Evaluation of Fine Needle Aspiration for diagnosis of Tuberculous Lymphadenitis in Children using the Xpert MTB/RIF Ultra at the University Teaching Hospitals Children's Hospital, Lusaka, Zambias
Andrew Chisanga
University Teaching Hospitals, Children's Hospital, Lusaka, Zambia
Evans Mpabalwani
University of Zambia School of Medicine.
Aaron Nyirenda
University Teaching Hospitals, Department of department of Pathology
Dabwitso Banda
Zambia National institute for Public health (ZNPHI).
Chishala Chabala
University of Zambia School of Medicine.
DOI: https://doi.org/10.55320/mjz.49.4.387
ABSTRACT
Background: Tuberculous Lymphadenitis (TBL) is the commonest form of Extra Pulmonary TB and poses diagnostic challenges in setting with no access to Histopathology. Our goal was to evaluate the diagnostic yield of Xpert MTB Ultra performed on lymph node aspirate obtained using Fine Needle Aspiration (FNA) in children with suspected TBL.
Methods: This was a cross-sectional study conducted at a tertiary and main referral hospital in Zambia. Children aged 6 months to 15 years with lymphadenopathy and presumed TBL were enrolled. FNA was performed and lymph node aspirate samples were analysed using XPERT MTB/RIF ULTRA. Data was collected and analysed as frequencies and percentages. Logistic regression was used to measure the odds of testing positive for MTB.
Results: Sixty one children were enrolled in the study, 34(55.7%) were males and a median age of 6 years (IQR: 3-11 years). Sixteen (26%) were diagnosed with TB, 7 on clinical basis while, one was positive on gastric lavage, five (31%) were positive for TB on lymph node FNA using Xpert MTB/RIF Ultra. Then, 3 were positive Histopathology, with one also positive on XPERT MTB/RIF Ultra. Alternative diagnosis included malignancies like lymphomas and acute Leukemias. While non malignant lymphadenopathy included, benign reactive lymphadenopathy and HIV associated lymphadenopathy. The prevalence of HIV among the children diagnosed with TB was 37.5% (6/16). Thirty one percent (5/16) of children with TB had a close contact with TB, OR=9.0 (95% CI: 1.3-77, p-value (<0.05).
Conclusion: TBL is not uncommon in children presenting with Lymphadenopathy. FNA is a less invasive, inexpensive technique and coupled with use of Xpert MTB/RIF Ultra has potential for early diagnosis of TBL, in a low resource setting with limited Histopathology services.
INTRODUCTION
According to the World Health Organization (WHO), Tuberculosis (TB) remains one of the leading causes of morbidity and mortality especially in low income countries, with about 10 million infections Worldwide. Children account for about a tenth of cases and yet almost 15% of the deaths[1-2] . Data for children in Zambia remains scanty, with low notifications and limited reports on actual incidence and proportion especially of Extra Pulmonary Tuberculosis (EPTB)[3] . Bacteriological confirmation of tuberculosis in children is challenging and mainly utilizes clinical and radiological findings; both neither specific nor sensitive. TB in children is paucibacillary disease resulting in low sensitivity of standard diagnostic tests for TB[4-5] .
TB lymphadenopathy (TBL) is the commonest manifestation of EPTB, commonly affecting children below the age of 10 years, with cervical lymphadenopathy being the predominant site involved[6-7] . In endemic areas, TBL can account for as much as 60% of all forms of EPTB, with risk higher in children who are immunocompromised[7] .
In low resource settings, definitive diagnosis of TBL in children is often difficult because of limited availability of surgical and histopathology facilities when a lymph node biopsy is required. Fine needle aspirate (FNA) has demonstrated to be a key diagnostic tool in establishing a diagnosis of TBL[8-9] .
The introduction of Xpert MTB/RIF(Gene Xpert) as a cartridge based Nucleic Acid Amplification Automated Test (NAAT) revolutionized the diagnosis of TB for both pulmonary and extra-pulmonary samples including FNAs, as it could process samples, detect MTB DNA and rifampicin resistance in less than two hours[11] . As systemic review of the performance of Xpert MTB/RIF on extra pulmonary samples, showed a pooled sensitivity of 96% (95%, CI)
However, it had limited sensitivity in individuals with paucibacillary disease and those living with HIV, this necessitated the introduction of Xpert/MTB/RIF Ultra (Xpert Ultra) which has a higher sensitivity that approximates that of the gold standard, culture, with much less turnover time[12] .
