Effects of angiotensin receptor blockers and angiotensin-converting enzyme inhibitors on respiratory Mucin-5ac, Mucin-C5b and Forkhead box protein A2 of a hamster tracheal mucosa
Lumamba Mubbunu
University of Zambia, School of Veterinary Medicine, Department of Biomedical Sciences.
Copperbelt University, Michael Chilufya Sata School of Medicine, Department of Basic Sciences.
Edwell Mwaanga
University of Zambia, School of Veterinary Medicine, Department of Paraclinical Studies.
Bernard Hang’ombe
University of Zambia, School of Veterinary Medicine, Department of Paraclinical Studies.
Seter Siziya
Copperbelt University, Michael Chilufya Sata School of Medicine, Department of Public Health.
Humphrey Simukoko
University of Zambia, School of Veterinary Medicine, Department of Biomedical Sciences.
DOI: https://doi.org/10.55320/mjz.50.1.386
Keywords:MUC5AC, MUC5B, FOXA2, ARB, ACE inhibitor, Losartan and Enalapril.
ABSTRACT
Backgroud: Respiratory mucosal surface is continuously exposed to inhaled pathogens, and a protective layer of secreted mucus acts as the first line of defense against infection through a mechanism called mucociliary clearance. Mucus hypersecretion can negatively affect mucociliary clearance. Although ARBs and ACEIs are associated with induction of cough and angioedema as their side effects, no studies were found that show the effects of these drugs on Mucin-5ac, Mucin-5b, and Forkhead box protein A2. Mucin-5ac and mucin-5b are the main mucins in respiratory mucus and the viscoelasticity properties of respiratory mucus depends on them.
Methods: This study used a hamster as an animal model to investigate the effects of ARB and ACEI on respiratory mucin-5ac, mucin-5b, and Forkhead box protein A2. Enalapril and Losartan were used as representative drugs for ACEIs and ARBs, respectively. The concentrations of mucin-5ac, mucin-5b, and Forkhead box protein a2 were measured using ELISA. Dunnet’s t-test was used to analyze the results.
Results: Enalapril and Losartan increased mucin-5ac and mucin-5b, but the increase was not significant compared to the control (p > 0.05). However, enalapril and Losartan decreased the concentration of Forkhead box protein a2, but the decrease was not significant compared to the control (p > 0.05).
Conclusions: The study found that, administration of enalapril or losartan did not have a significant effect on the concentration of Mucin-5ac, Mucin-5b, and Forkhead box protein A2. Therefore, the administration of these drugs will not reduce mucociliary clearance of the respiratory tract through the impairment of mucus production.
INTRODUCTION
The respiratory mucosal surface is continuously exposed to inhaled pathogens, and a protective layer of secreted mucus acts as a first line of defense against infection[1] . Abnormalities in mucus secretion, including increased expression of the major airway mucins mucine-5ac (MUC5AC) and mucine-5b (MUC5B), are an important characteristic of inflammatory airway diseases[2] . In chronic inflammatory respiratory disorders, MUC5B and MUC5AC increase[3] . A higher ratio of MUC5AC to MUC5B is correlated with type 2 inflammation[4] . Type 2 inflammation describes an inflammatory pathway involving a subpopulation of CD4+ T cells known as Th2 cells that secrete IL-4, IL-5, and IL-13 and stimulate Type 2 immunity, which is characterized by high IgE antibody titers and eosinophilia. MUC5B and MUC5AC are major matrix-forming macromolecules in airway mucus, due to this, the viscoelastic properties of airway mucus depend on MUC5AC and MUC5B[5] . The advent of Coronavirus disease 2019 (COVID-19) has brought with it new challenges, especially for people with existing respiratory and cardiac diseases related to the use of angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin receptor blockers (ARBs)[6] . ARBs and ACEIs are widely used in patients with hypertension and other cardiovascular diseases to improve the quality of life of affected persons[7] . Studies have shown that severe cases of covid-19 were observed in patients with hypertension, kidney disease, and diabetes mellitus[6] . There are controversies as to why this was the case, and the role of angiotensin receptor blockers (ARBs) and angiotensin enzyme inhibitors (ACEIs) is not being ruled out as a contributing factor[8] . Among the most recognized examples of adverse side effects of ACEIs are cough and angioedema, both of which are associated with elevated levels of bradykinin in patients taking these drugs[9] . Bradykinin is elevated in these patients because inhibition of angiotensin converting enzyme (ACE) inadvertently means that bradykinin inactivation is down-regulated since ACE is involved in bradykinin inactivation[10] . Increased bradykinin promotes vascular leakage and fluid extravasation; this, in turn, can lead to pulmonary edema and inflammation.
