Prevalence, Awareness And Adverse Outcomes Of Breast Ironing Among Cameroonian Women In Buea Health District
Mela Fotabong
Pan-African University of Life and Earth Science Including Agriculture (PAULESI), University of Ibadan, Nigeria
Gbolahan Obajimi
Pan-African University of Life and Earth Science Including Agriculture (PAULESI), University of Ibadan, Nigeria
Temitayo Lawal
Department of Epidemiology and Medical Statistics, Faculty of Public Health, College of Medicine, University of Ibadan, Ibadan, Nigeria
Imran Morhason-Bello
Pan-African University of Life and Earth Science Including Agriculture (PAULESI), University of Ibadan, Nigeria
DOI: https://doi.org/10.55320/mjz.49.4.391
Keywords: Breast ironing, Prevalence, Awareness, Consequences, Adverse outcomes, Cameroon.
ABSTRACT
Background: Breast ironing, also known as breast flattening, is a practice that involves the use of an object to massage, press, or pound the breast. This practice is usually performed on girls, between the ages of 9 and 15 years The known effects of breast ironing are self-reported symptoms or signs of breast ironing by the victims. This study aims to investigate the prevalence, awareness, and adverse outcomes of Cameroonian women towards breast ironing.
Methods: A mixed method design involving qualitative and cross-sectional study among women aged 18years and above. The primary outcome variable was previous experience of breast ironing. Log-binomial model was used to determine effects of breast-ironing on selected reproductive health outcomes.
Results: Of 160 women interviewed, 22 (14%) had experienced breast ironing. The mean age was 26±4.62 years. All participants were aware of breast ironing. There were significant associations between being a victim of breast ironing and parity, breast symmetry, nipple anatomy, breast pain, milk quantity during lactation, breast sagging. The risk of reporting breast ironing was higher among women who experienced breast sagging earlier than expected, women who reported breast pain and women whose breasts had marked asymmetry.
Conclusion: Breast ironing is prevalent in the Buea health district of Cameroon, and victims are more likely to experience adverse breast outcomes. Health education and introduction of legislation against breast ironing will go a long way to eliminate this harmful traditional practice. More studies will help to further understand drivers of breast ironing in other regions of Cameroon.
INTRODUCTION
Breast ironing, also known as breast flattening, is a practice that involves using an object to massage, press or pound the breast flat.[1] Breast ironing is one of the traditional practices that is prevalent in some parts of Africa and is considered by the United Nations as a form of gender-based violence.[2] It is usually performed on girls, between the ages of 9 and 15 years at the start of breast development or pubarche to reduce size or delay its development,[2-3] with the belief that a flat child-like chest will discourage unwanted male attention, rape and premarital pregnancy.[4-5]
Breast flattening, female genital mutilation, forced marriages, dowry violence, and (but not limited to) honour killings, are considered by the United Nations (UN) as discrimination and violence against women.[6] This practice is not only seen in rural communities or developing countries but has been reported in immigrant communities in the United Kingdom.[4] As a result, the National Female Genital Mutilation Centre (NFGMC) in 2016 in England called on local authorities to review their internal violence against women and girls strategy, and include breast ironing as a form of violence against women.[7]
Breast ironing is practised in some West African countries including Guinea Bissau, Togo, Chad, Benin, Ivory Coast and Cameroon.[4] Reports of the practice have also been received from Kenya, Zimbabwe, and South Africa.[4] Breast ironing is more prevalent in Cameroon than in the countries mentioned above as it is practised in all the ten regions of the country.[3,4] In 2005, a nationwide quantitative study conducted by the Cameroonian NGO, Réseau National des Associations des Tantines (the National Network of Aunties, hereafter “RENATA”) interviewed 5,661 girls and women between the ages of 10 and 82 on “breast ironing” and reported that about 24% of girls and women had experienced a form of breast ironing. In the Littoral Region of Cameroon, the prevalence of breast ironing was about 54%.[1]
Furthermore, previous studies have reported that the prevalence rate, method of ironing, rationale for ironing, and reported outcomes vary significantly by region and individual, and have no proven correlation with socio-economic level, urban or rural living, religious affiliation, or ethnicity.[1,3,8] The level of education and exposure of women does not prevent them from carrying out this practice.[7] According to a report, a Senior Cameroonian Official who had never heard of breast ironing, discovered that his wife had clandestinely performed the procedure on their daughters without his knowledge or consent,[6] further underscoring the ignorance of some men about the practice in their homes.[8]
