Prevalence of Tuberculosis in HIV- or Tuberculosis-exposed neonates at the University Teaching Hospital in Lusaka over a period of six months
Matimba Dindi
University Teaching Hospital Children’s Hospital, Nationalist Road, Private Bag RW1X, Lusaka, Zambia.
Chishala Chabala
University Teaching Hospital Children’s Hospital, Nationalist Road, Private Bag RW1X, Lusaka, Zambia.
Somwe wa Somwe
University Teaching Hospital Children’s Hospital, Nationalist Road, Private Bag RW1X, Lusaka, Zambia.
DOI: https://doi.org/10.55320/mjz.49.4.390
Keywords:Neonate, Tuberculosis, HIV exposed, Xpert MTB-RIF
ABSTRACT
Background: Tuberculosis (TB) is the leading cause of mortality globally and represents a major health problem. The burden of TB in Zambia is among the highest in the African region with a national prevalence estimated at 455/100 000 for all age groups. A large proportion of people with TB are in the reproductive age group as such may either be pregnant or have young children. As at 2014 the prevalence of TB among women attending antenatal care in Zambia was estimated to be 1.5% in HIV infected women and 1.4% in uninfected women. There is a close association between maternal TB and HIV infection and postpartum infant morbidity and mortality. TB in neonates is very rare but a tenfold increase in the risk of acquiring TB in infants born to HIV infected mothers has been documented.
Methods: A cross sectional study was conducted to establish the prevalence of tuberculosis in neonates exposed to either HIV or TB, or to both TB and HIV. The study included neonates aged 28 days and below that were admitted to the intensive care unit (NICU) and nurseries on general pediatric wards at the University teaching hospital. Mothers to neonates that had a positive rapid HIV test were approached, made aware of the study and invited to participate by giving consent to have their baby included in the study. When consent was granted, basic demographic details and medical information were collected. One gastric lavage sample was collected before the first feed of the day and analysed using Xpert MTB- RIF test.
Results: One hundred forty-nine consecutive neonates that met the inclusion criteria were enrolled in the study. The average age of the neonates was nine days, 49 % had mean birth weight of 2.50kg (0.85 SD), 86 full term delivery and 73 (49%) were male. One hundred, ten (110) were born to multiparous (74%) vs 38 primiparous (26%) mothers. All the neonates enrolled in the study were HIV exposed and only one neonate was exposed to both TB and HIV. Mycobacterium tuberculosis was detected in 2 out 149 samples analysed using the Xpert MTB-RIF test. None were positive for rifampicin resistance.
Conclusion: The prevalence of TB using Xpert MTB-RIF test performed on gastric aspirates of HIV exposed neonates admitted to the University teaching hospital is 1.3 %.
INTRODUCTION
Tuberculosis (TB) is one of the leading infectious causes of mortality globally affecting both adults and children, as such represents a major health problem. In 2016, there were an estimated 10.4 million new TB cases: 6.2 million among men, 3.2 million among women and 1.0 million among children. Mortality from tuberculosis was reported at 1.7 million worldwide[1] .
The burden of TB in Zambia is among the highest in the African region with a national prevalence estimated at 455 per 100,000 population for all age groups[2] . A greater proportion of TB cases (51%) are within the reproductive age group. Therefore, many patients with TB will either be pregnant or have young children. Studies in pregnant women, have shown that TB is an important cause of morbidity in women requiring obstetric inpatient care, accounting for 15-34% of non-obstetric maternal deaths[3-4] . TB prevalence of 1.5% and 1.4% in HIV and non-HIV infected women attending antenatal care in Zambia in 2014 was documented[5] .
Maternal and childhood TB are epidemiologically linked and there is close association between maternal TB and postpartum infant morbidity and mortality in children born to HIV infected women[6-7] . Neonatal TB is closely related to maternal antenatal TB infection. Infants born to HIV infected mothers have a tenfold risk of acquiring TB[8] .
Vertical transmission of TB has been documented but thought to be rare[9] . Very few studies have been conducted to explicitly understand the burden of tuberculosis in neonates. Transmission rates of up to 16% have been observed in the first 3 weeks of life[10-11] .
