Changing Roles of a Radiographer in Fluoroscopy: Literature Review to Guide the Development and Practice of Fluoroscopic Studies in Zambia
Osward Bwanga
Midlands University Hospital Tullamore, Radiology Department,
Ernest Chanda
Cancer Diseases Hospital and Lusaka Apex Medical University, Lusaka, Zambia
Edward Mwansa
Evelyn Hone College of Applied Arts and Commerce, Lusaka, Zambia
Billy Nkoloma
Zambia Airforce Hospital, Lusaka, Zambia
DOI: https://doi.org/10.55320/mjz.49.4.393
ABSTRACT
Fluoroscopic imaging services in Zambia have been available since 1972 when the first equipment was installed at the University Teaching Hospital (UTH). However, there is limited fluoroscopy equipment use due to a critical shortage of radiologists who are traditionally trained to carry out this role. Radiologists work alongside radiographers who provide technical support and patient care. To address the shortage of radiologists, radiographers in the United Kingdom (UK) have explicitly expanded their scope of practice and started performing and reporting on fluoroscopic examinations such as barium swallow, barium meal, small bowel follow-through, barium enema, and video fluoroscopy after undergoing appropriate training. Literature from the UK shows that gastrointestinal (GI) radiographers' performance is of a high-quality standard. The initiative has been very effective and made a significant contribution to the delivery of fluoroscopic services in that country. Therefore, the aim of this article was to review the literature on role extension for GIradiographers to guide the development and practice of fluoroscopic studies in Zambia. It is anticipated that this article will bring awareness to stakeholders such as the Ministry of Health (MOH), Schools of Radiography, the Radiological Society of Zambia (RSZ), and the Zambia Medical Association (ZMA) on this important subject.
INTRODUCTION
Fluoroscopy is the next old estimating modality after conventional radiography. Since the discovery of Xrays in 1895, this modality has made significant contributions to the diagnosis and treatment of diseases. Ehrlich and Coakes[1] define fluoroscopy as an imaging modality that allows a moving X-ray image to be viewed in real-time. In Zambia, the first fluoroscopic equipment was installed at the University Teaching Hospital (UTH) of Lusaka in 1972. Traditionally, fluoroscopy is undertaken by aradiologist who operates the equipment in accordance with legislation such as the Ionising Radiation Protection Act of 2011 of the Republic of Zambia. [2] The traditional duties of a radiographer include equipment and patient preparations and monitoring radiation exposure.[1-3] Figure 1 shows a fluoroscopic equipment.

Fluoroscopyis an added application to conventional radiography. Most fluoroscopic equipment can perform both fluoroscopy and conventional radiography. This is an advantage to limited resource settings like Zambia because the equipment can be placed around the country to be used for both functions. Unfortunately, there are few fluoroscopic equipment in Zambia. At the time of writing this article, seven (7) functional fluoroscopic equipment were in the country serving a population of approximately 19.6 million. Fluoroscopy also offers the ability for the focused and functional examination of a particular region of interest in real-time.[4-5] For example, the oesophagus can be evaluated in real-time during a barium swallow by the radiologist. This is not possible with conventional radiography. However, fluoroscopy exposes patients to potentially higher doses of ionising radiation than conventional radiography.[1-6]
The benefit of performing fluoroscopy outweighs the increased dose.
Globally, the use of fluoroscopy started declining in the 1970s following the advancement in medical imaging technology and the discovery of crosssectional modalities such as ultrasonography (US), CT, and MRI.[1-4] The other reason for the decrease in the use of fluoroscopy is the critical shortage of radiologists to use the equipment and report on images.[4,7,8] To overcome, this challenge, radiographers in some countries such as the United Kingdom (UK) have formally extended their role to performing and reporting on fluoroscopy examinations such as barium and videofluoroscopic studies.[7] There is something to learn from this important initiative, especially in developing countries such as Zambia where the problem of shortage of radiologists is even worse than in the UK.