Bradykinin is an inflammatory mediator through which ACEIs, and ARBs can act to affect the mucins of the tracheal mucosa. Bradykinin is a potent, transient vasoactive peptide that acts as a vasodilator and an inflammatory mediator in various signaling cascades[11] . Bradykinin contracts airway smooth muscles, increases microvascular leakage, and stimulates mucus secretion[12 - 13] . Furthermore, inflammatory conditions such as angioedema may deplete FOXA2 expression and lead to hyperplasia of goblet cells and submucosal glands, thereby leading to hyper-secretion of respiratory mucus[14] . Increased secretion of mucus in the trachea can negatively affect mucociliary clearance. Mucociliary clearance system includes two major functional mechanisms; these are, ciliary beating and mucous secretion systems, each of which is usually complimentary and cooperative. In addition, mucociliary system is made possible because of the airway surface liquid (ASL). The ASL is a thin fluid layer that covers the airway surface at the interface between epithelial cells and air space[15] . The ASL is important in regulating airway pH, ciliary function and mucociliary activity. The airway surface liquid is made up of two layers, namely the mucus layer and the periciliary layer. The mucus layer is made up of gel-forming mucins MUC5AC and MUC5B which trap and remove inhaled particles from the airway system. Mucociliary clearance is the primary defense mechanism that protects airways from inhaled infections and toxic agents[1] . Mucus hyper-secretion negatively affects the mucociliary clearance system by increasing the viscosity of the mucus. Although ARBs and ACEIs are associated with a dose dependent induction of cough and angioedema as their side effects, no studies were found that show the effects of ARBs and ACEIs on Mucin-5ac, Mucin-5b and Forkhead box protein A2 of the respiratory system, especially in the wake of COVID-19 pandemic.
This study aimed to use a hamster (Mesocricetus auratus) as the animal model to investigate the effects of angiotensin receptor blockers (ARBs) and angiotensin converting enzyme inhibitors (ACEIs) on respiratory MUC5AC, MUC5B and FOXA2 of the hamster tracheal mucosa. Enalapril and Losartan were used as representative drugs for ACEIs and ARBs, respectively. The concentrations of MUC5AC, MUC5B, and FOXA2 were studied as response variables.
MATERIALS AND METHODS
Study Design and Setting
This was a post-test only control group study design that was carried out in the Biochemistry laboratory of the School of Veterinary Medicine of the University of Zambia. The objective of this study was to compare the expression of FOXA2, MUC5AC and MUC5B in the trachea of hamsters treated with ACEIs or ARBs versus those that had not been treated. The hamsters were randomly put in three groups of six. The hamsters that were used for the study were moved from the common housing to a separate non-infectious room during the period of the study.
Experimental groups were as follows:
1. Group 1 was six hamsters treated with distilled water, these served as the control group.
2. Group 2 was six hamsters treated with Enalapril 12mg/L.
3. Group 3 was six hamsters treated with Losartan 28mg/L.
The ethical clearance was granted by the University of Zambia Biomedical Research Ethics Committee (UNZABREC) IRB00001131 of IORG0000774. The approval number for the study is REF. No. 2504-2022. Further permission to carry out the study was granted by the National Health Research Authority Ref No: NHRA0000005/08/04/2022.
Study Variables
Concentration of respiratory Mucin-5ac (MUC5AC), mucin-5b (MUC5B) and Forkhead box a-2 (FOXA2).
Sample Population Calculations
The sample population was calculated using the “resource equation” method[16] . In this method, the degree of freedom of analysis of variance (ANOVA) (E) should lie between 10 and 20. If E is less than 10 then adding more animals will increase the chance of getting a more significant result, but if it is more than 20 then adding more animals will not increase the chance of getting significant results. E = N – k = kn – k = k (n – 1), where N = total number of subjects, k = number of groups, and n = number of subjects per group. Rearranging the formula, n is given as: n = E/k + 1
a) Minimum sample size= 10/3 + 1=4.3 rounding off = 4 animals per group.
b) Maximum sample size=20/3 + 1 = 7.7 rounding off = 8 animals per group.
The sample size per group was calculated to be between 4 and 8 animals per group. The average (4 + 8) / 2 = 6 animals per group were used in this study.