Tuberculosis in neonates is difficult to diagnose because clinical features are like other neonatal or congenital infections. Diagnosis of TB in the neonate is based mainly on the maternal history, the physical signs and failure to respond to antibiotics and supportive therapy as well. Conventional methods of detecting TB in children i.e microscopy and culture have poor yields of up to 70% even with meticulous attention to detail in preparation and analysis of samples[12] . Newer and rapid methods for diagnosis of TB among children are now available and highly recommended. Among them Xpert MTB RIF test which is now recommended as the initial diagnostic test in children suspected of having TB or Multi-drug resistant TB regardless of HIV status[1] .
This study sought to establish the prevalence of tuberculosis in HIV exposed neonates using Xpert MTB-RIF by analysing gastric aspirates of neonates that had history of maternal TB and HIV exposure or either of the two conditions.
METHODOLOGY
This was a cross sectional study conducted at the University Teaching Hospital, in Lusaka, Zambia from June 2017 to May 2018 on HIV and TB exposed neonates admitted to the Neonatal intensive care unit and nurseries on general pediatric wards for various medical conditions.
Neonates with any of the following were considered for the study; HIV exposed; presence symptoms suggestive of TB in the mother and a diagnosis of Tuberculosis in pregnancy in the mother. Assuming a study population of approximately 3600 neonates admitted to NICU every six months and the sample size was calculated using the prevalence formula. The calculated sample size was 207.
Excluded neonates included those whose mothers were non-reactive for HIV antenatally, presence of congenital malformations requiring nasogastric tube for continuous decompression of the stomach and neonates with pulmonary or gastrointestinal hemorrhage.
Convenience sampling was used to recruit research participants. Every consecutive HIV or TB exposed neonate whose rapid HIV antibody test was positive was considered for the study. If the mother or guardian consented to participating in the study, the baby was recruited and assigned a serial number.
HIV infected mothers whose babies were admitted to NICU or the nursery, were identified through the mandatory counselling and testing that is offered to all inpatients.
Once the informed consent was obtained, required information was collected using the data collection sheet and physical examination conducted on neonates.
A gastric lavage was then done before the first feed of the day 4 to 5 hours after the last evening feed. One gastric wash out was done using 10mls of normal saline after which gastric contents were collected and stored in a sterile container. The gastric aspirate samples were stored temporarily in an airtight box, pending transfer the laboratory.
In the laboratory, samples were collected in falcon centrifuge tubes. Using a sterile pipette, the sample was mixed with the Xpert MTB RIF sample reagent in the ratio of 2 volumes of reagents to one volume of sample. The mixture was vortexed for 1 minute at high speed and left to incubate for 5 minutes after which the mixture was vortexed again for another minute and left to stand for a further 10 minutes. Two millilitres of the liquefied sample was then transferred to an Xpert MTB RIF cartridge sample chamber dispensing slowly to minimize the risk of aerosol production. The cartridge lid was closed tightly and loaded into Xpert MTB RIF machine and left to process for one hour, forty-five minutes. Internal quality control using a known MDR TB sample was performed each time a new lot of shipment of reagents was used.
The results were reported as “MTB not detected” for negative samples and “MTB detected” for positive samples. Tuberculosis determined by a positive Xpert MTB- RIF result. Data and sample collection were done primarily by the investigator. The data was entered in excel spreadsheet and imported into Stata Corp LP Version 13, College station Texas, USA and data analysis was conducted Stata software. Proportions were used to describe age, gender, HIV status, whereas means were employed to describe birth weights, gestation age and maternal age. Baseline characteristics are presented in tables.
Ethical clearance was obtained from ERES converge IRB. Permission to conduct the study was obtained from UTH administrative management.
The purpose and procedures of the study were clearly explained in the language preferred by the parent/guardian and a written informed consent obtained.
RESULTS
One hundred and sixty (162) mothers and neonates were identified for the study. A hundred and fifty-eight mothers gave consent for their babies to be enrolled in the study while 4 declined and were excluded. One hundred forty nine (149) samples were collected. Nine neonates were excluded for various reasons; 1 died before the sample was collected,5 neonates were discharged before sample collection while the other 3 neonates whose mothers had given consent initially declined sample collection on subsequent contact.
