Challenges faced by patients with Osteoarthritis of the Hip and Knee in using their Bathrooms in Lusaka, Zambia
Billiat Chongo
Lusaka Apex Medical University, Lusaka, Zambia
Chese Ngulube
Physiotherapist, Zambia
Marjorie Mwansa
St John Paul II Italian Orthopaedic Mission Hospital, Lusaka, Zambia
Dominic Sashi
Ministry of Health, Zambia
Fair Banji Mwiinga
Lusaka Apex Medical University, Lusaka, Zambia
DOI: https://doi.org/10.55320/mjz.50.1.383
Keywords:Osteoarthritis, Using Bathrooms, Challenges, International classification of disease health and functioning, Toileting
ABSTRACT
Background: People with Osteoarthritis (OA) of the hip and knee have difficulties in performing basic activities of daily living. These problems arise from disturbed biomechanics, pain and loss of range of motion. Both pain and stiffness prevent deep knee flexion, a movement that is important in the use of both the toilet and the bathing facilities. The aim of this study was to determine the challenges faced by patients with osteoarthritis of the hip and knee in using their bathrooms in Lusaka, Zambia.
Methods: A cross sectional, descriptive quantitative study was done. The study was conducted at the University Teaching Hospital in the Department of Physiotherapy. Fifty six participants with hip or knee osteoarthritis were recruited in the study. Portions of the ICF were used to determine the level of difficulty in using both the bathtub for bathing and the toilet. A visual analogue scale and manual goniometer were used to measure the intensity of pain and range of motion respectively. Data were analysed using SPSS version 25.0. Chi Square test was used to determine if there was a relationship between severity of pain and the ranges of motion in the hip and knee at the significance level of 0.05.
Results: Participants in this study had a mean age of 53.39 years (SD=9.210). Majority were females (79%) and 21% males. The participants had mild problems with (52%, n=29) followed by moderate problems with bathing (32%, n=18). More than half of the participants had moderate problems (55% while a few (7%) had severe problems with toileting. During bathing and toileting, 80% and 62% of the participants experienced moderate to severe pain in the knee and hip respectively. There were significant associations between the severity of pain and the ranges of motion in hip flexion, hip extension and knee flexion (P = 0.01, 0.001 and 0.02).
Conclusion: Patients with OA of the knee and the hip have moderate to severe challenges with bathing and toileting. Pain may be the main factor contributing to the challenges in bathing and toileting. Physiotherapy needs to take the bathing and toileting facilities into account when managing patients with OA of the knee and hip.
INTRODUCTION
Osteoarthritis is the most common form of arthritis. The knee joint is most frequently affected followed by osteoarthritis (OA) of the hip and then other joints such as the small joints of the hands[1] . The prevalence of OA increases dramatically after the age of 50 years in men and 40 years in women[2] . Estimates of symptomatic osteoarthritis are 9.6% of men and 18.0% of women over the age of 60 years globally, although precise estimates of the prevalence of OA remain elusive[2] . Kaur and colleagues[3] stated that the prevalence of OA is unknown, due to the uncertainties and variations in diagnostic mechanisms. Usenbo and others[4] reported that osteoarthritis was the most prevalent form of arthritis in urban settings of South Africa (55.1%) but ranged from 29.5 – 82.7% among adults aged over 65 years in rural settings. The commonest form of osteoarthritis among Africans affects the knee and hip[5] and causes the greatest burden on functional ability seemingly because of joint pain and stiffness [6] .
Some of the personal factors associated with onset of knee pain are being overweight, female gender and previous knee injury[7] , joint instability, misalignment of joints, obesity[8-9] . The prevalence of OA increases dramatically after the age of 50 years in men and 40 years in women[2] . In the progression of OA, conditions affecting other parts of the body such as obesity, and trauma can immensely contribute to the degradation of joint systems in those with OA[10-11] .
