Mad Dogs and Englishmen - A case of fatal hyperthermia in military personnel
K Saasa
General Practitioner
MSS Patel
Consultant Pathologist
DOI: https://doi.org/10.55320/mjz.49.4.394
Keywords: hyperthermia, heat exhaustion, heat stroke, body temperature, tropical sun, hot climate, ultraviolet B rays
ABSTRACT
A case of fatal hyperthermia in a military personnel is reported. It highlights the health hazards of over exposure to hot temperatures. A clinico-pathological aspect of the topic is discussed.
INTRODUCTION
“Mad dog and Englishmen” is the title of a 1930's song with lyrics by an Englishman Noel Coward (1899-1973). The verses advise fellow expatriate sunbathers about hazards of tropical sun e.g. “go out in the midday sun when local natives retire to tear their clothes off and perspire”. Another line, “one must avoid sultry sun's UV light” could be a muted reference to dermatological complications like sunburn and malignant melanoma.
A hypothalamic autoregulation controls the body temperature within a critical limit at 37°C (98.4°F). A failure of this 'thermostat' which results in a raised core temperature above 38°C (101°F), subject to ambient humidity, will manifests as hyperthermia. In febrile conditions the hypothalamic thermostatic setting is raised to bring about 'therapeutic' pyrexia. In contrast, a drop below 32°C (90°F) develops into hypothermia. All may have a fatal outcome, especially if untreated in the early stages.
In comparison to hyperthermia, hyperpyrexia is the predominant clinical presentation in tropical Africa especially due to the prevailing broad spectrum of infectious diseases. Saasa K, personal observation.
An overdose with drugs such as atropine, phenothiazines and amphetamines can also cause hyperthermia.[1-2] An adverse reaction to anaesthetic agents or sedatives administered to patients with a genetic disorder of the skeletal muscle causes malignant hyperthermia.[1-3] Medically induced hyperthermia has been used in specialised centres to treat certain cancers.
Hyperthermia can occur in leisure pursuits such as sunbathing and lying in solar beds, and in some occupations like athletics, firefighting, furnace operation and soldiering.
Sunbathers of today are generally better informed of the solar health hazards. This is evident from the widespread use of sun hats and sunscreen compounds to block the harmful effect of UVB sun rays needed for synthesising 'sunshine vitamin' cholecalciferol D3. There are also Health and Safety laws enacted to provide occupational protection in the workplace.
CASE REPORT
A young fit and active Briton who was serving in the military, based in the Mediterranean, regularly took part in strenuous exercises in hot climate. He had past history of heat stroke under similar circumstances two years earlier and was successfully treated by cooling and rehydration. At that time he was suspected to have suffered rhabdomyolysis. He had been declared fully fit to participate again in a strenuous army exercise.
On this fatal occasion, he was in mufti when participating with his unit in a voluntary fitness test cum cross-country run. He suffered an episode of heat stroke which registered a rectal temperature of 42°C (107°F). He was treated by active cooling and cooled IV fluid rehydration but became moribund at the army hospital. He remained unconscious and required ventilation. He developed renal failure and coagulation tests suggested a possibility of disseminated intravascular coagulopathy (DIC). His condition continued to deteriorate over the next five days until his death.
A thanatopsy revealed gross cerebral oedema without focal abnormality; pulmonary oedema with deep congestion and haemorrhagic pneumonia; confluent pericardial petechiae and myocardial haemorrhages, and hepatic steatosis with a nutmeg pattern. The other organs were unremarkable, including skeletal muscles which showed no sign of rhabdomyolysis.
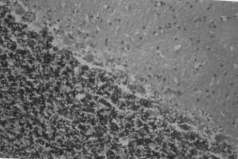
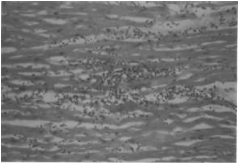
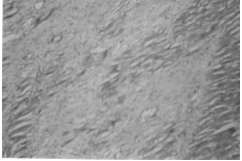
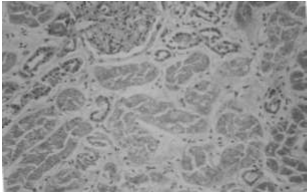
Microscopy showed occasional chromatolysis of cerebellar Purkinje cells (Figure 1); focal myocarditis with a chronic inflammatory cell infiltrate and ischaemic myocardial scarring (Figures 2 & 3); severe haemorrhagic pneumonitis, and colonies of Gram positive bacteria (Figure 4); renal acute tubular necrosis with granular casts, but no sign of DIC (Figure 5) as depicted in the microphotographs, and hepatic centrilobular necrosis with venous congestion.
The overall findings, although not pathognomonic were consistent with the medical diagnosis of a heat stroke.

DISCUSSION
The short case illustrates solar health hazards which can be climatic or environmental.
Overheating of the body or hyperthermia occurs when the body fails to cool down sufficiently by dissipating excessive heat generated by overexertion or prolonged exposure under hot temperatures. The syndrome ranges from the less serious heat rash, heat cramps and heat syncope to more serious heat exhaustion which can lead to life threatening heatstroke or sunstroke at 40-41°C (104-106°F) with sudden loss of consciousness.
A medical diagnosis can be made from the history and the prevailing core temperature. The lesser manifestations can be treated safely by first-aid intervention but heat or sun strokes must be medically managed at a hospital.
The pathology in heat stroke are cerebral degenerative changes where the neurones become hydropic and pyknotic and develop gliosis. There is loss of cerebellar Purkinge cells.[1] There may be intraventricular septal haemorrhages.[1-3] There may also be cardiopulmonary haemorrhages.[1-3]
Depending on post event therapeutic intervention and survival period, there may be myocardial necrosis, lobar pneumonia, renal nephrosis and hepatic centrilobular and adrenal cortical necrosis. DIC which was suspected in the case illustrated can be fatal.[1-3] Some of these features were evident as shown in figures 1 - 5.
Death was attributed to acute haemorrhagic pneumonia consistent with hyperthermia.
REFERENCES
- Gee D. Deaths from physical and chemical injury, starvation and neglect. In: Mant A.K, (ed) Taylor's principles and practice of medical jurisprudence. 13th edn. London: Churchill Livingstone, 1984, ch 12
- Simpson K, et al. The ultimate effect of injury. In: Simpson K, Knight B, (eds) Forensic Medicine. 9th edn. London: Edward Arnold, 1985, ch 9
- Gee D.J. Thermal injuries. In: Polson C.J, Gee D.J, Knight B, (eds) The essentials of forensic medicine. 4th edn. Oxford Pergamon Press, 1985, ch 7
Medical Journal of Zambia, Vol 49, 4
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.