A Comparative Review of the Efficacy of 24-Hour Versus 48-Hour Dose Regimen of Amoxicillin/Clavulanic Acid Prophylaxis for postoperative infections following elective Caesarean Section at the University College Hospital, Ibadan, Nigeria: A Randomized Clinical Trial
Olakunle Olawole Oloko
Department of Obstetrics and Gynaecology, University College Hospital
Olayinka Oladunjoye Ogunbode
Department of Obstetrics and Gynaecology, University College Hospital
Gbolahan Obajimi
Department of Obstetrics and Gynaecology, College of Medicine, University of Ibadan, Nigeria
Ayodele Arowojolu
Department of Obstetrics and Gynaecology, College of Medicine, University of Ibadan, Nigeria
DOI: https://doi.org/10.55320/mjz.49.4.388
Keywords:Elective Caesarean Section, Postoperative infection, Antibiotics prophylaxis, Antibiotics regimen.
ABSTRACT
Objectives: To compare the efficacy of 24hour versus 48hour prophylaxis of amoxicillin/clavulanic acid in the prevention of postoperative infections.
Study Design: This study was a randomized controlled clinical trial conducted in a tertiary hospital in Ibadan, Nigeria. Two hundred and fifty -two pregnant women scheduled for elective caesarean section were randomly assigned into two groups. After the initial pre-incision antibiotic administration, group A received the Amoxicillin/Clavulanic Acid for 24 hours while group B received the same drug for 48hours.
Main Outcomes: Participants were examined on the 3rd, 10th and 17th post-operative days for evidence of infections. All entry and analysis of data was by computer using the Statistical Package for Social Sciences version 22 (IBM, New York). Statistically significant differences were determined at p value of < 0.05.
Results: The incidence of postoperative wound infection, postoperative fever and endometritis in this study was 5.2%, 9.1% and 5.6% respectively. There was no significant differences in the incidence of postoperative wound infection, postoperative fever and endometritis between the two regimens of antibiotics.
Conclusion: A 24-hour prophylactic regimen of amoxicillin/clavulanic acid is adequate following caesarean section and prolonged use of antibiotics is generally unnecessary, costly and inadvertently increases antibiotics resistance.
INTRODUCTION
Caesarean section is one of the commonly performed surgical procedures in obstetric practice and has become the preferred route of delivery when compared to instrumental vaginal delivery in many developing and developed countries mainly due to reduced perinatal morbidity and mortality, lesser risk of litigations and increasing availability of required skills[1,2,3]. With the increasing practice of caesarean section, there is concomitant increased risk of post-operative infections which puts more burden on health care systems, coupled with other challenges which are frequently more encountered in Sub-Saharan Africa such as scarcity of skilled personnel, rudimentary facilities and financial constraints[2-4]. These postoperative infections, when present, leads to prolonged hospital stay, maternal morbidities and mortalities and increased cost of care to the patients[5-6].
Globally, sepsis accounts for approximately 11% of maternal deaths, and in Africa, puerperal sepsis had been documented to account for as high as 30.7% of maternal deaths[7-8]. Caesarean section is an important risk factor for postoperative maternal infection[2]. Worldwide, the incidence of postoperative infection following caesarean delivery ranges from 2-16% depending on the risk level[9]. Common bacterial pathogens that have been implicated in postoperative infection includes Staphylococcus Species, Enterococcus Faecalis, Escherichia Coli, Proteus Mirabilis and Pseudomonas Species[10,11].
Several pre-operative, intra-operative and post operative preventive measures such as preoperative antibiotics, chlorhexidine alcohol skin preparation, use of clippers instead of razor, preoperative vaginal cleansing, uterine exteriorization, removal of placenta by traction of umbilical cord, intra-abdominal irrigation, suture closure of subcutaneous tissue if wound thickness greater than 2 cm, prophylactic negative pressure wound therapy and dressing removal between 24 and 48 hours have proven to help to reduce the incidence of post-caesarean section infection[12]. Prophylactic antibiotics have been recommended generally for population of more than 5% incidence of postoperative infection[13].