Pain is the factor that drives individuals to seek medical attention; hinders the maintenance of physical activity; and plays a key role in onset of frailty in the elderly[3] . Pain from OA has been described as a dull aching pain that, over time, becomes more constant though of short episodes of more intense pain[12] . Two types of pain occur in OA; one is intermittent but severe, and the other constant and background or aching, which can be nociceptive, neuropathic or both. According to Miller and co-investigators[13] , tissue injury products such as prostaglandins and bradykinins, as well as cytokines and chemokines excite pain-sensing neurons (nociceptors)[14] . Moreover, excessive or abnormal joint loading stimulates joint tissue cells to produce pro-inflammatory factors and proteases that mediate joint tissue destruction and leads to swelling, decreased shock absorbing properties, softening, fracturing, ulceration and ultimately erosion of the cartilage with exposure of the sub-chondral bone[12-15] .
Knee osteoarthritis contributes more to the dysfunctions than other forms of arthritis because it restricts the mobility of the individual as a whole[2] . Persons with arthritis have demonstrated marked pain-related functional impairment characterized by difficulty with many aspects of daily activity[16] . Disabilities in OA are manifested as pain and stiffness, difficulty in walking, difficulties in independently carrying out activities of daily living such as bathing and toileting, and reduced social interaction[17] . In fact, about 11% of adults with knee OA need help with their personal care[18] . This study set out to determine the level of difficult faced by patients with OA of the hip and knee in using their bathing and toileting facilities.
METHODS
Study design:
A quantitative descriptive cross sectional study was carried out.
Study site:
The study was conducted in the department of physiotherapy at the Adult University Teaching Hospital, Lusaka Zambia.
Study population and sample size:
The population was 97 patients with OA of the hip or knee who sought physiotherapy during the study period. The patients had been referred for physiotherapy services by Orthopedic Surgeons. Only patients with radiologically confirmed osteoarthritis were included in the study. Patient OA of the knee or hip who had low back pain, radiculopathy or lower limb neuropathies were excluded from the study. Patients who were using other facilities to bath without having to enter a bathtub were also excluded.
Simple random sampling using a rotary technique was used to select the study participants. Seventy eight (78) participants were selected for the study.
Data collection:
A questionnaire adapted from the ICF on activities of daily living was used to determine the level of difficulty in using both the bathtub and the toilet. Portions of the d domain (self-care and mobility) were included in the questionnaire. The specific areas picked from the d-domain of the ICF were:
i. Mobility (d4) d450-walking and moving, d4600 walking in the home, d410 changing body posture, d420 transferring while standing, d4153a maintaining sitting posture and d4154b maintaining standing posture.
ii. Self-care (d5) d530 for toileting and d510 for washing one self
Bathing was divided into five tasks (moving to bathroom, getting into the bathtub, positioning in the bathtub, rising to standing while in the bathtub, getting out of the bath tub). This gave a possible total of 20. For toileting, the activity was divided into four (4) tasks (getting to the toilet, lowering to sit/squat, sitting/squatting on the toilet pan and rising from sitting/squatting position). A visual analogue scale was used to determine the intensity of pain. A manual goniometer was used to measure the ranges of motion for the hips and knees.
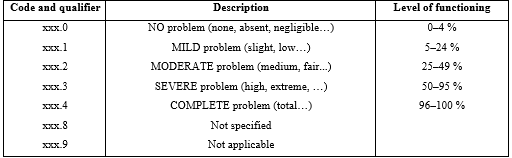
Data were collected as the participants attended their usual physiotherapy sessions. Each participant gave a written informed consent. Personal characteristics were collected first then each participant scored the level of challenges they faced with both bathing and toileting as activities and as divided into tasks (which were recorded as problems or difficult on the questionnaire) based on the ICF as no problems (0), mild problems (1), moderate problems (2), and severe problems (3) or completely unable to (4). This gave a possible total of 20 for bathing using a bathtub and 16 for toileting. To collect data on the severity of pain during bathing and toileting, a visual analogue scale was used; the score was determined by measuring the distance in centimeters on the line between the no pain anchor and the patient’s mark, which provided a range of scores from 0-10. The scores were described as no pain (0cm) mild pain (1-3cm), moderate pain (4-6cm) and severe pain 7-10cm).