Studies involving the performance of Xpert Ultra in both adult and paediatric populations have focused on respiratory samples with paucity of data on lymph node aspirates in children with suspected TBL[13,14,15] . FNA provides a less invasive way of obtaining samples for analysis making it suitable for a possible effective tool in diagnosing EPTB, specifically TB adenitis. FNAs analysed using a tool like Xpert Ultra with established good sensitivity in low bacillary disease provides a possibility of quick diagnosis of TB and early institution of treatment[12,16,17] .
METHODS
Study setting and recruitment
This was a cross sectional study of children with suspected TBL at the University Teaching Hospitals, Children’s Hospital Lusaka, Zambia a tertiary referral hospital and included children reviewed in the inpatient and outpatient departments. The study was conducted between August, 2020 and March, 2022. Children presenting with lymphadenopathy (one or more lymph nodes greater or equal to 1cm)[18] between the ages of 6 months and 15 years were referred for suspected TBL or for Lymph node biopsy were recruited. However, children with lymphadenopathy but on already on Anti tuberculous treatment or confirmed TB in other sites were excluded. HIV counseling and testing was done as part of routine care. Physical examination was done including anthropometry. Then FNA was done and sample was analysed with Xpert Ultra. Children found positive for TB were treated as per national guidelines[6] . Children negative for TB were then recommended for possible biopsy by paediatric surgeons through their managing units. Biopsies were further sent for histopathology. Further, respiratory samples collected and X-rays done by managing units were tracked and results recorded.
Fine needle Aspirate procedure
Under aseptic conditions, a 21-G needle attached to a 10cc syringe was used by the study physician. The enlarged lymph node was then fixed in position and needle inserted and obtained the aspirate. Aspirate was washed into a labeled specimen bottle with 1ml of normal saline and was sent to the TB laboratory for immediate analysis with Xpert Ultra.
Histology examination of lymph node Biopsies
Standard histopathology preparation was done as follows: specimen reception, gross examination, tissue processing, tissue embedding, microtomy, tissue staining, slide mounting, microscopic examination and report generation. Following gross examination of specimen sections of the tissue samples were taken and placed in cassette for processing with formalin, alcohol and xylene and Paraffin wax. The tissue was then embedded and placed on a mold to form a paraffin wax tissue block called formalin fixed paraffin embedded (FFPE) tissue block. Three micrometer slices of tissue were made, stained, dried and later examined by pathologists. Caseating granulomatous inflammation was suggestive of histomorphological manifestations of Mycobacterial tuberculosis. An alternative diagnosis to TB was reported as such.
Statistical analysis
Data was collected on the study questionnaire and entered into an electronic data base (Excel Sheet). Double data entry on excel sheet was then analysed using R4.1.3 software for windows.
| Goal of analysis | Non-parametric test |
|---|---|
| To describe each group categorical variable | Fishers exact test |
| To compare continuous variables | Mood’s Median test |
| To make an association between clinical characteristics | Fisher exact test |
| To rule out confounders | Multiple logistic Regression |
RESULTS
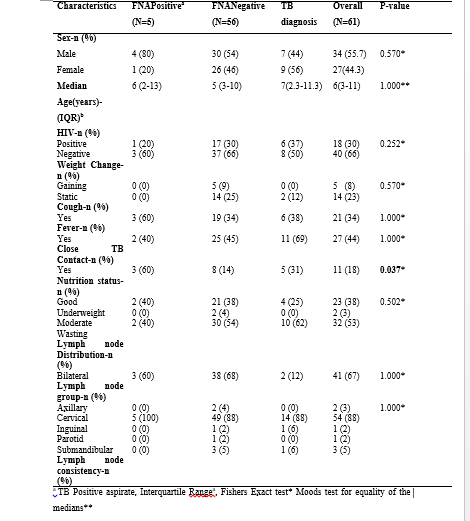
We screened a total of 70 Children of which 61 met the inclusion criteria and were enrolled in the study. FNAs were done on all the enrolled children and specimen samples were subjected to Xpert MTB/RIF/Ultra. Lymph node biopsy was recommended to participants who were negative for MTB on Xpert/ ultra, only 23 consented to Biopsy and had final report ready by the end of the study. When indicated, Bone marrow biopsy was done by the managing unit as part of the investigation for Lymphadenopathy. Table 1 highlights the characteristics of the children enrolled in the study.