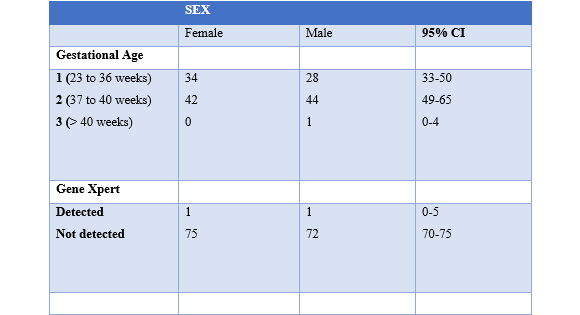
Two neonates had Mycobacterium tuberculosis detected in the gastric aspirate samples. The first one a female, aged 3 days at the time of enrolment in the study while the other was a male infant aged 26 days at the time of presentation. Both were born at term with birth weights of 3.5kg and 2.8kg respectively.
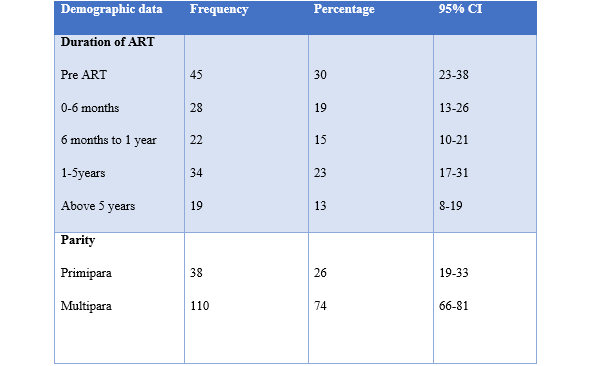
All the 149 women had positive antibody test for HIV. None of these had a history of being treated for TB in pregnancy. Forty-five (30%) of these, were not on antiretroviral therapy for PMTCT. They were the majority in this study. The main reason for this, was delayed booking or commencement of antenatal care. A few women had declined treatment despite being tested earlier in pregnancy on account that the first test done, was non-reactive. Twenty-eight (19%) had been on treatment for six months or less. Thirty-four mothers had been on treatment for a period between one and five years while 19 women were on treatment for more than 5 years. These accounted for 23% and 13% respectively.
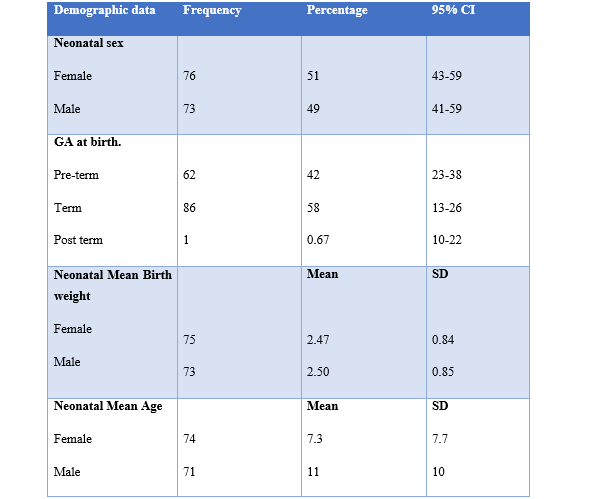
One hundred forty-nine neonates were included in the study. Seventy-six (76) females and 73 males, giving 51% and 49% respectively translating to a ratio of 1:1.
The mean age for female neonates was 7.3 days while for males 11 days. There was no significant difference in the birth weight by gender. The mean birth weight for female babies was 2.47kg while for male babies had an average weight of 2.50kg at birth.
Sixty-two (42%) were preterm deliveries, 86 (58%) were term babies and 1 was a post-dates delivery accounting for 0.67% of the target population for this study.
Majority of the neonates were term babies accounting for about 57% while 43% were born prematurely.
Two out of the one hundred forty-nine samples analysed had MTB detected by gene Xpert accounting for 1.3% of the samples analysed.
DISCUSSION
The study found a low prevalence of TB 1.3% 95% CI (0-5 %) using MTB RIF test performed on gastric aspirates of HIV exposed neonates admitted to UTH. The findings presented above represent a partial analysis of the results of this study. The calculated sample size was 207, however 149 samples had been analyzed over the six-month period due to constraints on funds to purchase gene Xpert cartridges.