Several objects have been reported as tools for performing breast ironing. Example of such objects include grinding stone, black fruit, plantain peel, mortar pestle, coconut shell or hammer (all carefully heated over burning coals).[4] With these hot objects, perpetrators press and iron their victim’s developing breasts to destroy any indication of emerging womanhood. The massage could last from one week to several months depending on how resistant the breasts are and also depending on how resistant the victim or her body is to the practice. Sometimes, the heated objects are used twice a day for weeks or months to crush the budding breast.[9] The victims report that the procedure is excruciatingly painful.[9,10,11] The objects are heated to the extent that the perpetrators sometimes use a cloth or bag to protect themselves from burns. It was reported that a woman sustained second degree burns in the process of ironing her daughter’s breast and only then did she understand the agony her daughter had been going through.[12]
There are short- and long-term effects of breast ironing which could manifest as physical and or psychological symptoms and signs.[12] Some effects of breast ironing have been reported by victims but have not been extensively studied. These effects include an immediate delay or halting of breast growth, swelling, burning, irritation, pimples on the breasts, abscesses, fever, extreme pain, a long-term overgrowth of one or both breasts or failure of one or both breasts to grow, difficulty with breast-feeding, scarring, and breast cancer.[1,8,12] This study is therefore one of the few to apply a multivariable regression to adverse effects of breast ironing in Cameroon, and aims to investigate the prevalence, awareness and adverse effects associated with breast ironing among Cameroonian women. This information would be useful in understanding the adverse effects associated with breast ironing among women.
METHODOLOGY
This was a mixed method study that involved a cross-sectional design for the quantitative arm and focus group discussions (FGDs) and in-depth interviews (IDI) for the qualitative arm. The study was conducted in five hospitals in Buea Health District, Southwest Region of Cameroon. The qualitative study was conducted among victims of breast ironing, which was then followed by the quantitative study. Information collected was used to design the data collection tool that was used for the quantitative study. Each FGD was made up of three women and it explored the meaning and interpretation of the culture of breast ironing in Cameroun. It also sought to understand the drivers and barriers in perpetuating this practice and their awareness on regulation. Two FGDs were conducted in two separate facilities to prevent information diffusion between participants – one of them among nulliparous victims of breast ironing and the other among victims of breast ironing who have delivered at least once. After the FGDs, two women from each group were selected for the IDIs which sought to know the role of their parent, their personal view on this practice including whether they will permit breast ironing for their children, personal benefits and medical challenges they experienced. The theoretical framework was based on socio-ecological models where breast ironing practices were explored from the perspectives of individual, family, community, and policy levels. Notes were taken during the discussions and interviews.
A cross-sectional study was conducted among women seeking reproductive care services including antenatal care (ANC), family planning (FP) and infertility management. Women were recruited by convenience sampling. A structured questionnaire was administered to women who gave consent to be part of the study after explaining the study procedure. Individual participants completed the questionnaire containing demographic data, awareness and previous experience with breast ironing. The last part of the questionnaire contained information about examination and was completed by the primary investigator or research assistant trained to conduct breast examination. The size of the breast was estimated through the cup size of the participant’s bra and subjectively, participants were asked if they judged the size their breasts to be normal, smaller, or larger than normal.
Sample size was calculated using the formula for estimating proportions[13-14] and a mimium of 150 participants were required. 160 respondents were selected in order to increase the precision of the study. A cluster sampling technique was use to select 5 facilities where data was collected. The first two facilities were used as sites for the qualitative study whilst the other three were for the cross-sectional study. Data collection was via a questionnaire which was checked for completeness and entered using the statistical package for social scientist (IBM SPSS) version 20. Statistical analysis was carried in STATA version 15. Descriptive analysis was displayed in the form of tables, charts, percentages, and frequencies. Inferential statistics was done using the Chi Square and Log-binomial regression model. Risk ratio was presented at 95% confidence interval and a p value of less than 0.05 was considered significant, prior to which a likelihood ratio test was performed. The audio recordings of the qualitative data were transcribed verbatim. The principal investigator read the transcripts, manually coded the information into predetermined themes and data were analysed using thematic content analysis.
