Impact of introduction of TB LAM in the TB testing algorithm at Levy Mwanawasa University Teaching Hospital on case detection and notifications
Ireen Chanda Bwalya
Levy Mwanawasa University Teaching Hospital, Department of Infectious Diseases, Lusaka, Zambia.
Obvious Chilyabanyama
Centre for Infectious Disease Research, Lusaka, Zambia.
DOI: https://doi.org/10.55320/mjz.50.1.374
Keywords:Lipoarabinomannan, Diagnose, Hospital, Algorithms, Tuberculosis
ABSTRACT
Background:TB-LAM tests were introduced in the TB program in Zambia in 2019, to aid in diagnosis of TB. We carried out a study to determine the impact that TB lipoarabinomannan (LAM) test has had on case identification and notification at a tertiary hospital in a city with a high prevalence of HIV. We also compared sensitivity, specificity, positive predictive value and negative predictive of TB LAM tests and X-pert MTB RIF test in HIV positive and HIV negative patients.
Method:Retrospective analysis of the TB laboratory as well as the TB notification registers to determine the number of TB cases identified by TB LAM and Xpert MTB-RIF. We identified patients who had both TB LAM and X-pert MTB RIF tests to determine sensitivity, specificity, positive and negative predictive values of TB LAM and Xpert MTB RIF, using TB notification and commencement of anti-tuberculosis treatment as the gold standard for comparison.
Results:Between January 2019 and June 2022, there were a total number of 2353 notified cases of Tuberculosis. A total of 511 cases of Tuberculosis were identified on the basis of positive TB LAM. This accounted for 59% of all bacteriologically confirmed cases of TB. The sensitivity and specificity of TB LAM in diagnosis of TB in the study population was 55.8% and 91.4% respectively. Positive and Negative predictive values for TB LAM were 84.5% and 69.6% respectively. The sensitivity and specificity of Xpert MTB RIF in diagnosis of TB in the study population was 29.2% and 98.2% respectively. Positive and Negative predictive values for Xpert MTB RIF were 93.5% and 60.4% respectively. Positivity yield was higher for TB LAM as compared to Xpert MTB RIF (19% versus 9% in 2019; 36% versus 10% in 2020 and 38% versus 10% in 2021).
Conclusion: TB LAM identified 59% of all bacteriologically confirmed cases of tuberculosis at Levy Mwanawasa University Teaching Hospital. Contrary to what has been found in other studies, the sensitivity of TB LAM was much higher than that of Xpert MTB RIF. In addition, the sensitivity of TB LAM was higher in HIV negative as compared to HIV positive, which is contrary to what has been established in similar studies.
INTRODUCTION
Tuberculosis (TB) is among the leading causes of mortality and morbidity globally. In 2021, it is estimated that 10.6 million people were infected with tuberculosis. There were an estimated 1.6 million deaths attributable to TB in the year 2021, of which 187,000 deaths occurred among patients living with HIV [1] . Zambia is one of the thirty high burden TB countries in the world. In 2018, the incidence of TB in Zambia was estimated to be 346 per 100, 000 population [2] . The diagnosis of TB in Zambia is mainly by chest X-ray. However, not all health care facilities in Zambia have X-ray services. In many instances, patients have to travel considerable distances to other health care facilities to have X-rays done. This introduces significant costs to the patients, and creates diagnostic delays. According to the Zambia National TB program, the gold standard for diagnosing TB is examination of sputum by Xpert MTB RIF. However, not all facilities are able to examine sputum by gene X-pert examination. In addition, the yield of gene X-pert for the diagnosis of Mycobacterium TB is low in our patient population, due the high prevalence of Human Immunodeficiency infection (HIV). Patients with TB and HIV co-infection usually have paucibacillary disease; thereby making the diagnosis of TB in this patient population challenging.[3]
TB LAM is a point of care mycobacterial test that detects the presence of lipoarabinomannan antigen in urine. Lipoarabinomannan is a component of the mycobacterium TB cell wall that is released into the blood, and consequently filtered into urine as the mycobacteria degrade[4] . In 2015, the World Health Organization (WHO) issued a policy guidance recommending the use of TB LAM in patients with advanced HIV. This is because the sensitivity of TB LAM is higher in patients with advanced HIV. TB LAM is not recommended for use in HIV negative patients, because the sensitivity of TB LAM in HIV negative patients is very low [5] .