Although prophylactic antibiotics have been found to be beneficial for women going for emergency caesarean section[7], controversy exists regarding the usefulness of antibiotic prophylaxis for women scheduled for elective caesarean section performed prior to rupture of membranes. This is more so as postoperative infection rates are lower following elective caesarean section when compared to those following emergency caesarean section[14]. This inconsistency from literature regarding the benefit of antibiotic prophylaxis for elective caesarean section still forms a basis for examination, even though some studies have suggested that caesarean section in itself, is a risk factor for postoperative infection whether emergency or elective[13]. Other areas of controversies include the choice, dosage, frequency, duration, offending organisms, sensitivity patterns and the time at which the antibiotic prophylaxis is commenced[15].
In the absence of risk factors, WHO recommends a single dose of intravenous prophylactic antibiotics for pregnant women scheduled for caesarean section and given 30-60 minutes before skin incision[16], yet some hospitals in the developing countries including the study centre, use antibiotics prophylaxis for 48 hours or more. Bacteria pathogens complicate 10% of postoperative infections following caesarean section despite antibiotics and over 80% of these postoperative infections occur after the patient has been discharged from the hospital[12-13], thus, maternal postoperative infections may be underestimated if based on hospital discharge records.
There is therefore a need for an updated prospective review of the antibiotic prophylaxis protocol based on randomized controlled clinical trial on postoperative infections after elective caesarean section. This study aimed to compare the efficacy of 24hour versus 48hour prophylaxis of amoxicillin/ clavulanic acid in the prevention of surgical site infection among pregnant women scheduled for elective caesarean section, in Ibadan, Oyo State, Nigeria, and to determine the incidence of post caesarean section operation site (wound) infection, postoperative fever and endometritis among women in the two groups.
METHODS
This was a randomized double-blinded, interventional, two-armed, single centre clinical trial conducted at the labour ward unit of the University College Hospital, UCH, Ibadan, Nigeria between 3rd May 2018 and 2nd April 2019. Ethical approval was obtained from the University of Ibadan/University College Hospital Institutional Review Committee (UI/EC/16/0291).
Sample size was calculated using the formula below for Randomized Controlled Trials (RTC)[17]. Randomization was done using a computer-generated allocation sequence[18] and they were allocated into group A(intervention) and group B (Control) receiving 24 hours and 48hour of prophylactic antibiotics, respectively. Group A additionally received placebo for the remaining 24 hours to avoid bias.
Two hundred and fifty-two patients scheduled for elective CS were recruited following informed consent. Patients with immunosuppressive disorders, fever, antibiotics use in the preceding week, allergies to amoxicillin/clavulanic, premature rupture of membranes and scheduled for emergency caesarean section were excluded from this study.
Elective caesarean section was performed either through a Pfannenstiel incision or a midline infraumbilical incision. Vicryl sutures were used for all the patients and the surgical incisions were cleaned with the same antiseptic and dressings applied. The antibiotics were administered by medical doctors who were not part of the investigators and other post-operative care were done as per protocol in the hospital. Temperature checks were done 4 hourly using digital thermometers and assessment for evidence of wound infection and endometritis were done on the 3rd, 10th and 17th postoperative days either as in-patients or out-patients.
Superficial wound infection was defined by the presence of purulent or serous discharge from the wound with indurations, warmth, and tenderness in the skin area[14] while febrile morbidity was defined by temperature of > 38 degree obtained on 2 or more occasions excluding the first 24 hours after delivery and endometritis was defined by a combination of fever, suprapubic tenderness and abnormal vaginal bleeding[19]. Those with postoperative complications were treated as per departmental protocol.
Data were collected using proforma that was designed by the investigators based on available information in literature. The data was cleaned before final analysis and Statistical Package for Social Sciences (SPSS-22.0 IBM New York) was used for analysis. An interim analysis was conducted to assess harm/benefit of the study, after recruiting a third of the required study participants and no participant suffered adverse outcome. The investigators were blinded from the study during the intervention follow up and data analysis phases of the study.