RESULTS
Socio-Demographic Data
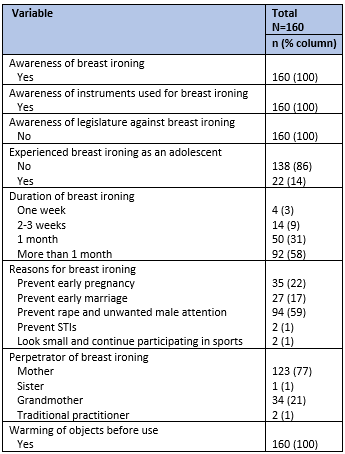
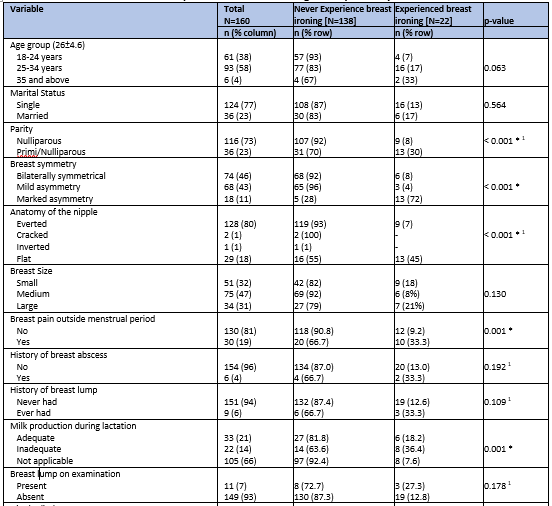
The mean age and standard deviation of the 160 participants recruited for this study was 26±4.62 years, range 18 – 38 years. 77% of participants were married while 23% were single. Nulliparous women constituted 73% of the study population while women who have had one and two deliveries were made up 22% and 5% respectively. The mean bra size of participants was 34, and the results of breast examination showed that larger percentage of the participants had an everted anatomy of the nipple (80%) and about half (46%) had bilaterally symmetrical breast.
Awareness of the Practice of Breast Ironing
All participants (100%) were aware about the practice of breast ironing. They had either been a victim of the practice, known someone who was a victim or had heard of the practice. Furthermore, all the participants correctly defined breast ironing as “the practice whereby an object was used to massage, pound or press the developing breast of young girls flat”. All participants stated that they were not aware of any laws against breast ironing practice.
Prevalence and Practice of Breast Ironing Practice
Twenty-two out of 160 participants had experienced breast ironing as adolescent, giving a prevalence of 14%. Most of the participants (89%) stated that the practice lasted at least 1 month. However, victims of the practice all agreed that the practice lasted for at least one month while 77% of the victims reported that the practice lasted more than 1 month.
Perpetrators and Objects used for Breast Ironing
The most prevalent perpetrators of the practice were mothers and grandmothers who performed the practice in 77% and 21% respectively. Sisters of the victim and traditional practitioners were each reported by 1% of participants as perpetrators of breast ironing.
The most common objects used for breast ironing reported by participants were grinding stones and pestle which represented 34% and 23% of all objects used respectively. All participants agreed that the objects were heated before use.
Reasons for Breast Ironing Practice
The most common reason for breast ironing reported by the participants was to prevent rape and unwanted male attention (59%). Two additional reasons by some victims of breast ironing are as follows: “our parents ironed our breasts so we should continue to look young and keep on participating in sporting activities in schools meant for minors”. Two out of 160 participants believed that the practice was carried out to prevent sexually transmitted infections.
Perception and Intention towards Breast Ironing Practice
Perception on the practice of breast ironing- All participants stated that breast ironing was a bad cultural practice.
Intention to carry out breast ironing or their children - All participants reported that they will not perform breast ironing on their children, and they wanted the cultural practice to be abolished.
Success of the Practice: Almost three quarter (74.4%) of the participants reported that the practice did not stop breast development. On the other hand, almost half of the victims of breast ironing (45.5%) reported that the procedure was successful.