A manual goniometer was used to measure ranges of motion (ROM) in the hip and knee joints, during which process participants were dressed in underwear to expose the hip and knee, in the privacy of a cubicle. Range of motion (ROM) in the knee was measured with the participant in the prone position and the knee joint line on the lateral aspect of the knee was used as the fulcrum for flexion. The movable arm of the goniometer followed the long axis of the fibular in line with the lateral malleolus and the fixed arm followed the long axis of the femur in line with the greater trochanter. To measure ROM for hip extension the participant maintained the prone position and the greater trochanter was taken as the fulcrum. To measure ROM for hip flexion, abduction and adduction, the participants assumed the supine position. For hip flexion, the fulcrum was the greater trochanter with the knee flexed on the ipsilateral limb. For abduction and adduction, the anterior superior iliac spine was the fulcrum and the opposite anterior superior iliac spine as the reference point for the stationary arm of the goniometer. For internal and external rotation the participants assumed the high sitting position. The center of the patella was taken as the fulcrum and hanging (vertical) position of the leg as the neutral position. Both internal and external hip rotations were measured from the zero point. Each movement was measured actively and repeated thrice. The best of the movements was recorded for each direction of movement.
Data management and analysis:
Submitted questionnaires were checked for completeness and stored securely in a box file to which only the researcher had access. The questionnaires were then sorted, coded, and data entered in the statistical Package for Social Sciences (SPSS). Using the SPSS program, descriptive and inferential statistical analyses were performed. Descriptive statistics measures of central tendency included mean and mode, while the measures of dispersion included the range and standard deviation. Inferential statistics were performed to test the statistical significance of association between variables using the student’s test, Chi-Square test and linear regression. Inference was done at 95% confidence and significance at 0.05. Age and gender were analyzed as ratios and presented in tables. Data on pain severity were analyzed as means and described as no pain, mild pain, moderate pain and severe pain, and presented in tables. To determine whether there was a significant difference in mean ages of males and females, the independent t-test was used. ROM in the knee and hip were analyzed as mean ROM for individual movements in each joint in males and females. The Chi-square test was used to find out whether there were significant differences in joint motions between males and females. To find out if there was a relationship between severity of pain and ROM, linear regression analysis was performed.
Types of bathing and toileting facilities were analyzed as percentages and frequencies. Bathing facilities were divided into Bathtub (with or without other utensils) and toileting facilities, which were divided into sitting, and squatting toilets. The level of difficulty in bathing and toileting were determined and described according to the ICF and presented in graphs. To determine the level of difficulty in using bathing facilities, data were analyzed separately; bathing activities were divided into tasks and each task was scored from 0-4. The total for all tasks for bathing was found by adding all scores out of a possible 20. This was translated to percentage and described as the overall difficult in bathing and described based on the ICF. The levels of difficulty for all participants were then presented as frequencies. To determine the level of difficulty in using toilet facilities, data were analyzed separately; toilet activities were divided into four tasks and each task was scored from 0-4. The total for all tasks in toileting was found by adding all scores out of a possible 16. This was translated to percentage and described based on the ICF scale.
Chi Square test was used to assess whether the severity of pain was significantly related to ROM in the hip and knee joint at the significance level of 0.05.
Ethics approval
Ethics approval was granted by the Lusaka Apex Medical University Biomedical Research Ethics Committee (FWA 00029892, IRB 00001131, Ref: 00124-22). Institutional permission was granted by management at the Adult University Teaching Hospital.
