Factors associated with successful In-Vitro Fertilization Treatment at Lusaka IVF and Fertility Clinic in Zambia
Mazuba Makamo
Department of Obstetrics and Gynecology, School of Medicine, University of Zambia, Lusaka, Zambia
Lusaka IVF and Fertility Clinic, Lusaka, Zambia
Nalule Muyinza Flavia
Department of Epidemiology and Biostatistics, School of Public Health, University of Zambia, Lusaka, Zambia
Lusaka IVF and Fertility Clinic, Lusaka, Zambia
Sali Edward Tamale
Lusaka IVF and Fertility Clinic, Lusaka, Zambia
Bellington Vwalika
Department of Obstetrics and Gynecology, School of Medicine, University of Zambia, Lusaka, Zambia
DOI: https://doi.org/10.55320/mjz.50.2.372
Keywords:In-vitro Fertilization, Factors, Embryo transfer, Age
ABSTRACT
Background: The considerable emotional, physical and financial burden associated with infertility and its treatment in general, demands that factors strongly associated with the outcome should be identified and regulated prior to embryo transfer. This will improve the outcome of IVF and provide a patient centered approach to treatment.
Methods: This was a cross sectional study at the Lusaka IVF and fertility clinic. The study aimed to identify factors associated with successful IVF treatment. 414 women had undergone IVF treatment and were eligible. The data was collected from patients’ files and entered in excel then exported to Stata V13.1.for analysis. The participant’s characteristics were compared using the Chi square. The success rate was calculated and associations measured using univariate and multivariate logistic regression.
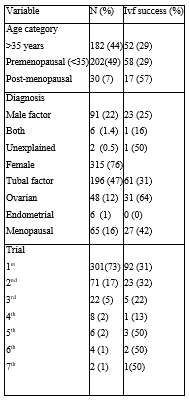
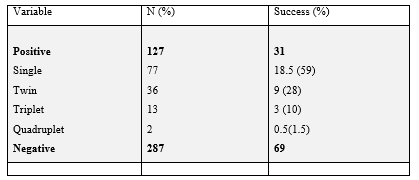
Results: The success rate of IVF treatment was 31% in the study period. Factors associated with successful IVF treatment include age, number of embryos transferred and the sperm factor. These were statistically significant. It was noted that post-menopausal women were 3 times more likely to have a successful IVF than those less than 35 years.
Conclusion: The success rate of IVF treatment at LIVF clinic was 31%. The factors associated with successful IVF treatment were age of the woman, order of embryos transferred and use of donor sperm. There is need to engage the law makers to come up with a legal framework that will guide on the handling of gametes which will include sperm and oocyte donation and receiving, freezing, transportation and surrogacy.
INTRODUCTION
Infertility remains a big problem in the global burden of disease. Couples and individuals who desire but are unable to achieve and maintain a pregnancy, have needs which are not being addressed, especially in low resource settings worldwide. The global infertility prevalence rates are difficult to determine because of the presence of both male and female factors. This complicates the estimate which may only address the woman and an outcome of pregnancy diagnosis of live births.[1] In Zambia, it was reported that secondary infertility was more prevalent than primary infertility. Furthermore, pelvic surgery and other procedures like manual vacuum aspiration were strongly associated with infertility.[2] This estimate warrants worry and therefore demands interventions of assisted reproduction such as in-vitro fertilization (IVF).
Many couples with infertility seek assisted reproductive techniques such as IVF to assist in achieving pregnancy. IVF is a procedure by which oocytes are collected from the ovaries and co-incubated with sperm. The resulting embryos are then transferred into the uterus trans-vaginally to achieve a pregnancy. This procedure does not guarantee a successful pregnancy or live birth. Several factors associated with its success have been postulated and used to improve the outcomes. These factors include; cause of infertility, previous pelvic surgery, number of embryos transferred, additional procedures like ICSI, number of IVF cycles attempted, use of donor eggs and whether frozen or fresh embryos were used. These factors have been investigated in other regions but southern Africa. In 2003, the IVF-associated live birth rates after the transfer of fresh and frozen-thawed non-donor embryos in the United States were 34.7% and 27%, respectively.[3]
With regards to assisted reproductive therapy, the first IVF Center, the Lusaka IVF and fertility clinic was opened in 2015. There has been no study to evaluate factors associated with successful IVF treatment in Zambia since the inception of its first and only IVF clinic. The cost burden and uncertainty of IVF treatment outcome does not make the decision to pursue the treatment any easier. Therefore, IVF treatment demands for individual characterization that would predict success of the treatment The aim of this study was to determine the success rate and factors associated with successful IVF treatment at the facility. These factors will be used to predict the success in individuals and treat correctable factors before undertaking the procedure thus reducing the emotional stress, psychological impact and financial burden associated with a failed IVF treatment.