Association between Experience of Breast Ironing and explanatory variables
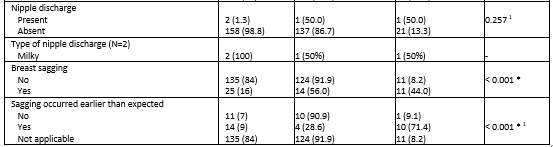
The percentage of women who had experienced breast ironing was very high among women with who experienced sagging earlier than expected (71%). Also, women who had inadequate milk production during lactation also had a high percentage (36%) of women who had experienced breast sagging. The results showed an association between experience of breast ironing and explanatory variables such as breast pain during menstrual period, milk production during lactation, breast sagging and time at which sagging.
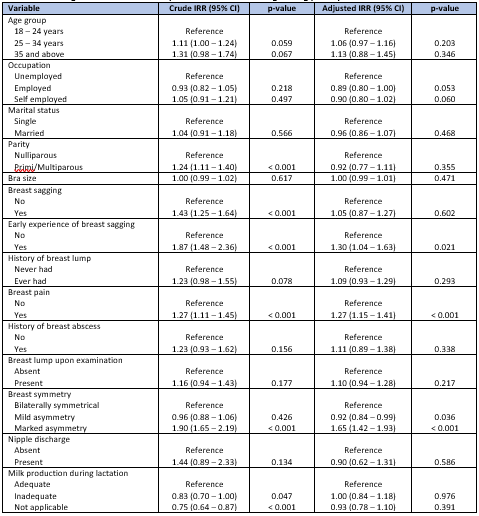
Risk Factors Associated with Breast Ironing Practice
Women who had experienced breast ironing as an adolescent were more likely to have an early experience of breast sagging than those who had never experienced breast ironing (adjusted Risk Ratio (aRR): 1.30; 95% Confidence Interval (CI): 1.04-1.63). Also, women who reported breast pain were more likely to have experienced breast ironing than women who did not report breast pain (aRR: 1.27; 95% CI: 1.15-1.41). Women whose breast exhibited marked asymmetry were more likely to have had previous experience of breast ironing than women with bilaterally symmetrical breast (aRR: 1.65; 95% CI: 1.42-1.31).
DISCUSSION
The prevalence of breast ironing in this study was 14%. This was lower than the National prevalence of 21% obtained by Rebecca Tapscott in 2015.[1] This may be due in part to the high awareness and condemnation of the practice.[8-15] However, the prevalence of breast ironing in this study was higher than that of the Southwestern region (11%) of Cameroon where the study was conducted.[1] All participants were aware of breast ironing, suggesting that the practice was very common in the community. Despite the high level of awareness, majority condemned this cultural practice because of the adverse physical, psychological, and emotional problems that were commonly reported by the victims.
This study further revealed that all participants could correctly define breast ironing and explain how the procedure was performed. This high level of awareness about the practice might not be unconnected to the increased sensitisation to prevent and discourage breast ironing in the community.[6-12] The French photojournalist Gildas Paré in 2015 carried out a campaign against breast ironing by publishing pictures of victims on his website and social media channels condemning and discouraging the procedure.[12]
Although women were aware of breast ironing and how it was performed, they were not aware of any laws prohibiting the practice. Currently in Cameroon, there is no specific law prohibiting breast ironing, however regional treaties prohibiting violence against girls and women have been endorsed.[9] It is therefore paramount to ratify laws against breast ironing, specifically prohibiting the practice and imposing severe sanctions on persons who perform this dastardly act. In this study we found that there was no association between breast size and breast ironing i.e., the breast size of women who experienced breast ironing and those who did not experience it were similar as measured by the cup sizes of their bra. This is probably because the practice does not significantly halt breast development. Even if the practice halts breast development as claimed by half of the victims of the practice, it was unlikely that scarification of the overlying skin from hot iron could damage alveola cells. The relationship between breast ironing and breast size would require further investigations. There was equally no statistically significant relationship between breast ironing and breast abscess or breast lump.
