Madura Foot in an African Adult Male in Zambia: A likely Case of Misdiagnosis
Malumani Malan
Mulungushi University, School of Medicine and Health Sciences. Honorary consultant Dermatologist, Department of Internal Medicine, Dermatology and Venereology Unit, Livingstone University Teaching Hospital .
Miyoba H. Michelo
Mulungushi University, School of Medicine and Health Sciences. / Honorary Consultant Surgeon-Department of Surgery, Livingstone University Teaching Hospital.
Kyakilika Kebby
Department of Surgery, Livingstone University Teaching Hospital, Livingstone.
DOI: https://doi.org/10.55320/mjz.50.2.384
Keywords:Madura foot, Mycetoma, eumycetoma, actinomycetoma, saprotrophs
ABSTRACT
Background: Mycetoma also synonymous referred to as Madura's foot is a chronic granulomatous cutaneous infection caused by some genera of fungi and bacteria, leading to progressive and proliferative destruction of soft tissue and the nearby anatomical structures if no intervention is offered on time.
Case presentation: We report a case of actinomycetoma in an African adult man residing in a rural-urban setup. After histological confirmation, the client was conservatively managed with oral medication: 1) dapsone 100mg once a day and trimethoprim/sulfamethoxazole(septrin) 160mg/800mg three times daily for one year with an excellent outcome.
Conclusions: The gist of this rare case is to exemplify the role of integrated management of patients without underplaying the role of good clinical practice. Also, a call and advocate for improved health care services in the sub-Saharan countries. This will prevent or reduce avoidable medical complications caused by neglected and treatable diseases like actinomycocetoma.
INTRODUCTION
Mycetoma is a chronic slowly progressive subcutaneous granulomatous infection. Mycetoma also synonymous referred to as Madura foot is a chronic granulomatous cutaneous infection caused by some genera of fungi and bacteria, leading to progressive and proliferative destruction of soft tissue and the nearby anatomical structures if no intervention is offered on time.[1-2] It has been characterized clinically by triad of granulomatous swelling, multiple sinus track formation, and discharge of granules.[3-4] According to Develoux et al., the commonest site is the foot which accounted for about 70% of all cases, leg, knee, thigh, hands and arm are the other most frequent extrapodal regions affected.[5]
Mycetoma are classified as either eumycetoma, caused by fungal species and actinomycetoma which is caused by bacteria. However, these organisms give a similar clinical presentation. Afroz et al., denotes that eumycetoma mostly present as a small localized tumor like mass, with or without sinuses, or may mostly be associated with significant morbidity in terms of gradual enlargement, deformity and destruction of the affected site if no intervention is offered.[2] The diagnosis of eumycetoma can be made tentatively clinically when discharging grains are visible to the naked eye but if in limbo, a fine needle aspiration or biopsy for histopathology can be obtained.[6] It is important to distinguish these two causative organisms as the management of these patients varies significantly. We report a case of actinomycetoma in an African adult man residing in a rural-urban setup.
CASE PRESENTATION
A 31 years old African man, a teacher by profession visited his local healthcare centre in the rural part of Zambia with complaints of progressive swelling under the right foot, which with time had progressive many holes discharging pus like fluid for several days. The lesion was worse when he wore closed shoes. Prior to the swelling, he gives a history of progressive pain under the right foot of over one year duration.
The pain was gradually increasing in intensity with time and it was worse during the night. He denies any pin and needle sensation or any abnormal sensation on the skin. He denied any history of trauma and was unsure of any piecing by any inanimate object prior to commencement of pain. Oral analgesics like paracetamol and brufen in the initial stages would give him some relief. There was associated gradual swelling over a 7 months period. Two months later, due to the pressure exertion on the foot while going about his daily chores, the lesion bulged and had made a protrusion on the right lateral border of foot. At this point he then went to a higher health center for medical checkup where a partial excision of the lesion was made.
Review of other system, past medical and surgical history were unremarkable. He was immunocompetent.
CLINICAL FINDINGS
Examination of the foot reviewed a granulomatous lesion on the lateral border with well-defined borders, some slough and multiple draining sinuses and an obvious club like foot deformity. The overlying skin was hyper-pigmented and tender to touch. On the plantar aspect on the foot, the sore had several cornified plug punctate-like opening coalesced in the mid-section of foot with hyperpigmentation and scaling of the surrounding glabrous skin as in Figure 1.

The rest of the examination was unremarkable.
DIAGNOSTIC ASSESSMENT
A tentative diagnosis of suspected soft tissue malignancy was entertained and patient was advised for a below knee amputation after review of biopsy results. Other laboratory investigations were unremarkable.
Histological report reviewed multiple filamentous colonies surrounded by an eosinophilic inflammatory reaction. Suppurative inflammation was noted around the colonies in the background; lymphocytes, plasma cells and histocytes also. There was no evidence of malignancy. The histological features were in keeping with actinomycocetoma.
After assessment of clinical and investigations done, the client was treated as a case of actinomycetoma- madura foot on the right foot.