RESULTS
Fifty-six patients participated in this study, giving a response rate of 100%. Of the 56 participants, 76.6% (n = 44) were female and 21.4% (n = 12) were male. The majority of the participants were aged between 40 – 46 years (32.1%). The mean age of the participants was 53.39 years with a standard deviation (SD) of 9.210. There was no significant age difference between males and females (p = 0.211). Forty-two percent of the participants (n = 24) had knee OA followed by 37.5%, (n = 21) with both knee and hip OA and 19.6%, (n = 11) had hip OA. Most of the participants used bathtubs and shower while standing in the tub, others (33.9%, n = 19) used a dish in the tub and the rest (26.8%, n= 15) used a tub only. For toileting, the majority (78.6%, n = 44) used a modern toilet with a sitting toilet pan. The rest (21.4%) used a pit latrine or low squatting toilet pan for toileting.
During bathing, majority of the participants (52%) had mild problems with bathing, and 16% had no problems. No participants had severe problems and none failed completely. In toileting two percent had no problems, 36% had mild problems, 55% had moderate problems and seven percent had severe problems. None of the participants was completely unable to use the toilet. Two tasks in bathing were more problematic. Majority of the participants (39%) had moderate problems in positioning themselves in the bathtub and 37% had moderate problems with rising from a lower position while in the bath tub (long sitting, squatting, and kneeling). More than half of the participants (51.8%) had no problems with getting into and out of the bathtub.
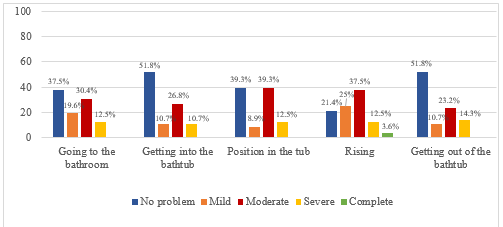
Most of the participants had moderate difficulties in all the five tasks of bathing (30.4%, 26.8%, 39.3%, 37.5%, and 23.2%, respectively).
Level of difficulty in tasks required in toileting
Most of the participants, (42.9%, n=24) had moderate problems in lowering themselves to sit and 33.9% (n=19) had moderate problems in rising from the sitting/squatting position while 28.3% (n=16) had moderate problems to sit or squat (Figure 3).
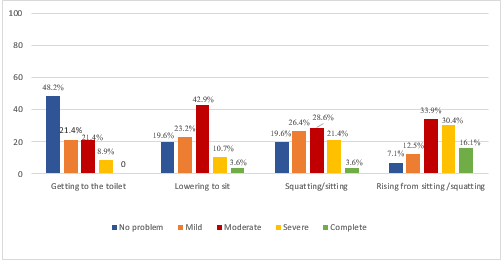
Most of the participants had moderate difficulties in all the four tasks of toileting (21.4%, 42.9%, 28.6%, and 33.9% respectively).
Severity of pain during activities and ranges of motion
Most of participants had severe pain in both the knee and the hip (n = 24 and n = 21 for knee and hip respectively). Females experienced significantly severe pain compared to males in the hip (P = 0.0001) but no significant difference between females and males in knee pain (P = 0.383). Male and female participants had similar ROM except for the hip abduction where males had significantly more ROM than females (P = 0.012).
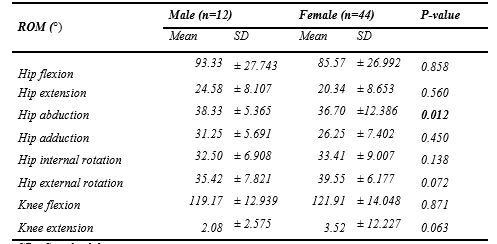
There were significant associations between the severity of pain in the hip and range of motion in hip flexion, hip extension, hip abduction and internal rotation (P = 0.01, 0.001, 0.0001 and 0.009 respectively). There was no significant relationship between severity of pain and range of motion in knee extension (Table 1).