METHODS
Study design
This was a retrospective cross-sectional study that looked at all the patients that had undergone IVF treatment between October 2015 and December 2018 at LIVF in Zambia. The study investigated demographic and clinical factors associated with a successful IVF treatment during this period. Patients with a successful treatment were characterized and compared with those that were not. Factors associated with a successful treatment were compared in the two groups.
Study site
The study site was Lusaka IVF and fertility clinic in Zambia. This is the first ever IVF center in Zambia. It started operations in 2015 and had its first IVF cycle in October 2015. It is located in Lusaka’s woodlands area, off independence avenue along Ngulube road. The source of data was in the clinic’s patients record room where the files are kept.
Sample selection
Inclusion
All patients that had undergone IVF treatment at the center between October 2015 and December 2018 and without missing data in the records relevant to the study.
Exclusion
Patients who had done IVF from other centers worldwide and came through the clinic for follow up and those whose outcome was not known to the clinic records.
Sample size
Total sampling was done and the sample size came to 414 participants. This was the total number of participants that met the inclusion criteria.
Data collection and analysis
The data was collected between 9th May, 2020 and 10th December, 2020 from the files of all the patients that had undergone IVF treatment. The exposure in this study was IVF treatment and embryo transfer and the outcome a successful delivery of a live baby or babies. The factors associated with the desired outcome were analysed using Stata version 13.1.
The desired variables were entered into excel from the files and then exported to Stata version 13.1 for analysis. The independent variables included; age, duration and cause of infertility, the number of IVF cycles attempted, number of embryos transferred, the day of embryo transfer, fresh or frozen embryo, whether donor gametes were used or own gametes, additional procedure such as ICSI or not, co-morbidities such as Hypertension or HIV. The outcome variable was a live baby or babies delivered following IVF treatment. This information was collected from the patients records in the hospital file by the PI and entered into Excel Microsoft office. The data was cleaned and then exported to Stata version 13.1. Patients were grouped by whether they had a successful treatment or not in the study period and characteristics were compared using the Wilcoxon rank sum test for continuous variables and the Chi-square or Fisher's exact test for categorical variables, as appropriate. The success rate was calculated from Stata. Associations between a successful IVF treatment and the stated independent variables were assessed using Logistic regression in Stata.
Data stotage
The data is stored in a hard drive and another memory disc accessed only to the PI. This data set has no names of patients or numbers that may identify the patient. However, there are unique identification numbers specific to the study that do not identify the patient. Upon entry of the data in the data set, the files were returned to the store room shelves in the clinic records room. The data entry was done at the clinic, outside the working hours of the clinic.
Ethical concerns
The data in the study is anonymous and there are no identification numbers to link a patient to the data base. There was no direct benefit for the participants in this study, but the knowledge generated from this study is intended to improve the care and approach of patients undergoing IVF treatment in Zambia. There were no procedures in the study that caused direct harm to the participants as only records of what was already done were used.
Permission to conduct the study was sought from the Lusaka IVF and fertility clinic management and they allowed without reservation on 24th July 2019. Ethical clearance was sought from the University of Zambia Biomedical Research Ethics Committee (UNZABREC) and the study was approved by the ethics committee on 23 October 2019. Authority to conduct the study was granted by the Zambian National health research authority on 11thNovember 2019.
Patient and Public Involvement
The process of conception through IVF is psychologically, emotionally, physiologically and socially stressful. IVF treatment is being offered in Zambia and the success rate is estimated around 30% to 60%. Factors associated with this success are adopted from an environment different from Zambia. However, in this setting we have no studies to suggest factors associated with success of IVF treatment. In the interest of the patients, it is important to know the factors associated with a successful IVF treatment as this would help to handle the problems that may hinder the outcome before embarking on the treatment. Patients were not directly involved/recruited in this study however secondary data from patients’ clinical records was used. A copy of study findings will be shared with the Lusaka IVF and fertility clinic.
