The association of Primary Biliary Cholangitis and Graves’ disease coupled with management challenges: a case report of a 36-year-old black Zambian female patient
Sydney Mpisa
University of Zambia
Edford Sinkala
University of Zambia School of Medicine, University Teaching Hospital, Liver Clinic
Wamundila Kawana
University of Zambia School of Medicine, University Teaching Hospital, Liver Clinic
Brown Kamanga
University of Zambia School of Medicine, University Teaching Hospital, Endocrine Unit
DOI: https://doi.org/10.55320/mjz.50.1.382
Keywords:PBC, Grave’s disease, autoimmune
ABSTRACT
The occurrence of other autoimmune conditions in primary biliary cholangitis (PBC) patients is documented in literature and thyroid disease is such an example. Such cases are however rarely seen in the African setting and particularly in Zambia. Here we report a case of a 36-year-old black Zambian female patient who was diagnosed with PBC in 2014 at the University Teaching Hospital(UTH), Lusaka, Zambia. She was lost to follow-up until November 2020 when she presented with a flare of PBC. During the flare the patient reported a 2-weeks history of pruritus, fatigue, passing dark urine and pale stools, coupled with progressive weight loss. Examination revealed moist skin, scleral jaundice, generalised scratch marks, wasting with a body mass index (BMI) of 15kg/m2, a small goitre with a bruit heard over it and fine tremors. She did not have proptosis, finger clubbing or cervical lymphadenopathy or pretibial myxoedema. File review showed no prior goitre. Ultrasound of the neck confirmed the homogenous thyroid gland with increased vascularity. Blood tests revealed a suppressed thyroid stimulating hormone (TSH) (<0.005Uiu/ml) elevated free triiodothyronine (FT3) (10.9pmol/l) and elevated free thyroxine (FT4) (53.4pmol/l). TSH receptor antibodies were also elevated. The clinical features and blood tests led to the confirmation of Graves’ disease in a patient with PBC. Our patient was subsequently started on carbimazole, propranolol and continued ursodeoxycholic acid with great clinical response to treatment of both the PBC and Graves’ disease.
Our patient managed to gain weight within six months of commencement of Graves’ hyperthyroidism treatment, with her BMI improving to normal, at 22.6 Kg/m2. One year into her treatment she developed agranulocytosis likely from the carbimazole which was subsequently stopped resulting in her thyroid hormones going up again. The patient could not take propylthiouracil (PTU) in view of the liver disease as such radio-active iodine (which is not readily available) was the only feasible option.
Our case report contributes to the body of knowledge that PBC tends to coexist with autoimmune thyroid disease and should be looked out for with a high index of suspicion especially in patients with PBC who report weight loss despite doing well on PBC therapy. We also seek to highlight the challenges in management and follow up of such patients in low resource setting. Although PBC is not so common in Black Africans, it should be suspected in patients who present with cholestatic jaundice especially in young female patients.
INTRODUCTION
Cholestatic liver conditions are a common cause of presentation to our liver clinic at UTH, Lusaka Zambia. The cholestatic liver conditions we usually see include gallstone obstructive jaundice, drug induced liver injury, malignancies and rarely autoimmune liver conditions. Primary biliary cholangitis is one of the autoimmune cholestatic liver conditions usually seen in women aged 30-65 years. It is a chronic autoimmune inflammatory disease of the liver small bile ducts. Being a T-cell mediated autoimmune condition it is associated with other autoimmune conditions like Sjogren disease, rheumatoid arthritis, scleroderma and thyroiditis[2] . Grave’s disease which is an autoimmune disorder characterised by hyperthyroidism due to circulating autoantibodies has been found to be often associated with PBC. The occurrence of PBC and Grave’s disease together is uncommon or under-reported in our African setting. We therefore set out to write a case report we managed in a resource constraint community of Lusaka, Zambia.
CASE HISTORY
A 36-year-old black Zambian female patient being followed for PBC confirmed by a liver biopsy in 2014. She presented to the outpatient wing (liver clinic), department of Internal Medicine, at the University Teaching Hospital in Lusaka, Zambia in November 2020 with a 2-weeks history of jaundice, fever, generalised pruritus, weight loss and fatigue. Prior to 2020, the patient was doing well on her PBC therapy despite the continued weight loss.
In 2014 the patient had been diagnosed with HIV disease, for which she was taking a triple therapy antiretroviral therapy consisting of Tenofovir, Lamivudine and Efavirenz with good viral control. The patient was then lost to follow-up until November, 2020.