Estimates of the sensitivity and specificity of TB LAM have been variable across studies. One meta-analysis showed sensitivity estimates ranging from 13 to 93% and specificity estimates ranging from 87% to 99% [6] ; while another gave sensitivity range of 8.3-93%, and specificity estimates of 93.9-100% [7] . In another study that was carried out among hospitalized patients, the sensitivity of TB LAM in HIV positive patients with bacteriologically confirmed TB was 59%. The specificity of TB LAM in HIV positive patients who were TB negative by culture was 96% [8] . Another study showed that the sensitivity of TB LAM in patients with CD4 counts lower than 50 was 45%. In this study, the specificity and positive predictive value of TB LAM was greater than 80% [9] .
Available literature suggests that when used in the recommended population, TB LAM increases the number of patients diagnosed with TB. A Cochrane systematic review concluded that when used in in-patient settings, TB LAM reduced mortality probably by facilitating prompt diagnosis and treatment initiation [10] . In a prospective observational study that was done among HIV positive ambulatory patients in Kenya, the addition of TB LAM to the diagnostic algorithm that included smear microscopy, gene X-pert and culture, increased the diagnostic yield from 36.6% to 84% [11] . The STAMP trial, which was a double blind, multi-center randomized controlled trial also showed similar results. In this study, the use of TB LAM provided the highest diagnostic yield (75%) as compared to urine expert (35%) and sputum expert (40%) [12] . In a study that was done in Zambia, TB LAM was shown to reduce the time to diagnosis and treatment among people living with HIV. The sensitivity of TB LAM in this study population was shown to be highest in those with lower CD 4 counts [13] . However, in a multicenter study that was conducted in Zambia, Tanzania and South Africa, it was found that among HIV positive patients who had culture positive TB; TB LAM did have any significant impact on the testing algorithm as an adjunct to smear microscopy or Xpert MTB-RIF. The researchers concluded that TB LAM did not increase same day treatment initiation in settings where X-rays were available [14] . In view of these conflicting findings, it is imperative that we review the impact that LAM has had on the testing algorithm at Levy Mwanawasa University Teaching Hospital in Lusaka, Zambia. Most of the studies that have evaluated TB-LAM have done so under optimal research conditions, with CD4 count available for all study participants. However, this study was carried out using routine clinical data, and is therefore more likely to yield results that represent the actual impact of TB LAM on case identification and notification; in a real life clinical setting, where CD4 count results are not always available. The purpose of this study is to determine the impact that the introduction of TB LAM has had on case detection and notifications, and to determine sensitivity and specificity of TB-LAM, using TB notification, and Gene Xpert as the gold standard.
METHODS
Study Design
This was a retrospective review of TB laboratory and notification registers at Levy Mwanawasa University Teaching Hospital. The TB laboratory registers in one of the monitoring and evaluation tools for the Zambia National TB program. It is available at all health facilities that have a laboratory on site. The results of all TB microbiological tests such as smear microscopy, TB LAM tests and Gene X-pert MTB tests are entered in the laboratory register. Patient information such as age, sex, address, and HIV status are recorded in the laboratory register. The TB notification register records all patients diagnosed with TB at a health facility. This includes those diagnosed with TB using X-rays, as well as those with extra-pulmonary TB. In addition to the patient information such as age, sex, address, and HIV status, the TB notification register also records the episode of TB (i.e. new, relapse or treatment after failure) smear microscopy results during treatment and final outcome of treatment.
Study Site
The study was conducted at Levy Mwanawasa University Teaching Hospital. This is a tertiary Hospital located in the capital Lusaka. Being a referral hospital, a significant number of cases of disseminated TB and advanced HIV are admitted to this hospital. Levy Mwanawasa Hospital has laboratory facilities where smear microscopy, gene X-pert and TB LAM tests are done.
Operational Definitions
The following operational definitions recommended by the National TB and Leprosy Program apply to this study:
Presumptive TB: A patient presenting with symptoms and signs suggestive of Tuberculosis.
Bacteriologically Confirmed TB: Biological specimen is positive by smear microscopy, culture or World health Organization (WHO) approved rapid diagnostic tests such as Xpert MTB/RIF, line probe assay (LPA), and lateral flow urine lipoarabinomannan (LF-LAM) assay.