This study revealed that the risk of breast pain outside menstrual cycle was higher among women who had experienced breast ironing as an adolescent (p<0.001). The associated pain may be due to the process of ironing which was very painful and could lead to undue sensitization of pain fibres in the breast. Marked breast asymmetry was more common in victims of breast ironing and thus a higher risk was also observed among women who had experienced breast ironing as an adolescent. This study further revealed an association between breast ironing and breast sagging. Those who experienced breast ironing as an adolescent reported had higher risk of reporting early onset of breast sagging, compared to their counterparts who did not. Breast ironing leads to destruction of the suspensory ligaments of the breasts resulting in early onset of breast sagging.
LIMITATIONS
The study was limited to the Buea health district of Cameroon and is therefore not a representation of the nation. The study is a cross-sectional one and hence cannot make causal inference.
CONCLUSION
Breast ironing a common traditional practice in the Buea health district of Cameroon, has far reaching consequences. This study revealed a prevalence of 14% which was lower than the National prevalence of 21%. Despite being aware of the practice and procedures for breast ironing, respondents were not aware about laws prohibiting the practice. The need for legislation and enforcement in Cameroon to prevent this harmful traditional practice is imperative and cannot be over-emphasized. Reproductive health and sexual education should be promoted by providing appropriate education and communication materials highlighting the dangers and consequences of breast ironing. Punitive measures for perpetrators and sexual offenders should be made public with the intent to stem the tide of this unwholesome practice. Collaboration with all stakeholders in the health sector and the ministry of justice along with non-governmental organizations will serve as an initial step in drive to eliminating breast ironing in Cameroon.
LIST OF TABLES
COMPETING INTEREST
The authors declare no competing interest.
AUTHORS' CONTRIBUTIONS
MF, GO and IM conceptualized the study. MF was involved in data collection process with major contributions from GO and IM. MF, TL and IM were involved in the analysis, and all authors participated in the drafting and approval of the final manuscript. IM and GO are senior authors in this manuscript.
ACKNOWLEDGMENT
The authors wish to acknowledge the Pan African Institute of Life and Earth Sciences (PAULESI) who provided funding for the postgraduate degree program leading to this publication.
REFERENCES
- Tapscott, R., Understanding Breast "Ironing": A Study of the Methods, Motivations, and Outcomes of Breast Flattening Practices in Cameroon. 2012.
- Robinson, F., Breast ironing. BMJ, 2019. 365: p. l1790.
- Mukuma, N.D., I., Breast Ironing in Cameroon: an overview for Fair Fund. 2007: p. 5.
- Amahazion, F., Breast ironing: A brief overview of an underreported harmful practice. J Glob Health, 2021. 11: p. 03055.
- Lazareva, I., Breast Ironing: 'the whole community needs an education', in The Guardian. 2019.
- Pemuta, N.V. The Social Context of Breast Ironing in Cameroon. 2016. Athens: ATINER'S Conference Paper Serioes.
- Tri.x. Breast Ironing in UK. 2019 [cited 2021 October 26]; Available from: https://www.trixonline.co.uk/policy-briefs/2019/july/july-252/.
- Pearsell, R., The Harmful Traditional Practice of Breast Ironing in Cameroon, Africa. Bridges: An Undergraduate Journal of Contemporary Connections, 2017. 2(1).
- Tchoukou, J.A., Introducing the Practice of Breast Ironing as a Human Rights Issue in Cameroon. Journal of Civil & Legal Sciences, 2017. 3(121).
- Bawe, R.N., Breast Ironing: a harmful practice that has been silenced for too long. Gender Empowerment and Development (GeED), 2011: p. 10.
- Brandley, T., Breast ironing: a harmful practice that doesn’t get sufficient attention, in The Conversation. 2019: Academic rigour.
- Pare, G., The Victims of Cameroon's Horrific Breast Ironing Tradition. VICE France, 2015. pg. 1-37. Accessed on 26-10-2021
- Charan, J. and T. Biswas, How to calculate sample size for different study designs in medical research? Indian J Psychol Med, 2013. 35(2): p. 121-6.
- Kasiulevicius, V.S., V.; Filipaviciūte, R., Sample Size Calculation in Epidemiological Studies. Gerontologija, 2006. 7: p. 225-231.
- Glover Williams, A. and F. Finlay, Breast ironing: an under-recognised form of gender-based violence. Arch Dis Child, 2020. 105(1): p. 90-91.
Medical Journal of Zambia, Vol 49, 4
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.