Table 1: Clinical characteristics of Children enrolled

Laboratory and histology results for Children with Lymphadenopathy
A total 33 respiratory samples were collected from the participants for screening for TB. Of the five participants that were diagnosed with TB by FNA, two had positive respiratory samples for TB as well. Further, of the 16 participants whose final diagnosis was TB, 8 had bacteriological confirmation while 8 were diagnosed clinically as per national guidelines[6] .. Rifampicin resistance was detected on one respiratory sample and on one FNA sample processed with XpertMTB/RIF Ultra.
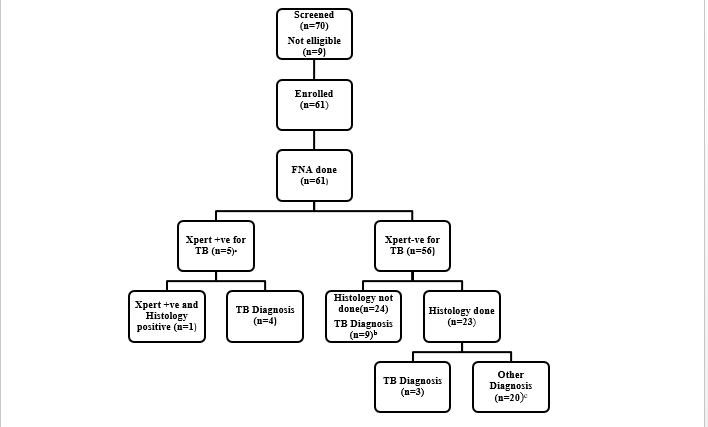
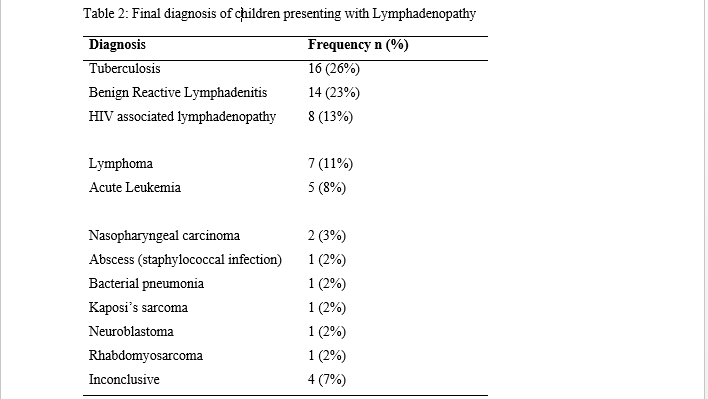
Table 2: Final diagnosis of children presenting with Lymphadenopathy
DISCUSSION
The study showed Xpert Ultra identified one third of children with TBL from samples obtained using FNA out of the total number of children with TB as the final diagnosis. There was no difference in yield between HIV positive children in comparison with those who were HIV negative. Xpert Ultra detected MTB in a third of samples that were positive on histology. There were no clinical features that were unique to children with positive Xpert/ultra-aspirates in comparison to those that that had an Xpert/ultra-negative aspirate but with a final diagnosis of TB.