All the neonates enrolled in the study were exposed to HIV. One neonate was exposed to both HIV and household tuberculosis contact through a father that had been diagnosed with sputum positive pulmonary tuberculosis soon after the baby was born. The proportion of mothers pre ART was considerably high at 30 % putting them at higher risk of tuberculosis among many other opportunistic infections. A positive HIV status, in the mother increases the risk of TB[13] . Consequently, posing a risk of TB in their babies[11-14] . However, this is not reflected in the results obtained. The probable explanation for this observation is that the HIV infections or seroconversion could have been recent therefore significant immunosuppression had not occurred in these women. A third of this group of mothers gave history of an earlier HIV test being non-reactive, while the majority had not booked for antenatal care yet and had gone into preterm labour and diagnosed to have HIV infection intrapartum. This finding raises concern that the HIV infection rates are still high in our country therefore escalation of prevention strategies is required in order to prevent worsening of the HIV prevalence rates in Zambia.
Seventy percent (70%) of the mothers had been on treatment for varied periods of time, a few months to several years with the longest being 13 years. This may also explain the very low prevalence of TB in the neonates enrolled in this study as transmission and out comes are affected by the duration of therapy before delivery. Four months or more of therapy has been shown to be protective to the unborn baby.
The first baby was referred to NICU for moderate birth asphyxia a few hours after birth and was managed for presumed sepsis with respiratory distress. Physical examination revealed fever, tachycardia and tachypnoea with subcoastal recessions, however the chest had vesicular breath sounds on auscultation. The baby improved and was discharged on day 10 of life after treatment with antibiotics and respiratory support with CPAP. The gastric lavage samples were analysed a day before the baby was discharged, hence at the time results were received the patient was no longer in hospital and was lost to follow up.
The second baby was referred for pneumonia from a first level hospital. He presented with a history of a cough, fever and worsening difficulty breathing. On examination he had fever, severe respiratory distress and some muscle wasting. His weight was 2.5kg and it was 300grams less than his birth weight. He also had coarse crepitations bilaterally and failure to thrive. He was managed for pneumonia with little improvement on first- and second-line antibiotics and had persistent respiratory distress for two weeks during admissions. A chest radiograph revealed multiple heterogeneous opacities in both lungs. He was commenced on ATT after the gastric lavage sample result revealed MTB detected. He was discharged a few days later after resolution of fever and respiratory distress. His weight also improved to 2.8 kg.
The clinical characteristics observed in the two neonates are comparable to those documented in literature. Most researchers have observed that symptoms in neonatal tuberculosis are often non-specific making diagnosis a challenge. Infected neonates can present from birth to several weeks of age and may appear acutely or chronically ill. Neonates most often have lung and liver involvement. Abnormalities on chest radiograph are common but varied.
The most important component of diagnosis is the degree of clinical suspicion. Three other neonates enrolled in this study were commenced on TB treatment based on chest radiograph findings as well as un-resolving pneumonia and fever despite treatment with antibiotics for more than seven days. The gene Xpert analysis did not detect MTB. One of these neonates treated presumptively, had a positive household Tb contact. The father had been commenced on TB treatment a few days before the baby was born. This patient was discharged after 3 weeks in hospital following clinical improvement. One patient did not improve much on ATT and died while in hospital while third patient was discharged on request. The patient improved clinically on ATT and was weaned off supplemental oxygen.
The prevalence of tuberculosis in HIV or TB exposed neonates at the University Teaching Hospital is 1.3% 95 % CI (0-5). This is in keeping with observations made in several centers that TB in neonates is rare[15] . Studies conducted in South Africa between 1996 and 1998 demonstrated prevalence rates as high as fifteen percent[15] . These studies were done at the peak of the HIV pandemic in Africa when access to anti-retroviral therapy (ART) was limited and most patients did not access treatment easily. This has changed over the years with more women gaining access to ART leading to improved immune status and probably reducing occurrence of opportunistic infections such as tuberculosis.
In 2014, a two year retrospective study of maternal deaths at UTH revealed that TB was responsible for 25% of mortality.3 Nineteen years later, Zambia has made several strides in the provision HIV care to women, children and the general population at large, therefore a reduction in morbidity and mortality from tuberculosis and other HIV related illnesses. The WHO 2017 Global report indicates that globally TB mortality rate is falling at about 3% per year while the incidence is falling at 2% per year. The decline among high burden countries, Zambia inclusive, has been estimated at 4%.