AREAS OF ROLE EXTENSION FOR RADIOGRAPHERS IN FLUOROSCOPIC STUDIES
There are three areas of role extension in fluoroscopic studies for radiographers reported in the literature: performing barium studies, performing videofluoroscopic swallow studies, and interpreting and reporting on barium studies. All these areas relate to gastrointestinal (GI) imaging. GI imaging involves examining any part of the alimentary tract and often requires the use of a contrast media to enable the structures to be visualized during fluoroscopy.[1-8] Traditionally barium sulphate suspension has been used as contrast media in GI studies. Since the 1990s, performing and reporting on barium studies have become areas of advanced practice for radiographers in the UK who carry out procedures previously undertaken by radiologists.[7-8] With a critical shortage of radiologists, radiographers working in Zambia can extend their role in this area.Like their counterparts in the UK, Zambian radiographers can perform barium studies with appropriate training, and expansion of their scope of practice by the Health Professions Council of Zambia (HPCZ), the regulatory body.
Performing barium studies
One of the common examinations performed using fluoroscopic equipment is barium studies. Globally, undergraduate radiography programmes include fluoroscopic procedures in the curriculum. For the last 20 years, radiographers in the UK have been performing barium studies with little or no radiologist involvement. [8] Due to a shortage of radiologists to perform barium studies, radiographers in Zambia have already taken up this role with radiologists reporting on fluoroscopic studies. However, medical facilities such as Kalindawalo General Hospital (KGH) andChinsali General Hospital(CGH) offering fluoroscopic imaging services (Table 1) have no on-site radiologists. This leaves the interpretation of barium studies to the referring clinicians, who are not experts in image interpretation of fluoroscopic studies. This practice can lead to errors and delays in the commencement of patient treatment. Four main barium studies are performed in Zambia: barium swallow, barium meal, small bowel follow-through (SBFT),and barium enema.
Barium swallow- a fluoroscopic examination of the oesophagus performed after introducing a positive contrast media. The purpose of this examination is to demonstrate radiographically the anatomy and function of the oesophagus.[5] The common indications for barium swallow include dysphagia, foreign body (FB), gastroesophageal reflux disease (GERD), hiatus hernia, achalasia, and carcinoma of the oesophagus. The contraindications mostly arise from the use of barium sulphate suspension. In case of suspected perforation or aspiration, non-ionic water-soluble contrast such as gastrografin should be used which can be absorbed by the body. [5-9] A radiograph of the barium swallow is shown in Figure 2.

The imaging technique for performing a barium swallow involves the radiologist or GI radiographer positioning the patient on an erect fluoroscopic table. The patient is then asked to drink barium sulphate suspension and screening is undertaken to view the movement of barium through the mouth to the stomach. A series of images is undertaken and reported after the medical imaging examination.
Barium meal- is a fluoroscopic examination of the stomach and duodenum performed following the introduction of a positive contrast media. The objectives of the barium meal examination are to study radiographically the anatomy and function of the distal oesophagus, stomach, and duodenum and to detect abnormal anatomic and functional conditions. [1-5] The main indication for barium meal includes ulcers, gastritis, diverticula, carcinomas, hiatal hernia, hypertrophic pyloric stenosis (HPS), and bezoar. The contraindications for barium meal examination relate to the use of barium sulphate. If the patient has a history of bowel perforation, laceration, or rupture of the viscus, an oral, water-soluble, iodinated contrast medium such as gastrografin should be used in place of barium sulphate. [5-10] Aradiograph of the barium meal is shown in Figure 3.

In most radiology departments, a barium swallow is always done in conjunction with a barium meal.[10] Following the barium swallow, the patient is positioned supine and additional contrast is given and images are taken in different positions.
Small bowel follow-through (SBFT) - is a fluoroscopic examination of the small bowel(intestine) performed following the introduction of a positive contrast media. The common indications for SBFT are malabsorption, neoplasm, bowel obstruction, and diverticula. Patients with suspected bowel perforation or possible large bowel obstruction should not receive barium sulphate suspension. [5-10] A radiograph of the SBFT is shown in Figure 4.
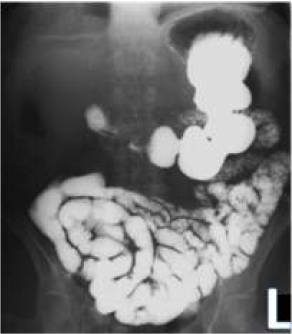
The patient is asked to drink barium sulphate suspension and images of the abdomen (fluoroscopy and/or conventional radiography) are taken every 30 minutes until the small bowel fills up. The examination frequently takes 2 hours, but in some instances, it can take a day.[5] When contrast reaches the terminal ileum, the examination is complete. Sometimes, delayed imaging is required to follow the contrast through the entire large bowel which normally can take 24 hours to reach the rectum. [5-9]
Barium enema- is a fluoroscopic technique of imaging the large bowel (colon). The examination is performed either by single-contrast or doublecontrast techniques. In a single contrast technique, imaging is done using positive contrast, whilst, in double contrast, both positive and negative contrast media are used to increase the sensitivity of the examination. [5] Barium sulphate or gastrografin are positive contrast, while air or carbon dioxide (CO2) is negative. The common clinical indications for performing barium enemas include polyps, neoplasm, colitis, diverticular disease, intussusception, and volvulus. The two strict contraindications for the barium enema are the same as small bowel follow-through: suspected bowel perforation and large obstruction.[9] For these conditions, a patient should not be given barium sulphate. A radiograph of the barium enema is shown in Figure 5.