The yield of Xpert Ultra on lymph node samples using FNA from our study was similar to a Gambian study involving 131 children with persistent lymphadenopathy, FNA showed 42.7% positivity for TB, though ZN staining and culture were used for diagnosis[19] . A much lower positivity however was noted in a European study with a much larger sample size[20] . Our study findings were comparable with South African study with similar sample size, though generic Xpert MTB/ RIF was used instead of Xpert Ultra (21). Similarly, in a Zambian study, Xpert MTB/RIF showed a positivity of 28% on formalin fixed lymph nodes of both adults and children[22] . However, an Indian study demonstrated 10% positivity for TB on lymph node aspirates but this particular study involved both respiratory and non-respiratory samples and was not restricted to children with lymphadenopathy[23] . Two South African studies however, demonstrated a much higher yield with Xpert MTB/RIF with both demonstrating a positivity of greater than 50%. In one of two studies, lymph node aspirates from children, while in the other samples were collected from both children and adults[21-24] . The higher prevalence of TB in South Africa could explain the higher positivity in these two studies[1] . The majority of studies involving Xpert MTB/RIF ultra have been done in adults and involved respiratory samples with paucity of data on extra pulmonary sample especially involving Children[13,14,15].
Children with HIV especially in sub-Saharan Africa, with a high burden of HIV are at a significantly increased risk of developing TB[4-25] .Six (37.5%) of the children diagnosed with TB were HIV positive. This included one of the 5 children positive on Xpert Ultra was HIV positive. Our findings were consistent with other studies which have demonstrated prevalence of TB in HIV infected children to be around 10-60%Children with HIV especially in sub-Saharan Africa, with a high burden of HIV are at a significantly increased risk of developing TB[4-25].Six (37.5%) of the children diagnosed with TB were HIV positive. This included one of the 5 children positive on Xpert Ultra was HIV positive. Our findings were consistent with other studies which have demonstrated prevalence of TB in HIV infected children to be around 10-60%[25-26] .
Of the lymph node biopsies done, 3 were positive for TB one of which had a positive lymph node aspirate for TB as well. Studies comparing FNAs with Xpert MTB/RIF and Histopathology have demonstrated a sensitivity varying from 30- 85%[27-27].
The median age of children with TB was 7years (IQR 2.3-11.3years) with an almost equal sex distribution. A close TB contact was a significant factor with asymmetrical, firm non-tender cervical lymphadenopathy being a common finding. These findings were consistent with other studies in similar setting[8,19,29].
A systemic review and meta-analysis of causes of Cervical lymphadenopathy in over 2000 children revealed non- specific benign causes were the commonest (68%) followed by viral infections. TB was the commonest cause of granulomatous disease with Lymphomas accounting for half of the malignancies[18]. Our findings were not very different, as benign reactive lymphadenopathy together with HIV associated Lymphadenopathy were the commonest causes of lymphadenopathy in children enrolled in our study. Further Lymphomas were the commonest malignancies found Seconded by Acute Leukemias. And similar results were noted by a study done in Sudan[30].
Our main limitation was the fact that FNA samples of lymph nodes were not subjected to culture which is the Gold standard in addition to the fact that the study was restricted to the UTHs-CH and was not a multicenter study. Only about two thirds of the desired numbers of children were enrolled, owing to the fact that the study was conducted during Covid-19 waves which led to the suspension of some of the hospital activities resulting in reduced patient in-flow. Further, not all patients being followed up by the managing units had respiratory samples collected or on chest x-ray done as part of their TB workup. This could have had implications in the final diagnosis.
The combination of FNA, which is readily available and inexpensive tool with Xpert MTB/ Ultra was able to detected MTB in a population with paucibacillary disease was a major strength of our study. The implication therefore, being the advocating of FNA to be utilized as an investigating tool for screening children with lymphadenopathy for TB especially in a low resource setting.
CONCLUSION
TBL is not an uncommon finding in children presenting with cervical lymphadenopathy in a TB endemic setting with FNA providing a non-invasive, non-labour intensive and quick way of obtaining the samples. Xpert Ultra is a useful tool in detecting MTB in paucibacillary disease in a low resource setting with an added advantage of detecting rifampicin resistance and comparable with histology.
ACKNOWLEDGEMENTS
We extend or gratitude to the Management at the UTHs-Children’s Hospital for having given us the opportunity to conduct the research at the Hospital. Finally, the department of Pathology and laboratory staff as well as parents and guardians of all the participants.
REFERENCES
- World Health Organisation. Global Tuberculosis Report 2021. Geneva; 2021.
