventing stillbirth, fetal loss and perinatal death: an overview of Cochrane systematic reviews (Review). 2020.
- Pattinson RC, New E, Plan A, Africa S, Trial AC, Antenatal WHO, Trial C. Does antenatal care timing influence stillbirth risk in the third trimester ? A secondary analysis of perinatal death audit data in South Africa. 2017:140-7.
- Tesfaye M, Dessie Y, Demena M. Late antenatal care initiation and its contributors among pregnant women at selected public health institutions in Southwest Ethiopia Article Abstract. 2021.
- Wolde HF, Tsegaye AT, Sisay MM. Late initiation of antenatal care and associated factors among pregnant women in Addis Zemen primary hospital, South Gondar, Ethiopia. Reproductive Health. 2019;16(1):73-.
Medical Journal of Zambia, Vol 50, 1
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.