The procedure for conducting a barium enema involves a patient lying on the left side on the fluoroscopic table and a lubricated catheter is inserted into the rectum by the radiologist or GI radiographer. It is common practice to give a hypotonic agent such as buscopan just before inserting the catheter to reduce bowel spasms.[5] A bag of barium sulphate suspension is suspended on the drip stand and allowed to slowly run into the bowel under control. Fluoroscopic images are taken in various positions to follow the contrast media. This is a single-contrast imaging technique. Sometimes, the examination can be performed using a double contrast technique where air or carbon dioxide is added. This technique moves the main bolus of barium forward, leaving behind only the barium adhering to the mucosal walls which and effective in the demonstration of polyps and diverticula.[5-9] A chaperone of the same sex as the patient should be present during the examination for the comfort of the patient. [11] The chaperone can also act as a witness in case the patient complains of unprofessional behavior from the radiologist or radiographer.
Radiographers should undertake training before taking up advanced roles. The first postgraduate training course for GI radiographers in the UK was developed in 1993 which is referred to as the “Leeds Course”. [7] It is estimated that more than 1200 radiographers working in the UK have undertaken this postgraduate course by 2007.[7] Some universities such as the University of Salford have integrated barium studies intotheir masters in advanced medical imaging for radiographers. [12] There are also other universities offering barium studies courses across the UK. In Zambia, fluoroscopic studies have been included in the undergraduate radiography programmes at all four (4) schools of radiography: Evelyn Hone College (EHC), the Lusaka Apex Medical University (LAMU), University of Zambia (UNZA) and Levy Mwanawasa Medical University (LMMU). The objective is to equip radiographers with knowledge and skills for performing and evaluating fluoroscopic studies such as barium swallow, barium meal, SBFT,and barium enema. Since radiographers have already taken up the role of performing barium studies in Zambia, the masters in diagnostic radiography curriculum being used at UNZAcan be scaled up to expose radiographers to advanced knowledge and skills in this area or establish a specialised training course.
Performing videofluoroscopic swallow study(VFSS)
Another role radiographers have taken up in the UK is performing videofluoroscopic swallowing studies(VFSS) also known as modified barium swallow studies.[7,8,13] The American Speech- language Hearing Association (ASLHA) [14] defines a videofluoroscopic swallowing study as a radiographic procedure that provides a direct, dynamic view of oral, pharyngeal, and upper oesophageal function. The aim of this fluoroscopic examination is to assess patients who have swallowing dysfunction due to mechanical or neuromuscular problems, with the result that they are at increased risk of aspiration and inevitable associated chest problems. [9] Identifying these patients early in their treatment plan can reduce hospital admission for chest infections such as aspiration pneumonia. [8] The patient is given various consistencies of food mixed with barium sulphate suspension which allows the bolus to be visualised in real-time using fluoroscopy during swallowing and recorded in a video format. This is the reason why the examination is referred to as a videofluoroscopic swallow study. Theexamination assists healthcare professionals to determine the diagnosis and appropriate clinicalmanagement strategies.
Traditionally, VFSS examinations are undertaken by a Speech-language Therapist (SLT) working alongside a radiologist to conduct and interpret the examination, with a radiographer providing technological support.[13] However, the role of a radiologist has been taken up by radiographers in the UK and the Republic of Ireland.[13-15] Radiographers and SLTs perform VFSS examinations dependently without a radiologist.