RESULTS
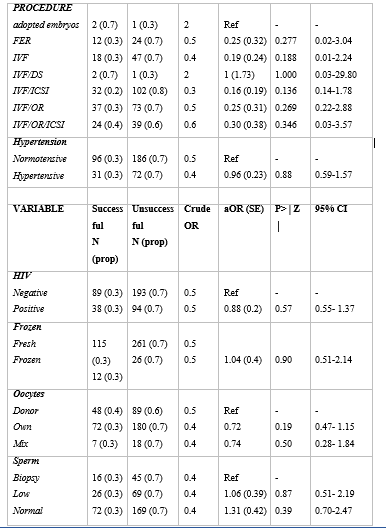
The table below outlines the logistic regression in the respective categories of the variables under investigation. It is observed that age, number of embryos transferred and donor sperm were significant at 95% Confidence interval.

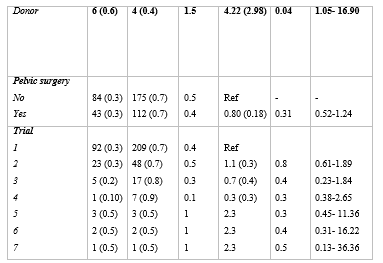
The table above shows that post-menopausal women were 3 times more likely to have a successful treatment than those that were premenopausal. It is also observed that the higher order the number of embryos transferred the higher the chances of a successful treatment. Women that had 3, 5, 7 embryos transferred were 5, 7, 9 times more likely to be successful than those that had a single embryo transfer (SET). It was however beyond the scope of this study to determine multiple gestation association with higher order embryo transfer.
The table below attempts to create a model based on the variables that were significant in the multivariate regression, to determine any confounding as well as develop a model of the factors that would predict successful IVF.

In this model we note that being post-menopausal and consequently using donor oocytes with increased order of embryo transfer is associated with a successful treatment. Post-menopausal women were about 3 times more likely to conceive and deliver a baby than premenopausal women who used their own oocytes.
The number of embryos transferred was significant and it was observed that the higher the order of embryo transfer the higher the odds of a successful treatment. It is observed that with 3, 5 and 7 embryos transferred the odds of success compared with SET was 5, 7 and 9. In the other order of embryo transfer, the number was likely so small that the results were not significant at 95% CI.
The male factor infertility was more likely to be successful if a donor sperm was used than if a biopsy or poor sperm quality was used. The results were however not significant after the multivariate analysis.
Other factors investigated were insignificant at 95% CI. However, we can draw from the trends in the values and guide to future studies that are bigger with larger sample size over a longer period of study.
DISCUSSION
The factors that were associated with successful IVF treatment in Zambia were; age of the woman, number of embryos transferred per cycle and sperm factor. Other factors investigated included; type and additional treatment on IVF, day of embryo transfer, whether fresh or frozen embryos, number of trials of IVF, communicable disease, HIV, non-communicable disease, hypertension, history of pelvic surgery prior to IVF treatment. The success rate of IVF treatment between October 2015 and December 2018 was 31%.
Success rate
An analysis by the ESHRE, European IVF monitoring consortium in 2016 showed that pregnancy rates per treatment started were 27.1% with IVF and 24.3 with ICSI.[4] The latest efficiencies reported by the American and European societies of reproduction and fertility are around 37% of pregnancies and 25% of deliveries per embryo transfer.[5] There is limited published data on the success in African countries and this is a milestone in knowledge as a guide to the success rate. Thirty one percent (31%) is comparably a good statistic for a developing nation like Zambia.
Age and IVF Success
In this study, the youngest client was 23 years old while the oldest was 56 years. The mean age of participants was 36 years. It was noted that the odds of success of IVF treatment was higher in post-menopausal women than those in their reproductive age. Post-menopausal women were 3 times more likely to have a successful treatment than women undergoing the same treatment that were premenopausal. This is contrary to what was found by[6] , who reported that age above 35 years was associated with lower success of pregnancy rate per ET compared to those below 35 years. The effect of advancing age on in-vitro fertilization (IVF) is demonstrated not only in ovarian response to ovulation stimulation, but also in reduced implantation efficiency. The advancement in IVF has seen the use of donated oocytes for women that are unable to produce their own eggs or produce poor quality eggs. This includes women with premature ovarian failure, poor response to ovulation induction drugs as well as menopausal women. Therefore, women with a poor prognosis for successful IVF with use of their own eggs are advised to consider donor oocyte procedure which has shown an increased likelihood of successful treatment. This may be the reason why there was a difference in the success of the treatment between post-menopausal women and those in their reproductive life. Masbou et al reported that couples that used donor oocytes did better than similar couples that did not.[7] Zambia has 72 different tribes and the cultural diversity is wide. Use of donated embryos however is not a strange phenomenon to the affluent Zambian community but may be a little odd to one who is not adequately exposed. Acceptance to use donor oocytes borders on religious as well as cultural beliefs. It was interesting to note in the study that couples that decided to go ahead with IVF and required donor oocytes, had no problem with use of donor oocytes. It is now upon the Zambian law makers to come up with a law that will guide the use of donated gametes as this is a good option to fertility treatment but needs a legal framework as a guide. In view of this, we may pick a leaf from Article 8 of the European Convention of Human Rights as the ‘right to respect for people’s private and family life’8 where there should be respect for reproductive autonomy. This has its positives and negatives but favors infertility couples that would need donated gametes such as oocytes. Reproductive autonomy is a vital component of human freedom and states that people should be at liberty to choose if, when, and under which circumstances they wish to procreate and raise children. Therefore, use of donated gametes should not be a hinderance for those desiring a child and need this kind of treatment.