- Dodd PJ, Yuen CM, Sismanidis C, Seddon JA, Jenkins HE. The global burden of tuberculosis mortality in children : a mathematical modelling study. Lancet Glob Health. 2017 Sep;5(9):e898–e906.doi:10.1016/S2214-109X(17)30289-9.
- Kapata N, Chanda-Kapata P, O’Grady J, Bates M, Mwaba P, Janssen S, et al. Trends in childhood tuberculosis in Zambia: A situation analysis. J Trop Pediatr. 2013;59(2):134–9. doi:10.1093/tropej/fms065.
- Ritz N, Curtis N. Novel concepts in the epidemiology , diagnosis and prevention of childhood tuberculosis. Swiss Med Wkly. 2014 Sep 10;144:w14000. doi:10.4414/smw.2014.14000.
- Roya-pabon CL, Perez-velez CM. Tuberculosis exposure , infection and disease in children : a systematic diagnostic approach. Pneumonia (Nathan). 2016 Nov24;8(23).doi:10.1186/s41479-016-0023-9.
- Republic of Zambia National Tuberculosis and Leprosy Control Program Guidelines for Management of Tuberculosis in Children. 2016. ( 1st ed). p1–22. Ministry of Health Zambia.
- Cruz AT, Starke JR. Pediatric Tuberculosis. Pediatr Rev. 2010 Jan;31(1):13–25; quiz 25-6. doi: 10.1542/pir.31-10-13.
- Graham SM (2016). The union’s desk guide for diagnosis and management of tb in children. (3rd ed). p1–17 . International Union Against Tuberculosis and Lung diseases(The Union) 68 Boulevard Saint-Michel,75006 Paris,France.
- Khan S, Liomba G, Rosenberg NE, Stanley C, Kampani C, Dhungel BM, et al. Utilization of fine needle aspiration cytology at Kamuzu Central Hospital. PLoS One. 2018 Jun;13(6):e0196561.doi: 10.1371/journal.pone.0196561.
- Wright CA, Pienaar JP, Marais BJ. Fine needle aspiration biopsy: diagnostic utility in resource-limited settings. Ann Trop Paediatr. 2008 Mar;28(1):65–70. doi:10.1179/146532808X27070707.
- World Health Organisation. Xpert MTB/RIF Implemenation Manual: Technical and operational “how to”: Practical consideration. Geneva; 2014.
- World Health Organisation. WHO meeting report of a technical expert consultation: non-inferiority analysis of Xpert MTB/RIF Ultra compared to Xpert MTB/RIF. Geneva; 2017. Available from: http://apps.who.int/iris/bitstream/10665/254792/1/WHO-HTM-TB-2017.04-eng
- Atherton RR, Cresswell F V, Ellis J, Kitaka SB, Boulware DR. Xpert MTB / RIF Ultra for Tuberculosis Testing in Children : A Mini-Review and Commentary. Front Paediatr . 2019;7(34):1–6. Available from: www.frontiersin.org
- Dorman SE, Schumacher SG, Alland D, Nabeta P, Armstrong DT, King B, et al. Xpert MTB/RIF Ultra for detection of Mycobacterium tuberculosis and rifampicin resistance: a prospective multicentre diagnostic accuracy study. Lancet Infect Dis. 2018 Jan;18(1):76–84. doi:10.1016/S1473-3099(17)30691-6.
- Antel K, Oosthuizen J, Malherbe F, Louw VJ, Nicol MP, Maartens G, et al. Diagnostic accuracy of the Xpert MTB / Rif Ultra for tuberculosis adenitis. BMC Infect Dis. 2020 Jan 13;20(1):33.doi:10.1186/s12879-019-4749-x.
- Patel JM, Patel KR, Shah K, Patel NU, Baria H, Patel PD. Comparison of fine-needle aspiration technique with Ziehl-Neelsen stains in diagnosis of tuberculous lymphadenitis. Int J Med Public Health. 2015;4(3):400–3.
- Wright CA, Hesseling AC, Bamford C, Burgess SM, Warren R, Marais BJ. Fine-needle aspiration biopsy : a first-line diagnostic procedure in paediatric tuberculosis suspects with peripheral lymphadenopathy? Int J Tuberc Lung Dis. 2009;13(11):1373–9.