THERAPEUTIC INTERVENTION, FOLLOW-UP AND OUTCOMES
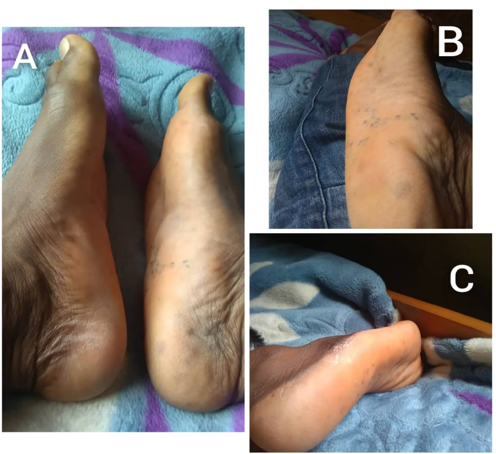
A dermatological consultations was made and recommendation on conservative management of patient on oral medication: 1) dapsone 100mg once a day and trimethoprim/sulfamethoxazole(septrin) 160mg/800mg three times daily for one year to be reviewed monthly for three months the three monthly. The progress of wound /lesion healing is as noted in figure 2 (A)After one week of treatment with aggressive wound cleaning daily. (B)Defect after one month and (C) after 2 months. The outcome of the treatment was positive as shown in figure 3: this is after one year of treatment .
PATIENTS PERSPECTIVE
Our client thought the condition he had was inflicted on him by a witch or wizard due to its insidious onset with an unexplained progression to the point where amputation of the limb was offered in fear of this lesion being cancerous.

DISCUSSION AND CONCLUSION
This article comes at a time when there is a cry for improved healthcare services in the country is paramount. In health centers where they are unable to thoroughly investigate, the opt for draconian and aggressive treatment options. For instance, our client was offered a below knee amputation but declined the offer in search of other treatment options. Other authors have noted that amputation is commonest complication of madura foot either due to late presentation, lack of adequate investigations or over assumption that the hideous lesion is malignant.[7-8] The need for early diagnosis can never be over emphasized coupled with functioning support healthcare departments like the laboratory- histopathological services, radiological and other essential services. It is because of lack of specialist clinician and fully fledged support units in most of the health centers in the country that diagnosis of such ailments delays.
Due to an increase in the number of specialized specialists and fairly improved healthcare services in the urban-rural areas of Zambia, the number of accurate diagnosis have been made and has reduced on referrals to the tertiary hospitals and reduced costs and complications on the side of patients during the management of their ailments.
As much as the diagnosis of madura foot can be made clinically by the following the disease characteristic triad of subcutaneous mass, multiple sinuses and discharge containing grains, its treatment is based on the causative organism; thus, histopathological diagnosis is paramount.
The gist of this case is to exemplify the role of integrated management of patients without underplaying the role of good clinical practice. This will prevent or reduce avoidable medical complications caused by neglected and treatable diseases like actinomycocetoma.
ACKNOWLEDGEMENTS
We sincerely wish to thank the patient for granting us permission to his pictures in this case report.
CONFLICT OF INTEREST
The authors have no conflict of interest to declare.
Ethical Approval: Not applicable
Informed consent: Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the editor of this journal
Financial Funding: Non to declare.
Data availability: Not applicable
Author’s contributions: KK, MHM and MM were involved in the management of the patient and fully participated in the write-up of this case review. MM gave the overall supervision of the write-up.
REFERENCES
- Arenas R, Martinez RFF, Torres-Guerrero E, Garcia C. Actinomycetoma: An Update on Diagnosis and Treatment. :5.
- Afroz N, Khan N, Siddiqui FA, Rizvi M. Eumycetoma versus actinomycetoma: Diagnosis on cytology. J Cytol [Internet]. 2010 Oct [cited 2020 Apr 15];27(4):133–5. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3001200/
- Relhan V, Mahajan K, Agarwal P, Garg VK. Mycetoma: An update. Indian Journal of Dermatology [Internet]. 2017 Jul 1 [cited 2019 Dec 24];62(4):332. Available from: http://www.e-ijd.org/article.asp?issn=0019-5154;year=2017;volume=62;issue=4;spage=332;epage=340;aulast=Relhan;type=0
- Katkar VJ, Tankhiwale SS, Kurhade A. FUSARIUM SOLONI MYCETOMA. Indian J Dermatol [Internet]. 2011 [cited 2020 Apr 15];56(3):315–7. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3132913/
- Develoux M, Dieng MT, Kane A, Ndiaye B. Management of mycetoma in West-Africa. Bull Soc Pathol Exot. 2003 Jan;96(5):376–82.
- Fernandes H, D’souza CRS, Shekar JC, Marla NJ, Swethadri GK, Naik R. Cytodiagnosis of actinomycetoma. Diagn Cytopathol. 2009 Jul;37(7):506–8.
- Venkatswami S, Sankarasubramanian A, Subramanyam S. The madura foot: looking deep. Int J Low Extrem Wounds. 2012 Mar;11(1):31–42.
- Abbas M, Scolding PS, Yosif AA, El Rahman RF, El-Amin MO, Elbashir MK, et al. The disabling consequences of Mycetoma. PLoS Negl Trop Dis. 2018 Dec;12(12):e0007019.
Medical Journal of Zambia, Vol 50, 2
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.