Drug Dose Calculation
The drugs used in this study were Enalapril maleate, which is an ACEI, and Losartan potassium, which is an ARB. The dose of the drugs was calculated from the maximum recommended dose for human treatment.
Enalapril: The maximum recommended dose is 40 mg per day[17] .
• 40 mg per day translates to 0.58mg/kg/day taking 70 kg as maximum body weight to calculate the drug dosage[18] .
• The water consumption of the Syrian male hamster is 5ml/100g body weight/day, and the female is 13.5 ml/100g body weight/ day[19] .
• The mean weight of the Syrian male hamster is 100 g[20] ; furthermore, a male hamster drinks 5ml/100g body weight of water, therefore, the dose of enalapril in drinking water to give an oral dose per day equivalent to 0.58 mg/kg/day is as follows:
0.58mg/1000g x 100g =0.058mg per day per hamster. Dissolved in water will be 0.058mg/5ml = 0.0116 ≈ 0.012mg/ml. converting this to mg/liter. 0.012mg/ml x.
1000ml/L = 12mg/L. Male hamsters were given 12mg/L of Enalapril in drinking water for four weeks.
Losartan: The maximum recommended dose for losartan is 100 mg per day[21] . Following the calculations done above, 100 mg per day translates to 1.4mg/kg/day in male hamsters. The dose of Losartan in drinking water was calculated to be 28 mg / L, which was equivalent to an oral dose of 1.4mg/kg/day.
Note: Dosage of drugs: Enalapril 12mg/L and Losartan 28mg/L in drinking water.
Animal Treatment and Control Groups
For this study,18 male hamsters were used. Male hamsters were used to reduce confounders that may arise due to the oestrous cycle in female hamsters[22] . In addition, male hamsters were used to reduce the chances of using a pregnant hamster during the study. The hamsters were randomly separated into three (03) groups of six (06). A group of hamsters was equal to six hamsters for purposes of this study. The drugs that were used in the study were Enalapril Maleate USP 20mg manufactured by LIFEON LABS PVT, LTD India; Zambia Medicines Regulatory Authority (ZAMRA) reg no.201/028 and Losartan Potassium USP 50mg manufacture by Emcure Pharmaceuticals: ZAMRA reg no.195/010. One group of six (06) hamsters was treated with Enalapril 12mg/L in drinking water for 30 days, and another group of six (06) was treated with Losartan 28mg/L in drinking water for 30 days. The last set of six (06) of hamsters was given distilled water; this served as the control group. The drugs that were administered to the hamsters were dissolved in distilled water. The dosage for the drugs was calculated from the maximum recommended dose in treating humans. For Enalapril, the maximum recommended dose is 40mg per day[18] , while that of Losartan is 100mg per day[21] . The hamsters had free access to food and water which contained drugs for the experimental animals and distilled water for the control animals. Distilled water was given to the control hamsters because the experimental hamsters received drugs dissolved in distilled water; thus, the only difference in drinking water between the experimental hamsters and the control was the dissolved drugs. The hamsters were feed with Nutrisure commercial pellets manufactured by NUTRIFeeds Zambia Limited, with a formulation of moisture content of 120g/kg-crude protein maximum, 13g/kg lysine maximum, 6.5g/kg-crude fat, 30/40g/kg-min/max crude fiber, 120g/kg-calcium, 10/12g/kg min/max and phosphorus- 6g/kg-minimum. The hamsters were kept in cages with paper litter and the litter was changed twice every week during the study.
Removal of the Trachea
The trachea was removed from the sacrificed animals by cutting it from the larynx to the tracheal bifurcation following the procedure described by Parkinson et al[23] . An overdose of general anesthesia (xylazine 10mg/kg body weight[24] ) was administered to the hamsters until no pedal withdrawal reflexes were present. The trachea was removed by making an incision cranially and caudally along the ventral midline that spanned from the chin to the pubis. Blunt dissection was used to remove nontracheal-associated tissue. The larynx was removed by making a transverse cut below the cricoid cartilage using a micro-dissecting scissors. Furthermore, the left and right primary bronchial branches were removed by making a transverse cut just above the carina using a micro-dissecting scissors. After removal, the trachea was placed in 2.0 ml of ice cold HIMEDIA phosphate buffer saline (PBS) pH 7.0.