DISCUSSION
Challenges in bathing and toileting
Patients with OA of the hip and knee experienced more problems with toileting than bathing. More than half of the participants (55%) experienced moderate problems in toileting compared to 36% in bathing. None of the participants had severe difficult with bathing while seven percent had severe difficult with toileting. Fifty two percent had mild problems in bathing but 55% had moderate difficulties with toileting. For example 16% of the participants had no problems with bathing compared to all participants with some degree of problem in toileting. Problems with bathing and toileting were reported in Lespasio and colleagues[19] study where patients with OA experienced difficulties in carrying out activities of daily living (ADLs) such as bathing and toileting. Moss[21] had looked generally at ADLs and observed that OA led to difficulties in ADLs. Meanwhile Cerit[20] found that among OA patients who experienced intense problems on their knees, 63.1% struggled to perform activities that required hip and knee movement. Activities that require sit to stand or vice versa have been reported to be difficult among people with OA[21] . In toileting (defecation), a person always requires sitting or squatting and then stand up while in bathing a person may flex and extend the hip and knee to sit and stand several times during the activity to wash different parts of the body. In this study 80% of the people with OA of the knee and hip had moderate to complete failure to rise from the sitting position in toileting which may be attributed to restricted hip and knee mobility in OA[2] . Hunter and Johnson[20] noted that more than 50% of OA patients had moderate to severe difficulty in ADLs. This study found that 16% could not rise from the toileting position and four percent could not rise to standing on their own in the bathtub. Getting to, in and out of the bathtub were relatively easy because more than 50% had no problems with these two tasks probably because these tasks do not need flexing the knee and hip to or beyond the right angle[22] .
Severity of pain and range of motion
In this study, pain in the hip/knee and reduced range of motion could have led to difficulties in bathing and toileting among patients with OA. During either bathing or toileting 28% had moderate to severe pain in the osteoarthritic knees. Comparisons between the normal averages of ROM in the knee and hip[22] to the findings in this study showed reductions especially in the movements that are required in bathing using a bath tub and toileting. Hip flexion was on average 31° less in the affected hip and 20° less in the knee compared to the known normal ROM. At the same time it was found that there were significant associations between the range of motion and severity of pain for the movements that are critical in both bathing in the bathtub and toileting (hip flexion P= 0.01, hip extension P= 0.001, hip abduction p= 0.001 and knee flexion p=0.02). This could explain why people with OA in the hip and knee have difficulties in toileting and bathing because these activities require deep flexion. Squatting and sitting become difficult in knee OA mainly because of pain and stiffness[21] . Whether pain led to reduced range of motion or forcing the joints to move during bathing or toileting led to pain, was not established in this study. An analysis of movements of the tasks in bathing using a bathtub and toileting however could help to justify the difficulties observed in this study. In toileting for example, one has to sit or squat depending on the toilet type. This position requires one to eccentrically use the lower limb muscles and reach a position where the angles at the knee and hip should be above 90° of flexion in a closed kinematic chain movement and on loaded joints. In the presence of pain at either the hip or knee joint, patients usually experience difficulties in independently bathing or toileting[23] . Pain from arthritis has been termed as one of the key barriers to maintaining physical activity[13] . In OA, tissue injury products such as prostaglandins and bradykinins as well as cytokines and chemokines excite pain-sensing neurons. The pathophysiological mechanisms in OA involve the pro-inflammatory interleukins IL-1β, IL-6, IL-8, tumour necrosis factor α (TNF-α) and several pro-catabolic mediators[15] . This may be among the reasons for the presence and severity of pain found in this study. This pain most likely occurred due to the exposed nociceptors or the rubbing of raw surfaces during joint motion in a movement that takes place in a loaded joint[35] . Pain could also have come from stretching the ligaments, capsule and synovium which are usually inflamed and thickened in OA. According to Leopold[14] pain is a dominant symptom in OA, which becomes more persistent and more limiting as OA progresses In fact, it has been demonstrated that knee OA patients with longer symptom duration have a neuropathic pain component in their knee[26] . It has also been noted that patients with neuropathic pain have more severe pain and disability than patients without a neuropathic component[27] . Although the nature of the pain was not established in this study, pain itself could have been a direct