It may also be inferred that there are other factors that cause infertility and failure of fertilization than a normally looking oocyte under a microscope. Other inherent characteristics of an oocyte may actually take part in the fertilization and eventually implantation. The donors of embryos are normally women that are above 25 years old and have conceived before. This may be considered around the peak of fertility with likely good outcomes.
There has been a great deal of enquiries on medication or treatment that improve own egg quality and quantity in women with advancing age. So far, there is little information on modalities to improve the ovarian reserve or egg quality in women with poor ovarian reserve due to advancing age. A study by Schwarze et al, evaluated the effects of DHEA treatment in IVF with ICSI and reported that there were better pregnancy outcomes with lower frequency of abortions with use of DHEA, but does not affect the average oocyte retrieval.[9] The mechanism of action of DHEA use maybe improved oocyte quality with improved endometrial receptivity. however, research continues with the goal of developing strategies to improve stimulation response and implantation efficiency in these patients. Some attempts to use germ cells and placental tissue to improve ovarian reserve and oocyte number have been under study, without any reported results so far. Other studies have assumed that ovarian stimulation may affect endometrial receptivity and this may show the difference in conception rates between those that have not received stimulation medication and those that have. However, other studies have shown equivocal results. Advanced maternal age is associated with a decrease in fecundity potential. A decrease in implantation and pregnancy rates are generally seen after the age of 35, and a significant decline after the age of 40 years. With increasing age there is a decline in the ovarian reserve and the quality of embryos produced.[10] Though the CDC report of 2016 noted that the percentage of live births per egg retrieval was 54.4% for women younger than 35 years, this reduced to 42% for women aged 35 to 37 and 26.6% for women 38 years to 40 years. Women aged 41 to 42 was 13. 3 and those 43 and above was 3.9%. This is the case for egg retrieval; however, we saw in this study that the odds were different. Older women were more likely to have a successful treatment as they opted for donor egg. CDC 2016 further reports that the success of IVF using donor eggs is as high as 53.5% with fresh embryos and 38.5% with frozen embryos.[11]
Sperm
Sperm quality during the study period were either normal sperm, low sperm, biopsy or using donor sperm. It was noted that donor sperm had almost 6 times likelihood to get a successful IVF treatment than sperm collected through a biopsy. This could mean that there is more about the genetics of the sperm that influences fertilization and more so implantation than just a normal looking sperm. Donor sperm appeared to be better than own sperm whether normal or low sperm levels. We can investigate genetic factors of the sperm as a cause of infertility in male factor infertility or unexplained infertility. According to the latest reports of the European Society of Human Reproduction and Embryology (ESHRE) and the Centers for Disease Control and Prevention of the United States (CDC), the rate of deliveries per ART cycle in 2014 and 2016 were 21% and 22%, respectively. Among the reasons for this relatively low efficiency, the quality of the spermatozoa has been pointed out as critical, and the presence of high percentages of DNA-damaged spermatozoa in patients’ ejaculates is possibly one of the main factors reducing the ARTs outcomes. Thus, one of the main challenges in reproductive medicine is to ensure the highest quality of the spermatozoa used in ARTs, and specifically, in terms of genetic integrity.[12]
During natural and normal fertilization, ejaculation of sperm into the vagina sends millions of sperm to swim up to the ampulla where fertilization takes place. It is assumed that this subpopulation of sperm that reaches the ampulla for fertilization is selected through the oviduct in a way that only those with highest fertilization capability and the best features for supporting embryo development get the opportunity to fertilize the egg,[13-14] It has thus been proposed that one of the reasons for the relatively low efficiency of ARTs is that we currently lack an effective method of separating this sperm subpopulation for IVF treatment especially for IVF and ICSI.[1] These procedures are presumed to bypass the sperm selection operating in vivo, increasing the risk of fertilizing the oocyte with a defective sperm that could lead to a failed IVF treatment. Furthermore, it is reported that the incidence of sperm abnormalities is higher in infertile men.[13] However, the extent to which the quality of sperm affects ART is not clear.[9] On the other hand it reported no difference in efficiency between ICSI and natural IVF cycle outcomes.