Currently, HIV care in the country is on an ambitious target of achieving universal access to ARV drugs, treating and preventing HIV and ultimately ending the HIV epidemic by 2030.This has led to the ‘test and treat’ strategy with the provision of ART regardless of CD4 cell count to all pregnant and breastfeeding women. Implementation of these guidelines is being strengthened at district and health facility level implying that fewer and only complicated cases of HIV or TB may be seen at a tertiary hospital like UTH. Therefore, what is obtaining at UTH may not be representative of situation in the district or country at large.
CONCLUSION
The prevalence of tuberculosis in neonates admitted to the University teaching hospital using the Xpert MTB RIF test is 1.3%.
REFERENCES
- WHO Global TB Report 2017. Global tuberculosis reports 2014 and 2015. Clin Perinatal 2017; 24; 111-120.
- Kapata N. Chanda- Kapata P, Ngosa W, Mine M, Klikenberg L, Nico K, Sunkutu V, Shibemba A, Chabala C. Chongwe G, Tembo M et al (2017). The Prevalence of TB in Zambia; Results for the First National Tb prevalence survey,2013-2014.http;/doi.org/10.1371/journal.pone.0146392
- Ahmed Y, Mwaba P, Chintu C Grange JM, Ustianowski A, Zumla A. (2017). A study of maternal mortality at University Teaching Hospital, Lusaka, Zambia. The emergence of tuberculosis as a major non-obstetric cause of maternal death. Int J Tuberc Lung Dis 2014; 3:675-80
- Khan M, Pillay T, Moodley JM, Connolly CA (2001). Maternal mortality associated with tuberculosis-HIV-1 co infection in Durban, South Africa. AIDS 2001; 15:1857-1863
- Kancheya N. Luhanga D, Harris JB, Morse J Kapata N, Bweupe M, Henostroza G, Reid SE. (2018). Integrating active tuberculosis case finding in antenatal services in Zambia.Int J tuberc Lung Dis 2014 Dec;18 (12): 1466-72.doi:10.5588/ijtld.14.0920
- Batra S, Ayaz A. Murtaza A, Ahmed S, Hasan R and Pfau R (2012) Childhood Tuberculosis in Household Contacts of Newly Diagnosed TB patients. PloS One7, e40880.
- Gupta A, Bhosale R, Kinikar A et al. (2011). Maternal tuberculosis; a risk factor for mother to child transmission of HIV.J Infect Dis 2011;203;358-363.
- Mukadi Y, Braun M, Nsanga B et al. (2009). A Retrospective cohort Study of the Risk of Tuberculosis among Women of Childbearing Age with HIV infection In Congo DRC.https://doi.org/10.1164/ajrccm/143.3.501
- Hassan G, Quresh W, Kadri S M. Congenital Tuberculosis (2006). J K Science Vol 8 No 4 193-4.
- Adhikari, M., (2009), Tuberculosis and tuberculosis/HIV co- infection in pregnancy, Seminars in Fetal & Neonatal Medicine doi: 10.1016/j.siny.2009.
- Bekker A, Preez D, Schaaf H, Cotton M.F, Hesseling A.C. (2012). High tuberculosis exposure among neonates in a high tuberculosis and HIV burden setting. International journal of tuberculosis and lung disease. Vol 16, No 8 2012 pp 1040-1046/7.
- Hopewell P.C, Pai M, Maher D et al. (2006). International Standards for tuberculosis care. Lancet Infect. Dis,: 6; 710-725.
- Corbett E.L, Watt C.J, Walker N et al (2017). The growing burden of tuberculosis; global trends and interactions of with HIV epidemic, Archives of Internal Medicine, vol163, no.9pp1009-1021.
- Pillay T, Adhikari M. (2014). Congenital tuberculosis in a neonatal intensive care unit. Clin Infect Dis 2014; 29; 468-8.
- Cantwell M F, Sehab Z M, Costello A M ,Sands L ,Green W F ,Ewing E P et al (2014) Congenital tuberculosis. New England Journal of Medicine; 330 ;1051
Medical Journal of Zambia, Vol 49, 4
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.