CLINICAL FINDINGS
The initial general clinical evaluation of the patient in November 2020 revealed generalised wasting (BMI of 15kg/m2), scleral jaundice, moist skin, generalised scratch marks, shiny nails and a fine tremor. Neck examination revealed a bi-lobed mass anteriorly, with a bruit heard over it on auscultation. Her blood pressure was normal, but she had an elevated radial pulse of 110/minute, regular and synchronic with her heart beat. She did not have proptosis, cervical lymphadenopathy or pretibial myxoedema.
DIAGNOSTIC ASSESSMENT
Thyroid ultrasound showed a homogenously enlarged thyroid gland with increased vascularity. No cervical lymph node enlargement was noted.
Laboratory results showed elevation of both free T3 and free T4 with a suppressed TSH (Table 1), in keeping with thyrotoxicosis. Anti-TPO, anti-TG and anti-TSH receptor were elevated (Table 2), confirming the diagnosis of Graves’ disease. Table 3 shows the latest liver enzymes which shows a cholestatic picture due to the PBC.
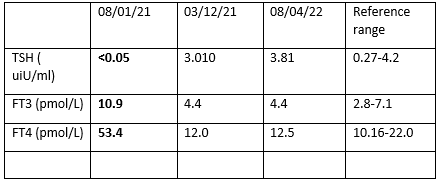
Key
TSH: Thyroid stimulating hormone
FT3: Free triiodothyronine
FT4: Free thyroxine


OTHER SIGNIFICANT RESULTS
Liver stiffness measured by Fibroscan was in the cirrhotic range (21.7kPa), normal range (4- 7kPa). Gastroscopy showed no evidence of oesophageal or gastric varices.
Due to diagnostic challenges, we did not do radioactive iodine 123 uptake scan or evaluate markers of bone resorption resulting from thyrotoxicosis, such as bone specific alkaline phosphatase, osteocalcin and procollagen peptides.
THERAPEUTIC INTERVENTION AND CHALLENGES
Patient was started on carbimazole 25mg orally per day while propranolol 20mg orally twice daily was given to normalise the pulse rate, control the excessive sweating and help reduce conversion of T4 to T3. She also continued on ursodeoxycholic acid 300mg per oral twice daily. The patient could not afford the cost of ursodeoxycholic acid as such she was under-dosing herself by taking 300mg once daily.
FOLLOW UP AND OUTCOME
The patient became euthyroid on subsequent visits in the Endocrine clinic, gaining her baseline weight from a BMI of 15kg/m2 to BMI 22.6kg/m2 within 6 months (pictures shown below). After becoming euthyroid on carbimazole the patient developed agranulocytosis 1 year into treatment which prompted to stop the anti-thyroid drugs. The patient could not take PTU in view of the PBC and therefore she is being evaluated for radio-active iodine treatment. Patient is currently stable with further 3-monthly regular follow-up in both the Liver and Endocrine clinics at University Teaching Hospital Lusaka, Zambia.
DISCUSSION
Primary biliary cholangitis is a chronic cholestatic liver disease characterised by a T-cell mediated attack on small intralobular bile ducts. The sustained loss of bile ducts causes signs and symptoms of cholestasis which eventually result in cirrhosis and liver failure[1] . PBC is common in females of Asian and European descent, literature on the epidemiology of PBC in African black patients is lacking.
The use of ursodeoxycholic acid has resulted in most patients having normal life expectancy with only a few developing liver cirrhosis. Associations between PBC and other autoimmune diseases has been described with Sjogren disease, rheumatoid arthritis, SLE, scleroderma and thyroiditis being among the reported associations[2] . Thyroid disease linked to PBC has been reported in few case reports mainly among Asian and European populations[3] . Autoimmune hypothyroidism is a prominent feature in PBC occurring in 10-25% of the patients[4] .
Graves’ disease and PBC occurring together has been reported in literature but is not a common finding. The outcome of patients with PBC can be altered as the hypermetabolic state produced by Graves’ disease can affect drug metabolism and increase catabolic state thus worsen weight loss. Follow up of patients with PBC and Graves’ disease needs great attention as elevations in ALP can occur from: 1-the increased bone turnover 2-thyrotoxicosis 3-carbimazole causing cholestasis. Elevations of alkaline phosphatase (ALP) are common in thyrotoxicosis occurring in 64% of patients, however this elevation is not always liver specific as such there is need to assess gamma-glutamyl transferase (GGT) and bilirubin as indicators of cholestasis[5] . Some literature suggests that hypothyroidism is protective in patients with liver cirrhosis as studies showed reduced incidence of decompensated cirrhosis in patients with hypothyroidism however no clear evidence suggests that hyperthyroidism causes cirrhosis[6] .