limiting factor in using bathing and toileting facilities. At the same time the toileting activity was moderately to completely problematic in most tasks; 80% for rising from the toilet sit or squatting position, 67% for lowering to sit or squat and 53% for maintaining the toileting position. It has been reported that knee osteoarthritis caused the greatest burden on functional ability seemingly because of joint pain and stiffness[42] . Pain, joint stiffness, inflammation, joint degeneration and musculoskeletal alterations lead to functional disabilities such as difficulty in prolonged standing, sitting or squatting and in activities involving knee flexion and extension[43] . Dos Santos and his colleagues[43] findings may help to explain the difficulties experienced by the participants in the current study because the two ADLs (bathing and toileting) require getting into the sitting/squatting, sustaining the position for some time and then rising. The presence of pain and limitations in the ROM may have led to the challenges and difficulties in bathing and toileting for people with OA of the knee and hip observed in this study.
Disturbed biomechanics
Disturbed biomechanics of the joint surfaces and surrounding tissues could have contributed to the level of difficult in bathing and toileting. Movements and positions requiring a greater degree of movement were more problematic. Positioning in the tub and rising to standing were problematic in more than 50% of the participants while four percent could not rise from the bathing position without help. In reference to problems, 34% had moderate, 30% severe and 16% could not rise from the toileting position on their own. While in the toileting position (sitting or squatting) more than 52% of the participants reported difficulties ranging from moderate to complete. Absence of articular cartilage in OA, forces are not attenuated and are transmitted directly to the sub-chondral bone where the pain receptors are exposed[18] . This could cause pain and the natural reaction would be to halt the movement. In OA the homeostatic process of sub-chondral bone remodeling fails, resulting in change in articular surface shape, reduction in cartilage stiffness and its shock-absorbing capacity[44] . Thickened and most times laxed ligaments lead to joint instability and reduced proprioceptive ability within and around the joint. Wallace’s team in a systematic review explained that in knee OA, the anterior cruciate ligament which primarily prevents anterior translation of the tibia on the femur is degenerated[46] . These changes could result in either reduced range of motion or hypermobility/instability thereby limiting the usability of the joints in ADLs.
Kinetic change could partly be the reason for the problems in rising and sitting/squatting on the toilet or change of posture during bathing. Patients with OA[47] have four times higher odds of having muscle weakness. In the current study 34 and 30% had moderate and severe problems with rising from the sitting/squatting position in toileting respectively. Meanwhile 37% had moderate problems in rising from the bathing position in the bathtub. All these movements needed a concentric contraction of both hip and knee extensors when lowering and eccentric muscle work when rising. Muscle weakness may have negatively affected the force production in the extensors to allow easy rising from a lower position. If one has to sit on the toilet, there is flexion at the hip and knee in the same plane. This task needs eccentric muscle work from the quadriceps and glutei to control flexion initiated and performed by gravity. It was also possible that pain affected the biomechanics in the hip and the knee in the study sample[45] . In this study significant associations were found between the range of motion and severity of pain for the movements that important in bathing in the bathtub and toileting (hip flexion P= 0.01, hip extension P= 0.001, hip abduction p= 0.001 and knee flexion p=0.02). In bathing using a bathtub, there are several movements reaching several ranges of motion and different postures taken to completely bath. These movements and postures require a lot of muscle work and energy. For example, one may need to sit or squat to wash the perineum but stand to wash the gluteal region. For one to sit, he or she requires to eccentrically contract lower limb extensor muscles, reach at least 900 of hip and knee flexion then maintain the sitting or squatting position before rising using concentric muscle work at the hip and knee. Knoop and others[40] listed muscle weakness, proprioception disorder, high laxity, and excessive movements of knee as contributing to the difficult in sitting and squatting on the toilet. The sex distribution may have had an influence on the findings because there were more females who also had significantly higher severity of Pain (p = 0.0001). At the same time females had less mobility in most movements of the hip and knee (Table 1. This finding is similar to Oboirein[48] and Silverwood[7] and their respective colleagues who named being female as having a more influence on the development, severity and negative effects of OA. In this study it was found that pain and ROM were significantly associated[2] (Table 2).