MUC5AC, MUC5B AND FOXA2 Extraction
The tracheal tissue was rinsed in fresh PBS and then it was homogenized in 2.0 ml ice-cold PBS pH 7.0. The homogenates were centrifuged for 5 minutes at 5,000 rpm, 4°C. The supernatant was removed, aliquoted in a 1.0 ml cryogenic vial with screw cup and stored at -20°C and was assayed the following day. The aliquot was used to measure the tracheal expression of FOXA2, MUC5AC and MUC5B using ELISA. The aliquots were centrifuged again after thawing before the assaying.
Enzyme-linked Immunoassay (ELISA) for FOXA2, MUC5AC AND MUC5B.
The reagents for ELISA were prepared following the standard procedure by Wuhan Fine Biotech Co., Ltd Hamster FOXA2, MUC5AC and MUC5B reagents kit manuals. Thereafter, 100ul of tracheal tissue extract was added to the test sample wells, the plate was then sealed with adhesive strip and incubated for 90 minutes at 37oC. After 90 minutes, the plates were taken out of the incubator, the adhesive strip was removed, and the plated contents were aspirated and discarded. The plate was washed using a multi-channel pipette 2.0 times with 200ul wash buffer. After washing, 100ul of diluted Biotin-labelled antibody (Biotin-labelled antibody dilution 1:100) was added to the bottom of each well without touching the side wall. The plate was covered with a strip of adhesive and put in the incubator at 37oC for 60 minutes. After 60 minutes, the contents of the wells were aspirated and discarded, the wells were washed using a multi-channel pipette for 3.0 times with 200ul wash buffer, and the wash buffer was allowed to stay in the wells for 2.0 minutes each time. After washing, 100ul of diluted HRP-Streptavidin conjugate (HRP-Streptavidin conjugate dilution 1:100) was added to the wells, the plate was covered with adhesive strip and incubated at 37oC for 30 minutes. After 30 minutes, the cover strip was removed, and the wells were washed 5.0 times with 200ul wash buffer while allowing the wash buffer to stay in the wells for 2.0 minutes each time. After washing 90ul of TMB substrate was added to each well, an adhesive cover strip was put on the plate and the plate was incubated for 20 minutes at 37oC without light. To stop the reaction, 50ul of stop solution was added to each well. Optical Density measurements were done at absorbance of 450nm using a microplate reader, Tecan Austria GmbH, 5082 Grödig, Austria Model SUNRISE BASIC TECAN serial number 1001004866. GraphPad Prism software version 10 was used to generate a standard curve and interpolate the unknown concentrations of FOXA2, MUC5B and MUC5AC from absorbance readings.
Results Analysis
The collected results were analyzed using IBM-SPSS version 27 program. Dunnett's Multiple Comparison ANOVA (Dunnett’s t-test) was used to compare differences in FOXA2, MUC5AC, and MUC5B concentrations between experimental hamsters and control hamsters. A p-value less than 0.05 was considered significant for Dunnett’s t-test.
Interpretation of the Results
In this study, the concentrations of tracheal FOXA2, MUC5AC and MUC5B were compared in hamsters treated with Enalapril or Losartan to hamsters treated with water (control). A p-value less than 0.05 was considered significant for Dunnett’s t-test. An increase in mucins secretion would negatively affect the viscosity of respiratory mucus and thereby affect mucociliary transport, leading to increased susceptibility to respiratory infections. Furthermore, a reduction in FOXA2 can lead to abnormal homeostasis of the lung and trachea environments, which would result in worsening of respiratory infections[25 - 26] .
RESULTS
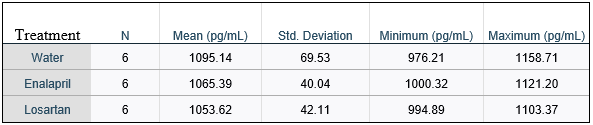
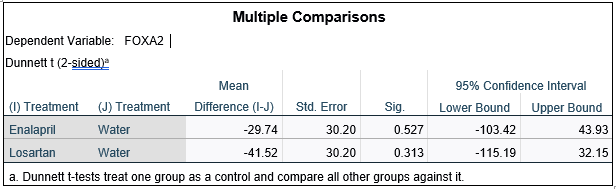
Table 1.0 shows the minimum, maximum and mean concentrations for FOXA2. Table 1.0 shows that the mean concentration of FOXA2 for hamsters treated with water was highest at 1095.14 pg/mL followed by Enalapril at 1065.39 pg/mL and the last hamster treated with Losartan at 1053.62 pg/mL. Figure 1.0 shows the bar graph for mean concentration of FOXA2 in picograms per milliliter (pg/mL) and the error bars show that there were no significant differences in mean concentration between hamsters treated with Enalapril or Losartan and hamsters treated with water (Control) at 95% confidence interval. Table 1.1 shows Dunnett’s t-test of mean concentration for FOXA2. Table 1.1 shows that there were no significant differences (p > 0.05) in the mean FOXA2 concentrations between hamsters treated with enalapril or losartan and distilled water (control).