The University of Salford in the UK offers training in videofluoroscopy under the masters in advanced medical imaging course for radiographers.12 This module focuses on clinical practice and reporting. In the Republic of Ireland, the Irish Institute of Radiography and Radiation Therapy (IIRRT)[15] also provides a two-day videofluoroscopy training course for radiographers annually. The course content includes introductions and indications for VFSS, anatomy of the pharynx and oesophagus, physiology of normal swallowing, stroke, and aging (effects on swallowing), penetration and aspiration, standard VFSS procedure, contrast media and food preparations, fluoroscopic equipment,and radiation protection, image evaluation and reporting, protocols for radiographer-SLTs lead VFSS clinics, and practical. Regarding image interpretation, the University College London (UCL)in the UK offers an introductory course to the interpretation of videofluoroscopic images in the diagnosis and treatment of patients with acquired dysphagia. [16] This postgraduate course equips radiographers and SLTs with image interpretation and reporting skills in VFSS.
In Zambia, VFSS imaging services are not available despite having fluoroscopy equipment and SLTs in the country. This may be attributed due to a shortage of radiologists to perform and report on the examinations. At the time of writing, there were 12 radiologists and three (3) SLTs in Zambia. [17-18] Direct radiologist services are only in urban areas of the Lusaka and Copperbelt provinces, leaving the remaining eight (8) provinces with none. A lack of radiologists in Zambia has been identified by the Ministry of Health and research studies as a hindrance to the delivery of quality medical imaging services.[19-21] Performing VFSS is one area where Zambian radiographers can extend their role and start this service in conjunction with SLTs and expand fluoroscopic services.
Interpreting and reporting on barium studies
Image interpretation and reporting on barium studies is another role where radiographers have extended their role in the UK. This was the third area of role extension in image reporting after ultrasonography and plain film radiography (appendicular, axial, chest and abdomen).[22] Radiographers undertake this role after undergoing appropriate postgraduate education and training in this speciality.
Research and clinical audits have been conducted to determine the quality of reporting radiographerson barium studies in the UK. One such researchwas carried out by Murphy et al., [23] to compare the diagnostic reports from GI radiographers and radiologists on barium enema studies on 788 patients. Taking the radiologist reports as the gold standard, radiographers' diagnostic reports were concordant in 753 (95.5%) studies. Another research performed by Law et al., [24] with 5516 double contrast barium enema studies over a 4-year period found no discrepancy in the diagnostic reports made by reporting radiographers and radiologists. The sensitivity score for reporting radiographers was found to be 94.5%. A retrospective audit was also conducted by Judson and Nightingale [25] to determine whether trained radiographers can perform and interpret barium swallows and meals to an acceptable standard. The overall accuracy of reporting radiographers based on 935 studies conducted over a 4- year period was 98.9%, sensitivity 98%, and specificity 98.9%. These research studies show that appropriately trained radiographers can perform and interpret barium studies examinations to a high standard.
To equip radiographers with image interpretation knowledge and skills, training programmes have been developed as part of advanced practice in medical imaging. The University of Salford offers clinical practice and reporting barium studies courses as part of the masters in advanced medical imaging course for radiographers. [12] The other Higher Education institution (HEIs) providing barium enema reporting is Robert Gordon University (RGU) of the UK. [26] The training enables the radiographers to demonstrate competence in image interpretation and reporting on barium enema studies.
With the critical shortage of radiologists in Zambia, this is one area where the Radiological Society of Zambia (RSZ) can advocate for role extension. At the time of writing, there were 1600 radiographers and radiography technologists in Zambia. Before allowing radiographers to start interpreting barium studies, appropriate education and training should be in place and the scope of practice extended by the Health Profession Council of Zambia (HPCZ). It is also important to involve key stakeholders during planning such as radiologists, medical doctors, clinical officers, medical licentiates, and schools of radiography.
BENEFITS FOR RADIOGRAPHERS PERFORMING AND REPORTING ON BARIUM STUDIES
Performing and reporting on barium studies is part of advanced practice for radiographers. Therefore, the benefits of advanced practice or role extension for radiographers also apply in the context of this article. The benefits identified from the literature could be grouped under four stakeholders: the patients, GI radiographers, radiologists, and radiology departments. For the patients, there is a reduction in waiting time and improved patient care. [8-27] With the establishment of GI radiographers in Zambia, more patients will have access to barium studies both in urban and rural areas because radiographers are found across the country where medical imaging facilities are available. The current direct access to barium studies is limited to the community in the following 7 medical facilities offering fluoroscopic services (Table 1):

The main benefits to radiographersare improvement in their status and increased job satisfaction. [7-28] A research study conducted by Ng'andwe and Bwanga[29] found that radiographers in Zambia emigrate to other countries such as Botswana and the UK due to job dissatisfaction. Another reason identified was a lack of postgraduate specialised courses and limited career pathways. Therefore, the introduction of GI radiographers to perform and interpret barium studies can result in job satisfaction and the retention of radiographers. To radiologists, this initiative will reduce their workload and enhance the collaboration between the two imaging professionals. [28] Therefore, radiologists should not see the role extension of radiographers as an incursion into their domain, but as partners in the delivery of quality imaging services. [27] It should be mentioned that radiologists have a key role to play in supporting radiographers undertaking advanced practice by providing training and acting as mentors.