Clinically Diagnosed TB: Does not fulfill the criteria for bacteriological confirmation, but TB been diagnosed based on clinical or radiological features.
Study Population
The study reviewed TB LAM and Gene Xpert test results for patients seen at Levy Mwanawasa University Teaching from 2019 to 2022. The TB-LAM test used at Levy Mwanawasa Teaching Hospital is the Alere Determine TB LAM antigen test (LF-LAM). These were supplied to the facility either directly by Medical Stores of Zambia, or procured for use in the TB program by our partner TB Local Organization Network (TB LON). Testing for MTB by Gene Xpert was done on the Cepheid MTB/RIF Testing Machine. All TB LAM an Xpert MTB tests were done in the Lab according to laid down standard operating and quality assurance proceedures. HIV testing was done either in the lab by trained staff, or by HIV counselors at the bedside. The HIV tests were conducted according to the HIV testing algorithms. Determine Rapid HIV test Kit was used as the initial screening test. This was then followed by confirmatory HIV testing using SD Bioline HIV test Kits.
Selection and recruitment procedures
Simple random sampling was used to select an appropriate sample. Using the data extraction template, a list of all patients that have had both an Xpert MTB test and TB LAM test was generated. Sequential numbers were assigned to each patient entry. A random number list was created by using a random number generator. Based on the random numbers generated, a random sample was selected.
Study Inclusion Criteria
To be considered for inclusion, lab and treatment register patient information was required to meet the criteria below:
Legible entries
complete demographic information
Results of TB LAM and Gene Xpert
Study Exclusion Criteria
Ineligible and incomplete entries
Missing or incomplete demographic information
Missing TB LAM or gene Xpert results
Data Collection
Data was extracted from the registers and entered into excel for cleaning. It was subsequently transferred to SPSS for analysis. Data that was collected from the registers included demographic variables (age, sex, and home address), HIV status and results of Gene Xpert and TB LAM tests.
Statistical Analysis
Data was analyzed using SPSS version 23. The primary outcome measure is the number of TB LAM and Gene Xpert tests that were positive and subsequently entered in the TB notification register. The proportion of cases notified based on positive TB LAM tests were compared to the proportion of patients being notified based on positive X-pert MTB test. Chi-square will be used to determine whether there is any significant difference between the two proportions. A significance level p less than 0.05 will be considered as statistically significant. The incremental yield was determined by calculating that number of notifications attributable to TB-LAM test alone.
Ethical Consideration
Ethical approval for this study was granted by the University of Zambia Biomedical Research Ethics committee (UNZABREC) and the National Health Research Authority under the reference. A waiver of consent was granted because the study met all the requirements for waiver of consent. Several steps were taken to ensure that all personally identifying information was kept private, and that confidentiality was maintained. Only the PI had access to the personally identifying information. Data was kept on a password protected computer. Treatment notification and laboratory registers were kept under lock and key within the TB unit throughout the study.
RESULTS
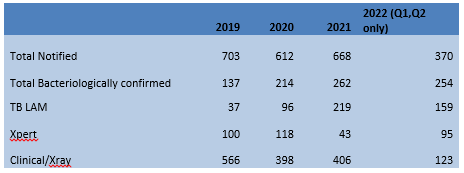
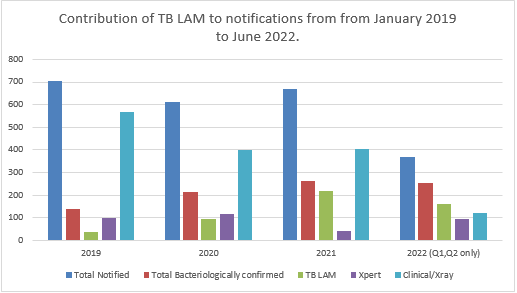