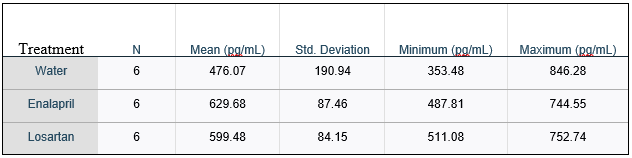
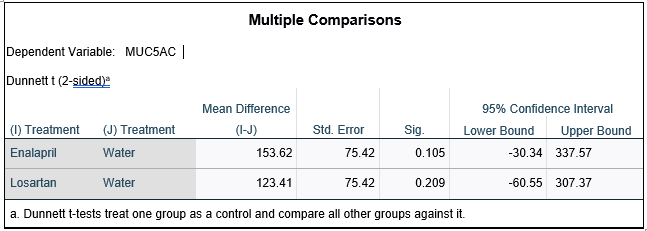
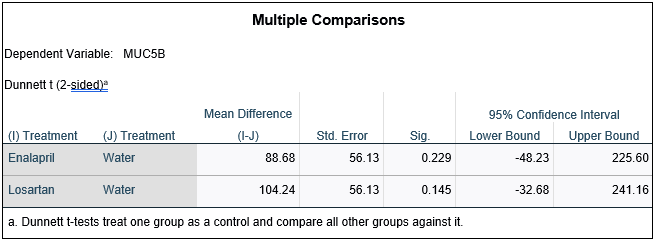
Furthermore, Table 2.0 shows the minimum, maximum, and mean concentration for MUC5AC. Table 2.0 shows that the mean concentration for hamsters treated with Enalapril was the highest 629.68 pg/mL followed by Losartan at 599.48 pg/mL and hamsters treated with water was the last at 476.07 pg/mL. Figure 2.0 shows the bar graph of mean concentration of MUC5AC picograms per milliliter (pg/mL) and the bar graph shows that there was no significant difference in mean concentration between hamsters treated with Enalapril or Losartan and hamsters treated with water (control) at 95% confidence interval. Table 2.1 shows Dunnett’s t-test of mean concentration for MUC5AC. Table 2.1 shows that there were no significant differences (p > 0.05) in the mean concentration of MUC5AC between hamsters treated with enalapril or losartan and hamsters treated with water (control).
Finally, Table 3.0 shows the minimum, maximum, and mean concentration for MUC5B.Table 3.0 shows that Losartan had the highest mean concentration at 619.98 pg/mL followed by Enalapril 604.42 pg/mL and the last water at 515.74 pg/mL. Figure 3.0 shows the bar graph of MUC5B mean concentration in picograms per milliliter (pg/mL). The bar graph shows that there were no significant differences in the mean concentration of MUC5B between hamsters treated with Enalapril or Losartan and hamsters treated with water (control) at 95% confidence interval. Table 3.1 shows Dunnett’s t-test of mean concentration of MUC5B. Table 3.1 shows that there were no significant differences (p > 0.05) in the mean concentration of MUC5B between enalapril or losartan treated hamsters and water treated hamsters (control).




DISCUSSION
This study aimed to investigate the effects of angiotensin receptor blockers (ARBs) and angiotensin converting enzyme inhibitors (ACEIs) on tracheal FOXA2, MUC5B and MUC5AC. FOXA2, MUC5B and MUC5AC are important macromolecules in maintenance of respiratory tract homeostasis and mucociliary clearance[5 - 25] . Impairment of mucociliary clearance can lead to increased susceptibility of the respiratory system to infections. Mucociliary clearance is the primary innate defense mechanism of the respiratory tract[27] . Mucociliary clearance can be impaired if there is an over expression of respiratory mucins specifically, MUC5AC and MUC5B[2 - 28] . Forkhead box protein A2 (FOXA2) is a key transcriptional regulator that maintains airway mucus homeostasis, depletion of FOXA2 leads to respiratory mucus hypersecretion which then leads to worsening of respiratory system infections[25 - 29] .