[30] Lastly, the benefits to the radiology department and the Ministry of Health (MOH), would help bridge the gap created by the shortage of radiologists in Zambia. [27] There is a delay in reporting due to a lot of pending radiographic images for report owing to the limited number of radiologists in Zambia. This leads to deferment in applying appropriate medical intervention to the affected patients. Therefore, the establishment of GI radiographers will result in increased and improved healthcare service delivery. It will fulfil the MOH's policy of bringing health services as close to families as possible.In addition, the advanced practice in radiographyreduces costs and generates economic cost savings as the salaries of GI radiographers are lower than radiologists. [8-28]
The lack of on-site radiologists in some hospitals offering fluoroscopic services results in extra costs associated with the transmission of images to hospitals with radiologist services. The introduction of VFSS will add to the current local imaging services in the country which will benefit patients with suspected swallowing dysfunction due to mechanical or neuromuscular problems. It will also bring awareness about the role of STLs in VFSS imaging services.
CONCLUSION
The shortage of radiologists in Zambia affects efficient medical imaging service delivery. This can be cushioned by extending the roles of radiographers to include performing and reporting on barium studies as seen in the UK. The lessons learned from the UK regarding the establishment of GI radiographers if adopted in the Zambian healthcare system have the potential to improve the delivery of fluoroscopic services. The suggested strategy for implementation relies on the involvement of stakeholders such as the MOH,RSZ, HPCZ, and schools of Radiography. The establishment of GI radiographers will bring fluoroscopic imaging services as close to the families as possible, boosting work satisfaction amongst radiographers as advanced roles come with increased enumeration and incentives.
ACKNOWLEDGEMENT
The authors would like to acknowledge the radiology department management at Chinsali General Hospital and MainaSoko Medical Centre for providing radiographic images used in this article. Special recognition and gratitude are extended to the Radiation Protection Authority (RPA) for supplying the data on the medical facilities with functional fluoroscopic X-raymachines in Zambia. Thanks go to the Radiological Society of Zambia (RSZ) for supporting the idea of role extension for radiographers. The authors would also like to thank Joseph Mulenga for proofreading the manuscript before submitting it for publication.
CONFLICT OF INTEREST
None to declare.
REFERENCES
- Ehrlich RA, Coakes DM. Patient care in radiography: with an introduction to medical imaging. 10th ed. London: Elsevier; 2020.
- Republic of Zambia. Ionising radiation protection act of 2011 (Amended). Lusaka:Government printers; 2011.
- Irish Institute of Radiography and Radiation Therapy. Fluoroscopy: guidelines on best practice. 3rd ed. Dublin: IIRRT;2013.
- Shalom NE, Gong GX, Auster M. Fluoroscopy: An essential diagnostic modality in the age of high-resolution cross-sectional imaging. World J Radiol . 2 0 2 0 ; 1 2 ( 1 0 ) : 2 1 3 - 2 3 0 .doi:10.4329/wjr.v12.i10.213
- Bontrager KL, Lampignano JP. Radiographic positioning and related anatomy, 6th ed. Mosby: MI. St. Louis; 2014.
- International Commission on Radiation Protection. Radiological protection in fluoroscopically guided procedures performed outside the imaging departmentICRP Publication 117. London: SAGE Publication Ltd; 2010.
- Nightingale J, Hogg P. The role of the GI radiographer: a United Kingdom perspective.Radiol Technol. 2007;78(4):284-290.
- College of Radiographers. The role of the radiography workforce in gastrointestinal imaging . London : The College of Radiographers; 2021.
- Carver E, Carver B. Medical imaging:techniques, reflection and evaluation. Amsterdam: Elsevier; 2012.
- Watson N, Jones H. Chapman and Nakielny's guide to radiological procedures. 7th ed.London: Elsevier; 2017.