In 2019, a total of 703 patients were diagnosed with Tuberculosis and commenced on treatment. The marjority of these patients had pulmonary tuberculosis (PTB). The total number of bacteriologically confirmed cases of TB in 2019 was 137. Out of these, 37 (27%) cases were notified based on positive TB LAM. The positivity yield for TB LAM tests in this year was 19%, as compared to 9% for Xpert MTB-RIF examination of sputum. In 2020, a total of 612 patients were diagnosed with TB and notified. In this year, there were a total number of 214 bacteriologically confirmed cases of TB. Out of these 96 (45%) cases were notified on the basis of positive TB LAM. In 2020, the positivity yield for TB LAM was much higher than that for Gene X-pert (36% versus 10% respectively). In 2021, a total of 668 patients were diagnosed with TB and notified. In this year, there were a total number of 262 bacteriologically confirmed cases of TB. Out of these 219 (84%) cases were notified on the basis of positive TB LAM. The positivity yield for TB LAM in 2021 was 38%, while that for gene Xpert was 9%. Between January and June 2022, there have been a total number of 370 notifications. Out of these, 254 (69%) are bacteriologically confirmed TB cases. Of the 254 bacteriologically confirmed TB cases, 159 (63%) patients were diagnosed and notified based on a positive TB LAM test. The contribution of TB LAM to notification between 2019 and 2022 are shown in the table and graph below:
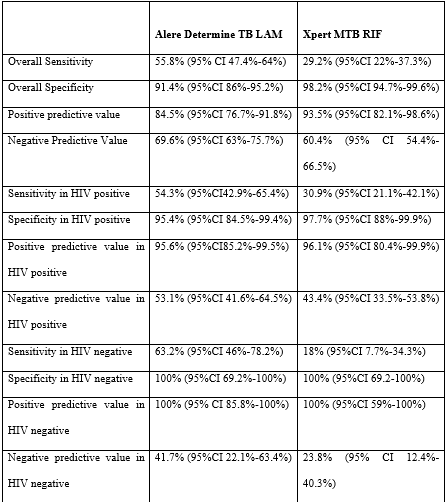
The overall sensitivity of TB LAM in diagnosis of TB in the study population was 55.8%. The specificity of TB LAM was found to be higher, at 91.4%. The positive and negative predictive values of TB LAM were 84.5% and 69.6% respectively. Among HIV positive patients, the sensitivity of TB LAM for the diagnosis of TB was 54.3%, while the specificity was 95.4%. The positive and negative predictive values of TB LAM test among patients with HIV were 95.6% and 53.1% respectively.
Among HIV negative patients, the sensitivity of TB LAM for the diagnosis of TB was 63%, while the specificity was 100%. The positive and negative predictive values of TB LAM test among HIV negative patients were 100% and 41.7% respectively.
The overall sensitivity of Xpert MTB RIF in diagnosis of TB was 29.2%. The specificity of Xpert MTB RIF was found to be higher, at 98.2%. The positive and negative predictive values of Gene Xpert MTB RIF were 93.5% and 60.4% respectively. Among HIV positive patients, the sensitivity of Gene Xpert MTB RIF for the diagnosis of TB was 30.9%, while the specificity was 97.7%. The positive and negative predictive values of Gene Xpert MTB RIF test among patients with HIV were 96.1% and 43.4% respectively.
Among HIV negative patients, the sensitivity of Gene Xpert MTB RIF for the diagnosis of TB was 18%, while the specificity was 100%. The positive and negative predictive values of Gene Xpert MTB RIF test among HIV negative patients were 100% and 23.8% respectively. A comparison of sensitivity, specificity and predictive values of Alere Determine TB-LAM and Xpert MTB RIF are shown in the table 2 below:
DISCUSSION
Out of the 2353 cases of tuberculosis that were identified between January 2019 and June 2022, 21.7% were identified by TB LAM whereas 15.1% were identified by Xpert MTB RIF. This shows that LAM is contributing to the identification of bacteriologically confirmed TB cases. This has implications on contact tracing, and the provision of TB preventative treatment. Current practice is to follow up only contacts of bacteriologically confirmed TB patients. TB LAM is increasing the number of households that are screened for TB, and consequently TB case detection and the provision of TB preventative therapy.
In their multi-centre study, Peter et al. concluded that TB LAM did not have any significant impact on the testing algorithm as an adjunct to smear microscopy or Xpert MTB-RIF. [14] We disagree with these findings, based on the results of our analysis. In the same study, Peter et al concluded that where X-rays are available, TB LAM is unlikely to increase same day initiation of treatment. We agree with this finding. Most cases of TB at our hospital are diagnosed by chest X-ray.