RESULTS
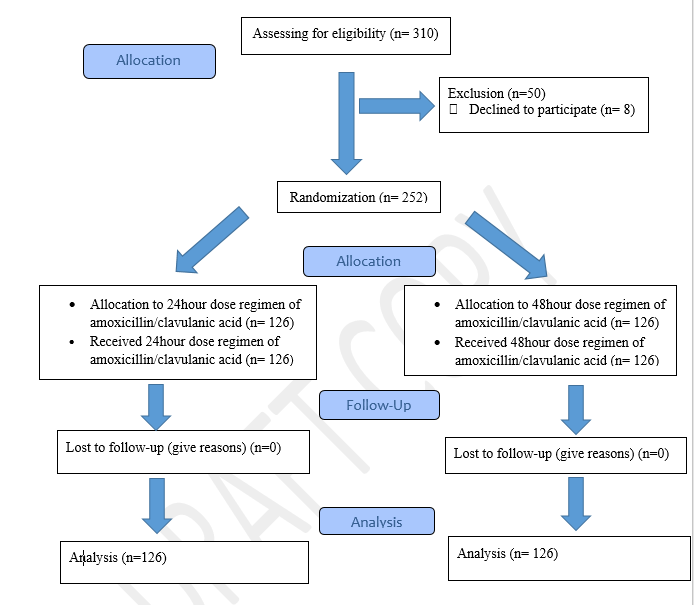
A total of three hundred and ten were assessed for eligibility but two hundred and fifty-two pregnant women who consented and met the inclusion criteria. Figure 1 shows the flow diagram of the progress through the enrolment, intervention allocation, follow-up, and data analysis phases of the study.
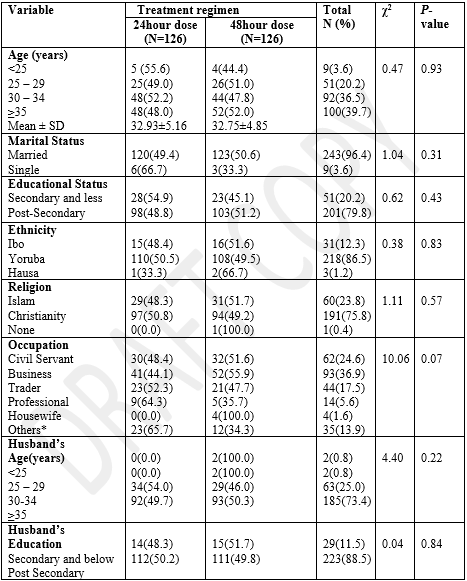
The mean age of the participants (32.93±5; 32.75±4.85) in years (SD) were similar in both groups. Most participants were in the age groups 30 – 35 years and ≥35years age groups. Similarly, most of the participants were married (120;123), had post-secondary education (98;103), and Yoruba ethnicity (110;108) in the two groups. Other selected socio-demographic characteristics are presented in Table 1.
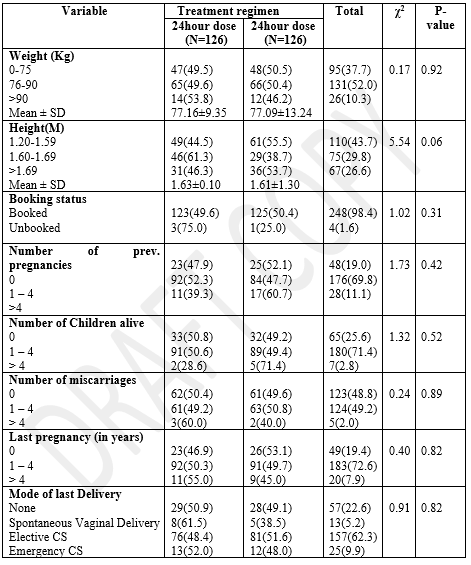
Majority of the participants in both groups were booked (123;125) and about half of the participants (52.3%;47.7%) were multiparous (para 1-4). The pattern was similar with those who had delivery by elective CS (48.4%;51.6%) during their last confinement. None of the obstetrics parameters were statistically significant and these are shown in Table 2.
Table 2: Reproductive characteristics of participants and comparison between 24hour dose regimen and 48hour dose regimen of amoxicillin / clavulanic Acid
The overall incidence of postoperative fever was 9.1%, endometritis was 5.6% and superficial wound infections were 5.2% respectively. (Figure 2).
Figure 2.showing the incidence of the selected primary outcome variables for the study.