CONCLUSION
Participants in this study had moderate to severe challenges in using their bathroom facilities. Rising from lower positions was the most difficult task in both bathing and toileting for people with hip and knee osteoarthritis. Pain, ROM and disturbed biomechanics seemed to be the main limiting factors.
What is already known on this topic:
The prevalence and pattern of OA of the knee and hip joints.
What this study adds
The study highlights challenges faced by people with OA of the hip and knee joints in using bathrooms
Suggests to rehabilitation specialists to consider the bathing and toileting facilities in order to understand the challenges people with OA of the knee and hip face during bathing and toileting
This study also highlights the need to grade the level of difficulty in using bathroom facilities using standard tools such as the ICF to understand the effect OA on activities of daily living, and monitor the progress of the condition and rehabilitation outcomes.
Study limitations
Information given by patients on pain scores was subjective and therefore only represented participants’ feelings at the time of data collection; the study did not compare problems in patients with hip OA and knee OA or those with both hip and knee OA. The BMI of the patients with hip and knee OA was not taken into account in this study.
RECOMMENDATIONS
The study makes the following recommendations:
- Both the assessment and management of OA patients of the hip and knee should take into account the bathing and toileting facilities of patients
- Future studies may be carried out with a larger population size to assess the level of difficulty faced by patients with hip and knee OA
- An observational study may be carried out on the level of difficulty faced by patients with OA of the hip and knee
- The ICF to be used by physiotherapists as a possible framework for organizing and directing treatment of patients with OA
Acknowledgements
The contribution of the following is acknowledged:
Conflicts of interest
Authors declared that they have no conflicts of interest
Competing interests
Authors declared that they have no competing interests
Funding statement
Not applicable
Authors’ contributions
- Billiat Chongo – principal supervisor, reporting results and drafting discussion
- Chese Ngulube – Data collection
- Sr Rebecca Majorie Mwansa – data analysis and study formatting
- Dominic Sashi – drafting of introduction section of manuscript
- Fair Banji Mwiinga – overall editing of manuscript
REFERENCES
- Alkuwaity, M., Alkhanani J. Ali B. Prevalence and determinant factors of Osteoarthritis of the knee joint among the Elderly in Arar, KSA. The Egyptian journal of hospital medicine, 2018 9(72), pp. 5173-5177.
- Kaur R., Ghosh A., Singh A. Prevalence of knee osteoarthritis and its determinants in 30-60 years old women of Gurdaspur Punjab. International Journal of Medical Science and Public Health, 2018 7(10), pp. 825-830.
- Osteoarthritis Research Society International. Osteoarthritis; a serious Disease submitted to the US, Food and Drug administration. 2016. [Online]. Available at: https://www.oarsi.org/education/oarsi [Accessed 5 December 2019].
- Usenbo, A., Kramer, V. & Musekiwa, A. Prevalence of arthritis in Africa: A systematic review and meta-analysis. Public Library of Science, 2015 10(8).
- Bija M. D., Luma, H. N. & Temfack, E. Patterns of knee osteoarthritis in a hospital in sub-Saharan Africa. Clinical. Rheumatoid. 2015 34(11), p. 1949–1953.
- Odole A., Ekediegwua E. B., Ekechukwu E. N. D. Correlates and predictors of pain intensity and physical function among. Musculoskeletal Science and Practice, 2019. 30(12), p. 150–156.