The sensitivity and specificity of TB LAM among HIV positive patients in our study was higher than that found in other studies [12-15] . The difference may be due to differences in the gold standard used. Other studies have used TB culture as the gold standard [10-13] while our study has used TB notification to indicate definite TB. Not all studies that have evaluated sensitivity and specificity of TB-LAM have used TB culture as the gold standard. Tessema et al carried out a study to determine the sensitivity and specificity of TB-LAM among Ethiopian patients. In their study, TB was confirmed by positive smear microscopy and by clinical symptoms of TB. In this study the sensitivity and specificity of TB LAM 74% and 86.9% respectively. Their study had higher sensitivity of TB LAM and lower specificity, as compared to our study. The positive and negative predictive values were 58.5% and 93.0% [15] . In the study by Huerga et al, the gold standard used to determine TB LAM sensitivity and specificity was Xpert examination of sputum, not TB culture [11] . The sensitivity and specificity of TB LAM in HIV negative patients was higher than that observed in other studies[6,8,9,17] . This has to be investigated further. There are suggestions that the degree of positivity, based on the intensity of the test bands could affect sensitivity estimates, with suggestions that faint lines could be false positive [18] . Our study could not address this coming concern as it was retrospective in nature. This could have affected the results.
We will source funding to evaluate TB LAM in HIV negative patients, using culture as the gold standard; and then compare with other studies. The positive predictive values of TB-LAM in HIV positive and HIV negative patients was similar to that which was found in other studies. [8] Other limitations of this study were the absence of CD 4 cell count results, and missing HIV test results for some patients.
CONCLUSION AND RECOMMENDATIONS
TB LAM is useful for identifying patients with TB. Where available, TB LAM test should be offered to HIV positive patients, as well as HIV negative patients unable to provide sputum samples. TB LAM is also a useful marker of mortality, and thus can be used as a prognostic marker.[4,14,19]
AUTHORS CONTRIBUTIONS
Conceived the study, collected data and participated in the analysis: IB
Analyzed data: OC
Wrote the paper: IB, OC
All authors read and approved the final manuscript
Competing interest
None
REERENCES
- Huerga, H., Ferlazzo, G., Bevilacqua, P., Kirubi, B., Ardizzoni, E., Wanjala, S. et al. Incremental yield of including Determine TB LAM Assay in the Diagnositic Algorithms for hospitalized and ambulatory HIV positive patients in Kenya. PLos ONE. 2017; 12(1): e10170976.doi:10. 1371/journal.pone.0170976.
- World Health Organization. Country profiles for 30 high TB burden countries. 2021, Available at: https://www.who.int/news/item/17-06-2021-who-releases-new-global-lists-of-high-burden-countries-for-tb-hiv-associated-tb-and-drug-resistant-tb (Accessed 17th June 2023).
- Lawn, S.D., Dheda, K., Kerkhoff, A.D., Peter, J.G., Dorman, S., Boehme, C.C. and Nicol, M.P. Determine TB LAM lateral flow urine antigen assay for HIV-associated tuberculosis: recommendations on the design and reporting of clinical studies. BMC Infectious Diseases. 2013; 407. https://doi.org/10.1186/1471-2334-13-4072
- Bulterys, M. A., Wagner, B., Redard-Jacot, M., Suresh, A., Pollock, R.N., Moreau, E. et al. Point-Of-Care Urine LAM Tests for Tuberculosis Diagnosis: A Status Update. J Clin Med. 2019; 9(1):111. doi: 10.3390/jcm9010111
- World Health Organization. The use of lateral flow urine lipoarabinomannan assay (LF-LAM) for the diagnosis and screening of active tuberculosis in people living with HIV: policy guidance. 2015. Available at: https://apps.who.int/iris/handle/10665/193633
- Minion, J., Leung, E., Talbot, E., Dheda, K., Pai, M. and Menzies, D. Diagnosing tuberculosis with urine lipoarabinomannan: systematic review and meta-analysis. European Respiratory Journal. 2011; 38(6): 1398-1405.
- Chatla, C., Mishra, N., Jojula, M., Adepu, R. and Mallikarjun P. A systematic review of utility of urine lipoarabinomannan in detecting tuberculosis among HIV-positive tuberculosis suspects. Lung India. 2021; 38(1): 64-73.