Table 3 shows the primary outcome variables between participants who had a 24hour dose regimen of amoxicillin/clavulanic acid and 48hour dose regimen. For postoperative fever, those who took 24hour dose regimen 8(6.4%) were more likely to have fever on day 3 compared to those in 48hour dose regimen, 6(4.8%). This, however, was not statistically significant (p=0.58, RR = 1.3 (0.47-3.73). Similarly, those who took 24hour dose regimen 4(3.2%) were more likely to have fever on day 10 compared to those in 48hour dose regimen, 3(2.4%) p=1.0, RR = 1.3 (0.31-5.84). Also, those who took 24hour dose regimen 4(3.2%) were more likely to have fever on day 17 compared to those in 48hour dose regimen, 2(1.6%) day 17 (p=0.58, RR = 2.0 (0.37-10.72). However, this was not statistically significant.
Table 3:Primary outcome variables of participants, and comparison between 24hours dose regimen and 48hours dose regimen of amoxicillin/clavulanic acid study arms.
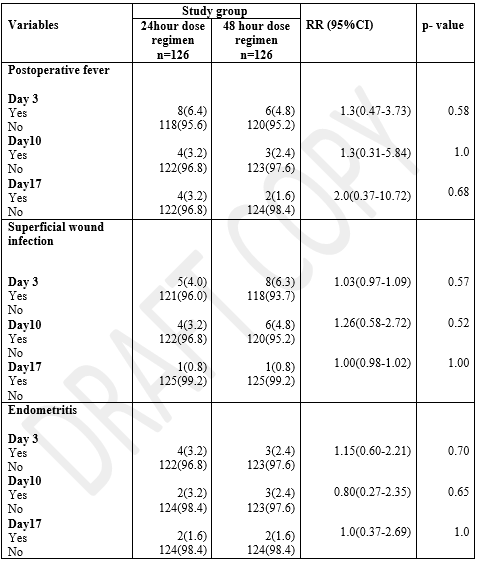
For superficial wound infection, those who took 24hour dose regimen 5(4.0%) were more likely to have superficial wound infection on day 3 compared to those in 48hour dose regimen, 8(6.3%). However, this was not statistically significant (p=0.57, RR=1.03 (0.97-1.09). Similarly, those who took 24hour dose regimen 4(3.2%) were less likely to have superficial wound infection on day 10 when compared to 6(4.8%) of the 48hour dose regimen (P value=0.52, RR = 1.3 (0.58-2.72). On day 17, 1(0.8%) participant in each study arm was likely to develop superficial wound infection (p=1.0, RR = 1.0 (0.98-1.02). However, this was not statistically significant.
Endometritis was one of the primary outcomes of the study. Four (3.2%) and 3(2.4%) of the participants developed endometritis on day 3 in the 24hour and 48hour dose regimen group respectively. This was not statistically significant (p=0.70, RR = 1.15 (0.60 – 2.21). Similarly, those who took 24hour dose regimen were less likely to have endometritis on day 10 (p=0.65 RR = 0.80 (0.27-2.35). On day 17, 2(1.6%) participants in both study arms were likely to develop endometritis. However, this was equally not statistically significant (p=1.0, RR = 1.0 (0.37-2.6).
DISCUSSION
Prophylactic antibiotics is one of the very important interventions adopted to prevent or reduce postoperative infection following surgery[10-20] and the study site being a tertiary hospital with a high caesarean section rate and with a well outlined protocol for the management of post-operative complications was a good choice for this study. In our study, the participants were representative of all the common diverse groups and thus the outcome has the potential for wide acceptance since minority groups were not excluded from the study.
The socio-demographic characteristics and reproductive characteristics had no statistical significance on the efficacy of the antibiotic prophylaxis in the prevention of postoperative infections, which was similar to the finding by Ajekweneh A et.al in Edo State, Nigeria[20]. A few other studies had found that women with a low level of education and low socio- economic status were more likely to develop postoperative infections[13-21]as they may be unable to maintain good post-operative hygiene and also may have difficulty in understating instructions by health care workers, thus affecting compliance. This observation was seen in this study as majority of the participants had tertiary level of education and by implication a wider exposure on the subject matter, which may have influenced their postoperative care and nutritional status, though education did not emerge as a key factor in this study in comparison to other studies[20-22].