- Deosthali A, Donches K, Delvecchio M, Aronoff S. Etiologies of Pediatric Cervical Lymphadenopathy : A Systematic Review of 2687 Subjects. Glob Pediatr Health. 2019; 6: 2333794X19865440.
- Fanny M, Beyam N, Gody JC, Zandanga G, Yango F, Manirakiza A, et al. Fine-needle aspiration for diagnosis of tuberculous lymphadenitis in children in Bangui , Central African Republic. BMC Pediatr. 2012;12(191):1–4. Available from: http://www.biomedcentral.com/147-2431/12/191.
- Puiu I, Stancu P, Nicolescu VE, Stoian F, Craiova P. Diagnosis of Tuberculosis Adenitis in children. Pediatrics. 2008;121(Supplement_2): S130–S131.doi:10.1542/peds.2007-2022rrrr.
- Coetzee L, Chb MB, Nicol MP, Jacobson R, Wright CA, Path FRC. Rapid Diagnosis of Pediatric Mycobacterial Lymphadenitis Using Fine Needle Aspiration Biopsy. Pediatr Infect Dis J. 2014 Sep;33(9):893-6. doi: 10.1097/INF.0000000000000312.
- Polepole P, Kabwe M, Kasonde M, Tembo J, Shibemba A, Grady JO, et al. Performance of the Xpert MTB / RIF Assay in the Diagnosis of Tuberculosis in Formalin fixed , Paraffin embedded Tissues. Int J mycobacteriology. 2017 Jan-Mar;6(1):87–93. doi:10.4103/2212-5531.201892.
- Das A, Anupurba S, Mishra O P, Tuhina Banerjee T, Tripathi R. Evaluation of Xpert MTB/RIF assay for diagnosis of Tuberculosis in Children. J Trop Pediatr. 2019 Feb1;65(1):14–20. doi:10.1093/trope/fmy005.
- Ligthelm LJ, Nicol MP, Hoek KGP, Jacobson R, Helden PD Van, Marais BJ, et al. Xpert MTB / RIF for Rapid Diagnosis of Tuberculous Lymphadenitis from Fine-Needle-Aspiration Biopsy Specimens. J Clin Microbiol. 2011 Nov;49(11):3967–70. doi:10.1128/JCM.01310-11.
- Corbett EL, Watt CJ, Walker N, Maher D, Williams BG, Raviglione MC, et al. The Growing Burden of Tuberculosis. Arch Intern Med. 2003 May12;163(9)1009–21.10.1001/archinte.163.9.1009.
- Berti E, Galli L, Venturini E, Martini M De, Chiappini E. Tuberculosis in childhood : a systematic review of national and international guidelines. BMC Infect Dis. 2014;14(Suppl 1):S3. Available from: http://www.biomedcentral.com/1471-2334/14/S1/S3.
- Sarfaraz S, Iftikhar S, Memon Y, Zahir N,HerekerFF,Salahuddin N. Histopathological and microbiological findings and diagnostic performance of GeneXpert in clinically suspected tuberculous lymphadenitis. Int J Infect Dis. 2018;76:73–81. Available from: https://doi.org/10.1016/j.ijid.2018.08.020.
- Raja R, Sreeramulu PN, Dave P, Srinivasan D. Journal of Clinical Tuberculosis and Other Mycobacterial Diseases GeneXpert assay – A cutting-edge tool for rapid tissue diagnosis of tuberculous lymphadenitis. J Clin Tuberc Other Mycobact Dis. 2020;21:100204. Available from: https://doi.org/10.1016/j.jctube.2020.100204.
- Shah I, Dani S. Profile of tuberculous cervical lymphadenopathy in children. J Trop Pediatr. 2017 Oct 1;63(5):395–8. doi:10.1093/tropej/fmx001.
- Ahmed HG, Elmubasher MB, Salih RA, Elhussein GE, Ashankyty IM. Fine Needle Aspiration Cytopathology of Pediatric Lymphadenopathy among Sudanese Children. Asian Pac j Cancer Prev. 2013;14(7):4359–63. doi:10.7314/apjcp.2013.14.7.4359.
Medical Journal of Zambia, Vol 49, 4
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.