- Rayes C., Leyland M. K., Peat G., Cooper C., Adern K. N., Prieto-Alhambra. Association between overweight and obesity and risk of clinically diagnosed knee, hip, and hand osteoarthritis: a population-based cohort study, Arthritis and Rheumatology 2016 68(8): 1869-1875
- Jiang G., Zhu X., Rong J., Xing B., Wang S., Liu A., Chu M., Huang G. Obesity, osteoarthritis and genetic risk, Bone and Joint Research, 2018 7(7): 494-500
- World Health Organization (WHO). Reducing risks, promoting healthy life, Geneva: WHO. 2015
- Bottaro A. The Pathophysiology of Osteoarthritis https://www.verywellhealth.com/pathophysiology-osteoarthritis-5093836 [Accessed March 20, 2021] 2021
- Kamimura M., Nakamura Y., Uchiyama S., Ikegami S, Mukaiyama K, Hiroyuki Kato H. The Pathophysiology and Progression of Hip Osteoarthritis Accompanied with Joint Pain are Potentially Due to Bone Alterations - Follow-up Study of Hip OA Patients Open Rheumatology Journal; 2014 8: 46–53. doi: 10.2174/1874312901408010046
- Wieczorek M., Rotanda C., Guillemin F., Rat A. Pain, Functional Limitations and Physical Activity Participation Trajectories in Patients with Symptomatic Knee and Hip Osteoarthritis: A multi-trajectory analysis [abstract]. Arthritis Rheumatol, 2018 Volume 945.
- Miller E. R., Tran B. P., Sondoqah A., Raghu P., Ishihara S., Miller J.R., Malfait A. The Role of Peripheral Nociceptive Neurons in the Pathophysiology of Osteoarthritis Pain Current Osteoporosis Reports. 2015 13(5): 318–326. doi: 10.1007/s11914-015-0280-1
- Leopold S. S. Osteoarthritis of the hip (Hip arthritis). 2015. Available at http://www.orthop.washingtom.edu/patient-care/articles/hip/osteoarthritis-of-the-hip-hip-arthritis.html [Accessed 23 December, 2020]
- Barr A.J., Campbell T.M., Hopkinson D. et al. A systematic review of the relationship between subchondral bone features, pain and structural pathology in peripheral joint osteoarthritis. Arthritis Research & Therapy 2017 17, 228 https://doi.org/10.1186/s13075-015-0735-x
- Hunter D. J. and Johnson V. L. The epidemiology of osteoarthritis. Best practice & Research, 2014 Volume 28, pp. 5-15
- Moss A., Murphy L., Helmick C. Annual incidence rate of hip symptoms and three hip OA outcomes from a U.S population -based cohort study, The Journal County Osteoarthritis Project. Osteoarthritis Cartilage , 2014 24(9), pp. 1518-1518
- Weinstein S., Waltkins-Castillo S., Singh K. Musculoskeletal Diseases and the burden of they cause in the United States. Prevalence, Societal and Economical cost, 2015 4(2), p. 102.
- Lespasio A., Deshpande R. B., Katz J. N., Hunter D.J. Number of persons with symptomatic knee osteoarthritis in the US; impact of race and ethnicity, age, sexual and obesity. Arthritis Care & Research, 2017 68(12), pp. 1743-1750.
- Cerit B. Determination and evalation of the needs of the patients with knee Osteoarthritis in their daily living activities. Procedia - Social and Behavioral Sciences, 2014 Issue 152, pp. 841-844.
- Lunn D., Lampropoulos A. Stewart T. Basic biomechanics of the Hip. Orthopedics and Trauma, 2016 30(3), pp. 239-246.
- Neumann A. D. Hip in Kinesiology of the musculoskeletal system: Foundations for Rehabilitation, ed. D. A Neumann (Mosby) 2010 465 - 518
Medical Journal of Zambia, Vol 50, 1
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.