The results of this study show that enalapril and losartan decreased the concentration of FOXA2 compared to the control (table 1.0), however, the decrease in concentration of FOXA2 was not significant (p > 0.05) compared to the control (table1.1; figure 1.0). Based on these results, enalapril and losartan did not lead to a significant reduction in FOXA2 in the trachea. No literature was found the shows the effect of ARBs and ACEIs on respiratory FOXA2. Since there was significant reduction in FOXA2, taking of enalapril or losartan would not lead to dysregulation of mucus homeostasis in the trachea by depleting FOXA2.
In chronic inflammatory respiratory disorders, MUC5B and MUC5AC increase in the respiratory tract[3] . MUC5B and MUC5AC are the major matrix-forming macromolecules in airway mucus, because of this, viscoelastic properties of airway mucus depend on them[5] . Thick mucus slows mucociliary clearance, affecting the ability of the respiratory track to remove pathogens and other particles. Loss of MUC5B inhibits innate inflammatory responses, resulting in accumulation of alveolar macrophages with impaired ability to phagocytose and clear pathogens[30] . Furthermore, MUC5AC confers resistance to viral infections[31] , however, overexpression of MUC5AC is detrimental in acute lung injury as it may cause mucus plugs and increase bronchial hyperresponsiveness[32 - 33] . MUC5AC-rich mucus markedly impairs mucociliary transport because it is tethered to the epithelial wall[28] . Mucins selectively bind to and disrupt the aggregation of microbial pathogens, preventing pathogens from entering the periciliary layer and blocking their access to the surfaces of the underlying epithelial cell surfaces[34] .
The findings of this study show that Enalapril and Losartan both caused an increase in MUC5AC and MUC5B (table 3.0; table 2.0). However, the increase was not significant (p > 0.05) compared to the control (table 3.1; figure 3.0; table 2.1; figure 2.0). Based on these results, Enalapril, and Losartan increases MUC5AC and MUC5B, but the increase is not significant (p > 0.05) when compared to the control. No other studies were found that show the effects of ARBs and ACEIs on MUC5AC and MUC5B. Further studies are required to study what effect these marginal increases may have on the viscoelasticity properties of respiratory mucus and mucociliary escalator[27] . Enalapril and Losartan did not have a significant effect on the concentration of respiratory FOXA2, MUC5AC and MUC5B of the Hamster tracheal Mucosa. Therefore, taking these drugs would not negatively affect mucociliary clearance of the respiratory system by overexpression of respiratory mucins.
CONCLUSION
The results of this study show that the administration of enalapril or losartan did not have a significant effect on the expression of FOXA2, MUC5AC and MUC5B. The implication is that taking enalapril and Losartan may not lead to impairment of mucociliary clearance or dysregulation of the tracheal homeostasis through over expression of MUC5AC, MUC5B and depletion of FOXA2. In general, the findings of this study suggest that administration of enalapril or losartan does not significantly increase the production of respiratory tract mucins, therefore, the administration of these drugs will not reduce the innate immune response of the respiratory tract through the impairment of mucus production.
Limitation of the Study
Interpretation of the results is based on FOXA2, MUC5AC, and MUC5B, the effects of Enalapril and Losartan were not tested on other mucins. Furthermore, though ACEIs and ARBs have similar mechanisms of action, the interpretation of results may be limited to Enalapril and Losartan.
What is already known on this topic?
• Role of ACEI and ARBs on ACE2 expression in the upper respiratory system.
• effects of ARBs and ACEIs in respiratory angioedema and cough.
What this study adds
• Adds information of the effect of ARBs or ACEIs on respiratory mucins MUC5AC, MUC5B and FOXA2.
• Taking enalapril or losartan may not increase susceptibility of patients to respiratory infections due to increased production of mucus and dysregulation of respiratory mucus homeostasis.
DECLARATIONS
Copyright Notice: The authors being the sole and legitimate holder of the copyright hereby transfer it to Medical Journal of Zambia.
Availability of data: Data is available upon request from the corresponding author.
Competing interests: The authors declare no competing interest.
Funding: The authors did not receive any specific funding for this study.
Authors' Contrbutions
Conceptualization: L. Mubbunu, H. Simukoko.
Methodology: L. Mubbunu, H. Simukoko; E. Mwaanga, B. Hang’ombe.
Data collection: L. Mubbunu, H Simukoko, B. Hang’ombe, S. Siziya and E. Mwaanga.
Analysis and drafting of manuscript: L. Mubbunu, H. Simukoko, B. Hang’ombe, S. Siziya and E. Mwaanga.