Booking status had been shown to have a major role in antenatal, intrapartum and postnatal care of pregnant women[13]. From this study, over 90% of the participants were booked with no significant implication on the study groups. This may be due to fact that this study involved elective surgeries and the outcome might have been different when compared with emergency caesarean sections.
The overall incidence of superficial wound infection rate was 5.2% and there was variation in the occurrence of superficial wound infections on the different days of follow up amongst the participants. Most of the participants were observed to have superficial wound infection on the third day after the caesarean section. This may be because wound dressings were removed on the first and second post-operative days, leaving the 3rd day post-surgery as the earliest time for the detection of wound infections.
In this study, participants in the 48 hours dose regimen group had slightly higher rate of superficial wound infections 8(6.3%) when compared to the 24hours dose regimen group 5(4.0%), however, the overall rates of superficial wound infections amongst the 2 groups were similar to the 5.3% to 10% observed in other studies in Nigeria[11,20,22]. This was however lower compared to previous rates of 16.2% and 19.4% reported in Ibadan and Lagos respectively[13-23]. This may be due to the fact that our study involved only elective cesarean sections thus eliminating the risks of wound infections that are present in many cases of emergency cesarean sections. Furthermore, the antibiotic administered in this study is one of the most effective choices for prophylaxis.
The overall incidence of postoperative fever was 9.1% and paradoxically, this was lower in the 24hourprophylactic dose regimen (4%) compared to 6.3% in the other group. One would have expected a lower rate of febrile morbidity in the 48hours dose regimen prophylaxis group and this may point to other factors that may influence the efficacy of antibiotic prophylaxis apart from the duration of the administration of antibiotics. Some researchers in Nigeria have reported a much higher rate of postoperative fever which was attributed to malaria fever[13-24].
The incidence of endometritis among the 24hour group (3.2%) was slightly higher compared to the other group (2.4%) but this was not statistically significant. This may be attributable to the longer duration of administration of the antibiotics, however, further studies on other predictors of endometritis following caesarean section may be needed to explain this.
The study was a randomized clinical, double- blinded interventional trial carried out in a tertiary hospital and biases were reduced through randomization, use of placebo, comparison and matching of participants, blinding of the investigators as well as participants using coded allocation numbers. The study encountered some limitations such as a relatively small sample size and short duration of follow-up, however the strength of this study as a randomized controlled trial cannot be overemphasized.
CONCLUSION
This study has revealed no significant difference in the efficacy between the 24hour dose regimen and the 48hour dose regimen of amoxicillin/clavulanic acid for the prevention of postoperative infection following elective caesarean section. Furthermore, the prolonged administration of antibiotics prophylaxis beyond 24hours is not justified as it has cost implications especially in a low income country where resources are scarce, fees are paid out-off pocket and the likelihood of antibiotics resistance with prolonged use.
DECLARATION
FUNDING
This study was self-sponsored.
CONFLICT OF INTEREST
There is no conflict of interest in the conduct of this study.
ACKNOWLEDGMENT
We acknowledge the patients who accepted to be part of this study. Special thanks to the staff of the labour wards unit who notified the investigators whenever there was an eligible participant.
REFERENCES
- Charvalho, P.D.S., Bittár, M.H. and Stjernholm, Y.V. Indications for increase in caesarean delivery. Reprod. Health 2019; 16:1–6
- Mascarello, K.C., Horta, B.L. and Silveira, M.F. Maternal complications and cesarean section without indication: systematic review and meta-analysis. Rev. Saude Publica 2017; 51:1–12.
- Aiken, A.M., Karuri, D.M., Wanyoro, A.K. and Macleod, J. Interventional studies for preventing surgical site infections in sub-Saharan Africa - A systematic review. Int. J. Surg. 2012; 10:242–249.
- Opoku, B. Prophylactic Antibiotic during Caesarean Sections at Komfo Anokye Teaching Hospital, Kumasi. Ghana Med. J. 2017; 41:48–51.