- Shah, M., Variava, E., Holmes, C.B., Coppin, A., Golub, J.E., McCallum, J. et al. Diagnostic accuracy of a urine lipoarabinomannan test for tuberculosis in hospitalized patients in a High HIV prevalence setting. J Acquir Immune Defic Syndr. 2009;52(2):145-151. doi:10.1097/QAI.0b013e3181b98430
- Suwanpimolkul, G., Kawkitinarong, K., Manosuthi, W., Sophonphan, J., Gatechompol, S., Ohata, P. et al. Utility of urine lipoarabinomannan (LAM) in diagnosing tuberculosis and predicting mortality with and without HIV: prospective TB cohort from the Thailand Big City TB Research Network. International Journal of Infectious Diseases. 2017; 59: 96-102.
- Nathavitharana, R.R., Lederer, P., Chaplin, M., Bjerrum, S., Steingart, K.R. and Shah, M. Impact of diagnostic strategies for tuberculosis using lateral flow urine lipoarabinomannan assay in people living with HIV. Cochrane Database of Systematic Reviews. https://doi.org/10.1002/14651858.CD14641.
- Huerga, H., Ferlazzo, G., Bevilacqua, P., Kirubi, B., Ardizzoni, E., Wanjala, S. et al. Incremental yield of including Determine TB LAM Assay in the Diagnositic Algorithms for hospitalized and ambulatory HIV positive patients in Kenya. PLos ONE. 2017; 12(1): e10170976.doi:10. 1371/journal.pone.0170976.
- Gupta-Wright, A., Corbett, E.L., Van Oosterhout, J., Wislon, D., Grint, D., Alufandika-Moyo, M. et al. Rapid urine based screening for tuberculosis in HIV-positive patients admitted to hospital in Africa (STAMP): a pragmatic, multicenter, parallel-group, double-blind, randomized controlled trial. The LANCET. 2018; 392(10144): 292-301.
- Kasaro, M.P, Chilyabanyama, O.N., Shah, N.S., Muluka, B., Kapata, N., Kruuner, A. et al. Performance of Xpert MTB/RIF and Determine TB-LAM Ag in HIV-infected adults in peri-urban sites in Zambia. Public Health Action. 2020; 10(4): 134-140.
- Peter, J., Theron, G., Chanda, D., Clowes, P., Rachow, A., Lesosky, M. et al. Test characteristics and potential impact of the urine LAM lateral flow assay in HIV infected out-patients under investigation for TB and able to self-expectorate sputum for diagnostic testing. BMC Infectious Diseases. 2015; 15(262). https://doi.org/10.1186/s12879-015-0967-z
- Tessema, T.A., Hamasur, B., Bjune, G., Svenson, S. and Bjorvatn, B. Diagnostic evaluation of urinary lipoarabinomannan at an Ethiopian Tuberculosis Centre. Scandinavian Journal of Infectious Diseases. 2001; 33(4): 279-284. DOI:10.1080/003655401300077306
- Huerger,H., Rucker, S.C.M., Bastard, M., Dimba, A., Kamba, C., Amoros, I. et al. Should urine-LAM tests be used in TB symptomatic HIV-positive patients when no CD4 count is available? A prospective observational cohort study from Malawi. JAIDS. 2020; 83(1): 24-30.
- Broger, T., Nicol, M.P., Sigal, G.B., Gotuzzo, E., Zimmer, A.J., Surtie, S. et al. Diagnostic accuracy of 3 urine lipoarabinomannan tuberculosis assays in HIV-negative outpatients. J Clin Invest. 2020; 130(11): 5756-5764.
- Drain, P.K., Losina, E., Coleman, S.M., Giddy, J., Ross, D., Katz, J.N. et al. Value of urine lipoarabinomannan grade and second test for optimizing clinic-based screening for HIV-adsociated pulmonary tuberculosis. JAIDS. 2015; 68(3): 274-280.
- Drain, P.K., Gounder, .L, Grobler, A., Sahid, F., Bassett, I.V. and Mshomed-Yunue, S.M. Urine lipoarabinomannan to monitor antituberculosis therapy response and predict mortality in an HIV- endemic region: a prospective cohort study. BMJ Open. 2015; 5(4): e006833. doi : 10.1136/bmjopen-2014-006833.
Medical Journal of Zambia, Vol 50, 1
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.