In a literature review published in 2015, 24 reported patients of concomitant PBC and GD, all involving females, there was no clear tendency for one disease to precede the other[3] . A complex relationship exists between the liver and the thyroid gland; therefore, clinicians should not treat these conditions in isolation. Besides autoimmune conditions, other conditions can affect both organs and these include; malignancies (non-Hodgkin lymphoma), amyloidosis, hemochromatosis, and drugs (amiodarone, mefloquine, carbamazepine)[7] .
We know that HIV infection can cause cholestasis, making it difficult to diagnose PBC in a patient with HIV infection. Cholestasis in HIV infection can be due to the HIV drugs, opportunistic infections and less commonly HIV-related malignancies. HIV-associated cholangiopathy is a differential to consider, caused by biliary obstruction resulting from benign stricture of the biliary tract in patients with advanced AIDS[8] . The occurrence of HIV-cholangiopathy has declined since the antiretroviral era. Our patient has been virally suppressed with good immunological control making HIV less likely to be the cause of cholestasis. There are some studies that suggest an increase in autoimmune conditions including PBC and Graves’ disease in HIV infected patients[8-9] .
TAKE HOME LESSONS
1. The association between PBC and Graves’ disease among black African patients is uncommon but should be considered.
2. Agranulocytosis in patients on carbimazole is a common complication and usually PTU is the substitute but in comorbid liver disease we can’t use it thus radio-active iodine (which is not readily available in Zambia) becomes the most suitable option in patients who decline surgery.
3. Liver disease in the HIV population is common because of the effects of the HIV, HIV drugs, hepatitis viruses and other opportunistic infections. However, clinicians should be on the lookout for autoimmune liver conditions as well.
4. Fatigue is a common complaint among patients with liver or thyroid disease. If both diseases occur in one patient, fatigue might be worse.
5. Cholestasis can result from hyperthyroidism or treatment with carbimazole, therefore close follow up is needed in patients with PBC and hyperthyroidism.
PATIENT PERSPECTIVE
“I feel normal now, this is my normal weight and l am grateful to the doctors at UTH. I still have episodes of itchiness but l learnt to live with that. My only other challenge is the cost of the ursodeoxycholic acid.”
Informed consent
The patient provided a written consent and agreed with the case write-up and its subsequent publication.
Authors contributions
All the authors contributed equally in the case report writing.
Acknowledgements
Dr Mubbunu Malambo: The head of Gastroenterology unit at UTH, Lusaka, Zambia.
ABBREVIATIONS
ALP--------------------------------------------- Alkaline Phosphatase
AST--------------------------------------------- Aminotransferase
ALT---------------------------------------------- Alanine transferase
BMI--------------------------------------------- Body Mass Index
PBC--------------------------------------------- Primary Biliary Cholangitis
GGT--------------------------------------------- Gamma glutamyl transferase
GD----------------------------------------------- Graves’ Disease
UTH---------------------------------------------- University Teaching Hospital
SLE------------------------------------------------ Systemic Lupus Erythematosus
TSH----------------------------------------------- Thyroid stimulating hormones
FT4----------------------------------------------- Free Thyroxine
FT3----------------------------------------------- Free Triiodothyronine
REFERENCES
- Selmi, C., R.L. Coppel, and M.E. Gershwin, Primary biliary cirrhosis, in The Autoimmune Diseases. 2006, Elsevier. p. 749-765.
- Islam, S., J. Riordan, and J. Mcdonald, Case report: a rare association of primary biliary cirrhosis and systemic lupus erythematosus and review of the literature. Journal of gastroenterology and hepatology, 1999. 14(5): p. 431-435.
- Shizuma, T., Clinical characteristics of concomitant systemic lupus erythematosus and primary biliary cirrhosis: a literature review. Journal of immunology research, 2015. 2015.
- Sherlock, S. and P. Scheuer, The presentation and diagnosis of 100 patients with primary biliary cirrhosis. New England Journal of Medicine, 1973. 289(13): p. 674-678
- Doran, G., Serum enzyme disturbances in thyrotoxicosis and myxoedema. Journal of the Royal Society of Medicine, 1978. 71(3): p. 189-194.
- Mosin, V.I., [Thyroid gland and the liver]. Klin Med (Mosk), 1973. 51(10): p. 21-8.
- Malik, R. and H. Hodgson, The relationship between the thyroid gland and the liver. QJM: An International Journal of Medicine, 2002. 95(9): p. 559-569.
- Imai, K., et al., Progressive HIV-associated cholangiopathy in an HIV patient treated with combination antiretroviral therapy. Internal Medicine, 2016. 55(19): p. 2881-2884.
- Silva, G.A.R.d., et al., Association between antiretrovirals and thyroid diseases: a cross-sectional study. Archives of Endocrinology and Metabolism, 2015. 59: p. 116-122.
Medical Journal of Zambia, Vol 50, 1
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.