- Betrán, A.P., Temmerman, M., Kingdon, C. et al. Interventions to reduce unnecessary caesarean sections in healthy women and babies. Lancet 2018; 392:1358–1368.
- Quinlan, J.D. and Murphy, N.J. Cesarean delivery: Counseling issues and complication management. Am. Fam. Physician 2015; 91: 178–184.
- Bonet, M., Souza, J., Abalos, E. et al. The global maternal sepsis study and awareness campaign (GLOSS): Study protocol. Reprod. Health 2018; 15:1–17.
- Ngonzi, J., Tornes, Y.F., Mukasa, P.K. et al. Puerperal sepsis, the leading cause of maternal deaths at a Tertiary University Teaching Hospital in Uganda. BMC Pregnancy Childbirth 2016; 16:1–7.
- Saeed, K.B.M., Greene, R.A., Corcoran, P. and O’Neill, S.M. Incidence of surgical site infection following caesarean section: A systematic review and meta-analysis protocol. BMJ Open 2017;7(1): 1–5.
- Ibrahim, W., Ahmed, M., Mervat, A. and Entisar, M. Effect of prophylactic antibiotics on preventing post caesarean section infection. J. Am. Sci. 2011;7: 5–7.
- Njoku, C. O. and Njoku, A. N. Microbiological pattern of surgical site infection following caesarean section at the university of calabar teaching hospital. Open Access Maced. J. Med. Sci. 2019; 7: 1430–1435.
- Kawakita, T. and Landy, H. J. Surgical site infections after cesarean delivery: epidemiology, prevention and treatment. Matern. Heal. Neonatol. Perinatol. 2017; 3:1–9.
- Morhason-Bello, I.O., Oladokun, A., Adedokun, B.O., Obisesan, K.A., Ojengbede, O.A., and Okuyemi, O.O. Determinants of post-caesarean wound infection at the university college hospital Ibadan Nigeria. Niger. J. Clin. Pract. 2009;12: (1) 1–5.
- Adaji, J., Akaba, G., Isah, A. and Yunusa, T. Short versus long-term antibiotic prophylaxis in cesarean section: A randomized clinical trial. Niger. Med. J. 2020; 61(4): 173-179.
- Dalton, E. and Castillo, E. Postpartum infections: A review for the non-OBGYN. Obstet. Med. 2014; 7: 98–102.
- WHO and USAID. WHO 2015 Summary of Recommended and Non-Recommended Practices to Prevent and Treat Maternal Peripartum Infections. 2015: Vol. 375.
- Hajian-Tilaki, K. Sample size estimation in epidemiologic studies. Casp. J. Intern. Med. 2011; 2:289–298.
- Saghaei, M. Random allocation software for parallel group randomized trials. BMC Med. Res. Methodol. 2004:4:1–6.
- Horan, T., Gaynes, R., Martone, W., Jarvis, W. and Emori, T. CDC definitions of nosocomial surgical site infections, 1992: a modification of CDC definitions of surgical wound infections. Infect Control Hosp. Epidemiol 1992; 13:606–608.
- Ezechi, O., Edet, A., Akinlade, H., Gab-Okafor, C. and Herbertson, E. Incidence and risk factors for caesarean wound infection in Lagos Nigeria. BMC Res. Notes 2009; 2:1–5.
- Braveman, P. and Gottlieb, L. The Social Determinants of Health: It’s Time to Consider the Causes of the Causes. Public Health Rep. 2014: Vol. 129.
- Hassan, K. O. and Alegbeleye, J. O. Post Caesarean Section Wound Infection and Microbiological Pattern at the University of Port Harcourt. Res. Obstet. Gynecol. 2018; 6: 1–8.
- Rabiu, K., Akinlusi, F., Adewunmi, A., Alausa, T. and Durojaiye, I. Risk factors for post-cesarean wound infection in a tertiary hospital in Lagos, Nigeria. Niger. Med. J. 2020; 61(5): 262-268.
- Mokuolu, O. A., Falade, C.O., Orogade, A.A. et al. Malaria at parturition in Nigeria: Current status and delivery outcome. Infect. Dis. Obstet. Gynecol. 2009; Article ID 473971;1-7.
Medical Journal of Zambia, Vol 49, 4
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.