Review and editing: L. Mubbunu, H. Simukoko, B. Hang’ombe, S. Siziya and E. Mwaanga; Supervision: H. Simukoko.
Manuscript submission: L. Mubbunu, E. Mwaanga, B. Hang’ombe, S. Siziya and H. Simukoko; have read and agreed to the published version of the manuscript.
REFERENCES
- 1. Button B, Cai LH, Ehre C, et al. A periciliary brush promotes the lung health by separating the mucus layer from airway epithelia. Science. 2012;337(6097):937-941. doi:10.1126/science.1223012.
- Singanayagam A, Footitt J, Marczynski M, et al. Airway mucins promote immunopathology in virus-exacerbated chronic obstructive pulmonary disease. J Clin Invest. 2022;132(8):e120901. doi:10.1172/JCI120901.
- Silva MA, Bercik P. Macrophages are related to goblet cell hyperplasia and induce MUC5B but not MUC5AC in human bronchus epithelial cells. Lab Invest. 2012;92(6):937-948. doi:10.1038/labinvest.2012.15.
- Lachowicz-Scroggins ME, Yuan S, Kerr SC, et al. Abnormalities in MUC5AC and MUC5B Protein in Airway Mucus in Asthma. Am J Respir Crit Care Med. 2016;194(10):1296-1299. doi:10.1164/rccm.201603-0526LE.
- Bonser LR, & Erle DJ. Airway Mucus and Asthma: The Role of MUC5AC and MUC5B. J Clin Med. 2017;6(12):112. Published 2017 Nov 29. doi:10.3390/jcm6120112.
- Richardson S, Hirsch JS, Narasimhan M, et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area [published correction appears in JAMA. 2020 May 26;323(20):2098]. JAMA. 2020;323(20):2052-2059. doi:10.1001/jama.2020.6775.
- Messerli FH, Bangalore S, Bavishi C, Rimoldi SF. Angiotensin-Converting Enzyme Inhibitors in Hypertension: To Use or Not to Use? J Am Coll Cardiol. 2018;71(13):1474-1482. doi: 10.1016/j.jacc.2018.01.058.
- South AM, Tomlinson L, Edmonston D, Hiremath S, Sparks MA. Controversies of renin-angiotensin system inhibition during the COVID-19 pandemic. Nat Rev Nephrol. 2020;16(6):305-307. doi:10.1038/s41581-020-0279-4.
- Byrd JB, Adam A, Brown NJ. Angiotensin-converting enzyme inhibitor-associated angioedema. Immunol Allergy Clin North Am. 2006;26(4):725-737. doi: 10.1016/j.iac.2006.08.001.
- Karamyan VT. Between two storms, vasoactive peptides or bradykinin underlie severity of COVID-19?. Physiol Rep. 2021;9(5):e14796. doi:10.14814/phy2.14796.
- Rex DAB, Vaid N, Deepak K, Dagamajalu S, Prasad TSK. A comprehensive review on current understanding of bradykinin in COVID-19 and inflammatory diseases. Mol Biol Rep. 2022;49(10):9915-9927. doi:10.1007/s11033-022-07539-2.
- Ellis KM, Fozard JR. Species differences in bradykinin receptor-mediated responses of the airways. Auton Autacoid Pharmacol. 2002;22(1):3-16. doi:10.1046/j.1474-8673.2002. 00230.x.
- Barnes PJ. Effect of bradykinin on airway function. Agents Actions Suppl. 1992;38 (Pt 3):432-438.
- Choi W, Choe S, Lau GW. Inactivation of FOXA2 by Respiratory Bacterial Pathogens and Dysregulation of Pulmonary Mucus Homeostasis. Front Immunol. 2020; 11:515. Published 2020 Mar 25. doi:10.3389/fimmu.2020.00515.
- Widdicombe JH. Regulation of the depth and composition of airway surface liquid. J Anat. 2002;201(4):313-318. doi:10.1046/j.1469-7580.2002. 00098.x.
- Arifin WN, Zahiruddin WM. Sample Size Calculation in Animal Studies Using Resource Equation Approach. Malays J Med Sci. 2017;24(5):101-105. doi:10.21315/mjms2017.24.5.11.
- Cleary JD, Taylor JW. Enalapril: a new angiotensin converting enzyme inhibitor. Drug Intell Clin Pharm. 1986;20(3):177-186. doi:10.1177/106002808602000301.
- Pai MP. Drug dosing based on weight and body surface area: mathematical assumptions and limitations in obese adults. Pharmacotherapy. 2012;32(9):856-868. doi:10.1002/j.1875-9114.2012. 01108.x.