- Bwanga O, Kayembe R M. Experiences of patients with computed tomography (CT) examinations: asystematic review of qualitative evidence. International Journal of Medical Reviews, 2022; 9(2): 244-253. doi:10.30491/ijmr.2022.279253.1195
- University of Salford. MSc advanced practice in m e d i c a l i m a g i n g ; 2 0 2 2 . F r o m http://www.salford.ac.uk/courses/postgraduate/advanced-medical-imaging (accessed on 10 November 2022)
- Newman RD, Nightingale J. Improving patient access to videofluoroscopy services: role of the practitioner-led clinic. Radiography.2011;17(4): 280–283. doi: 10.1016/j.radi.011.04.005.
- American Speech- language Hearing Association.Videofluoroscopic swallowing study (VFSS); 2022. Fromhttps:www.asha.org/public/speech / s w a l l o w i n g /videofluoroscopic-swallowing-study/(accessedon 10 November 2022).
- Irish Institute of Radiography and Radiation Therapy. Introduction to videofluoroscopy course; 2020. From ww.iirrt.ie/introuductionvideofluoroscopy-course-23rd-24th-march-2020/ (accessed on 12 November 2022).
- University College London. Reading adult videofluoroscopies: introductory course; 2022. From https://www.ucl.ac.uk/pals/reading-adult-videofluoroscopies-introductory-course(accessed on 15 November 2022).
- Bright S, Selemani, C. The development of speech-language pathology in Zambia: A reflection on the current landscape and two contrasting training models. Perspectives of the ASHASpecial Interest Groups,2017; 2, 63-72.
- Bwanga O, Mulenga M, Jere E, Sichone J. Is it possible to miss a metallic airway foreign body on a chest radiograph? Imaging case report from Zambia. Medical Journal of Zambia, 2022;49(1), 96-101.
- Ministry of Health. National health strategic plan 2017-2021. Lusaka: The Ministry of Health; 2017.
- Bwanga O, Mulenga J, Chanda E. Need for image reporting by radiographers in Zambia.Medical Journal of Zambia. 2019; 46(3): 215-220.
- Zulu EO, Phiri L. Enterprise medical imaging in the global South: challenges and opportunities;2022. From tttps://ieeexplore.ieee.org/document/ 9845508 (accessed on 16 November 2022).
- College of Radiographers. Preliminary clinical evaluation and clinical reporting by radiographers: policy and practice guidance. London: College of Radiographers; 2013.
- Murphy M, Loughran CF, Birchenough H, Savage J, Sutcliffe C. A comparison of radiographer and radiologist reports on radiographer conducted barium enemas.Radiography. 2002; 8 (4): 215–221,
- Law RL, Titcomb DR, Carter H, Longstaff AJ, Slack N, Dixon AR. Evaluation of a radiographer-provided barium enema service.Colorectal Dis. 2008;10(4):394-396.doi:10.1111/j.1463-1318.2007.01370.x
- Judson EE, Nightingale JM. An evaluation of radiographer performed and interpreted barium swallows and meals. Clin Radiol.2009;64(8):807-814. doi:10.1016/j.crad.2009.04.008
- Robert Gordon University. Barium enema reporting; 2022. From www4.rgu.ac.uk/prospectus/modules/disp_moduleView.cfm?Descriptor=HSM028 (accessed on 15 November 2022).
- Bwanga O, Chanda E, Kafwimbi S, Sichone J. Opinions of Zambian radiographers on extending their role in interpretation and reporting on general radiographic images: a cross-sectional survey. Medical Journal of Zambia, 2021; 48(3), 212 - 220.
- Thom SE. Does advanced practice in adiography benefit the healthcare system? A literature review. Radiography. 2018;24(1):84-89. doi:10.1016/j.radi.2017.08.002
- Ng'andwe EM, Bwanga O. Factors affecting the ability of radiographers to deliver imaging services in rural parts of Zambia. Radiography. 2 0 2 2 ; 2 8 ( 3 ) : 7 5 8 - 7 6 5 . d o i : 1 0 . 1 0 1 6 /j.radi.2022.03.005
- Bwanga O, Kayembe RM, Sichone JM. Intravenous cannulation and administration of contrast media by radiographers: a literature review to guide the training and practice in Zambia. Afr Health Sci. 2022;22(2):629-637.doi:10.4314/ahs.v22i2.72
Medical Journal of Zambia, Vol 49, 4
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.