- National Research Council (US) Subcommittee on Laboratory Animal Nutrition. Nutrient Requirements of Laboratory Animals: Fourth Revised Edition, 1995. Washington (DC): National Academies Press (US); 1995.
- Emily LM, & Hankenson FC. Chapter 5 - Biology and Diseases of Hamsters, Editor(s): James G. Fox, Lynn C. Anderson, Glen M. Otto, Kathleen R. Pritchett-Corning, Mark T. Whary, In American College of Laboratory Animal Medicine, Laboratory Animal Medicine (Third Edition), Academic Press, 2015, Pages 209-245, ISBN 9780124095274, https://doi.org/10.1016/B978-0-12-409527-4.00005-5.
- Sica DA, Gehr TW, Ghosh S. Clinical pharmacokinetics of losartan. Clin Pharmacokinet. 2005;44(8):797-814. doi:10.2165/00003088-200544080-00003
- Rabi DM, Khan N, Vallee M, Hladunewich MA, Tobe SW, Pilote L. Reporting on sex-based analysis in clinical trials of angiotensin-converting enzyme inhibitor and angiotensin receptor blocker efficacy. Can J Cardiol. 2008;24(6):491-496. doi:10.1016/s0828-282x(08)70624-x.
- Parkinson CM, O'Brien A, Albers TM, Simon MA, Clifford CB, Pritchett-Corning KR. Diagnostic necropsy and selected tissue and sample collection in rats and mice. J Vis Exp. 2011;(54):2966. Published 2011 Aug 7. doi:10.3791/2966.
- Payton AJ, Forsythe DB, Dixon D, Myers PH, Clark JA, Snipe JR. Evaluation of ketamine-xylazine in Syrian hamsters. Cornell Vet. 1993;83(2):153-161.
- Choi W, Yang AX, Waltenburg MA, et al. FOXA2 depletion leads to mucus hypersecretion in canine airways with respiratory diseases. Cell Microbiol. 2019;21(1):e12957. doi:10.1111/cmi.12957.
- Choi W, Choe S, Lau GW. Inactivation of FOXA2 by Respiratory Bacterial Pathogens and Dysregulation of Pulmonary Mucus Homeostasis. Front Immunol. 2020; 11:515. Published 2020 Mar 25. doi:10.3389/fimmu.2020.00515.
- Bustamante-Marin XM, Ostrowski LE. Cilia and Mucociliary Clearance. Cold Spring Harb Perspect Biol. 2017;9(4):a028241. Published 2017 Apr 3. doi:10.1101/cshperspect. a028241.
- Bonser LR, Zlock L, Finkbeiner W, Erle DJ. Epithelial tethering of MUC5AC-rich mucus impairs mucociliary transport in asthma. J Clin Invest. 2016;126(6):2367-2371. doi:10.1172/JCI84910.
- Wan H, Kaestner KH, Ang SL, et al. Foxa2 regulates alveolarization and goblet cell hyperplasia. Development. 2004;131(4):953-964. doi:10.1242/dev.00966.
- Huang X, Guan W, Xiang B, Wang W, Xie Y, Zheng J. MUC5B regulates goblet cell differentiation and reduces inflammation in a murine COPD model. Respir Res. 2022;23(1):11. Published 2022 Jan 18. doi:10.1186/s12931-021-01920-8.
- Ehre C, Worthington EN, Liesman RM, et al. Overexpressing mouse model demonstrates the protective role of Muc5ac in the lungs [published correction appears in Proc Natl Acad Sci U S A. 2014 Apr 15;111(15):5753]. Proc Natl Acad Sci U S A. 2012;109(41):16528-16533. doi:10.1073/pnas.1206552109.
- Koeppen M, McNamee EN, Brodsky KS, et al. Detrimental role of the airway mucin Muc5ac during ventilator-induced lung injury. Mucosal Immunol. 2013;6(4):762-775. doi:10.1038/mi.2012.114.
- Evans CM, Raclawska DS, Ttofali F, et al. The polymeric mucin Muc5ac is required for allergic airway hyperreactivity. Nat Commun. 2015; 6:6281. Published 2015 Feb 17. doi:10.1038/ncomms7281.
- Whitsett JA, Alenghat T. Respiratory epithelial cells orchestrate pulmonary innate immunity. Nat Immunol. 2015;16(1):27-35. doi:10.1038/ni.3045.
Medical Journal of Zambia, Vol 50, 1
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.