The ICSI technique is now gaining more favor in its use than natural IVF. In developing countries, a reported 71.3% of all ART treatments had ICSI in Europe in 2014 and 72 % in 2016. Herráez et al reported that Using ICSI in patients with severe oligospermia showed reduced blastulation rate, while asthenozoospermia affected the fertilization and cleavage rate following IVF treatment pregnancy rate.[15]
The use of donor sperm in couples needing the treatment has had mixed views. Even though investigating in to the acceptability of gamete donation is beyond the scope of this study, it is worth noting that anecdotally, oocyte donation is more acceptable than sperm donation. Furthermore, donated gametes did better than own gametes in this study.
Number of Embryos transferred
There was an increase in the success of IVF with transfer of more than one embryo. Furthermore, the increase in the order of embryos transferred shows an increasing likelihood of success. These findings are similar to what was found by Hauzman et al.[16] A similar trend was observed by Sharma et al where the pregnancy rate was higher in women with more than one embryo transfer.[17]
Couples and the attending physician often desire to optimize success of the fertility treatment thereby increasing the number of embryos transferred. Furthermore, there is a desire from couples to have multiple gestation and request from the attending physician to transfer more than one embryo. However, the subsequent complications of multiple embryo transfer over the single embryo transfer (SET), is beyond the scope of this study. Some highlights of complications include; preterm delivery and prematurity, risk of complications of multiple pregnancy such Pre-eclampsia, maternal distress and increased risk of operative delivery. SET is preferred in developed nations over double embryo transfer (DET) or multiple embryo transfer. This is also helpful as the embryologist is tasked to look for the best embryo. Similarly, in DET or multiple embryos transfer good embryos are picked and the risk for multiple gestation outweighs the benefit of a successful IVF treatment. In this study however, there was no limitation to the number of embryos transferred and this was based on several factors such as the quality of embryos number of trials of IVF and the desire by the couple or woman for a multiple gestation.
Suffice to say that among the study participants there were few maternal and neonatal complications reported to the clinic.
The American Society of Reproductive Medicine (ASRM), for instance, states that ‘physicians should be encouraged to counsel good-prognosis patients to accept’ SET, and highlights the importance of clinical judgement in selecting the best candidates.[18] Through ASHRM reported that for patients < 35 years of age with a favorable prognosis, ‘providers should only transfer a single embryo, and not more than two embryos’. The Practice Committee of the ASRM, agreed that for patients aged 38-40 years, and 41-42 years, no more than three and five cleavage-stage embryos, respectively, should be transferred. Patients, who have failed two or more IVF cycles or have a less favorable prognosis, can receive an additional embryo. For patients aged over 43, there is no limit to the number of Embryos transferred, according to the Practice Committee of the ASRM and the Practice Committee of the SART, 2013.
In one study, 52% of clinicians were found to deviate from ASHRM’s guidelines concerning embryo transfers due to patients’ requests, 51% deviated when using frozen embryos, and 70% did so when patients had failed prior IVF, and only 34% routinely discussed with all patients SET.[19] In certain developing, as well as in developed countries, most patients prefer transfer of at least two embryos, and providers often comply with these requests.[20]
The Lusaka IVF and fertility clinic also follows guidelines similar to ASHRM, however, other factors such as age of the woman or man, quality of embryos, prior failed IVF and patients request contributes to transfer of more than one embryo.
IVF treatment procedure
Couples undergoing infertility treatment underwent different procedures depending on the diagnosis and outlined plan of management. During the study period, the following procedures were undertaken; natural IVF, IVF with ICSI, IVF with donor oocytes, IVF with donor sperm, IVF with frozen embryo replacement and IVF with adopted embryos. Even though the results were not significant, it is worth noting that each procedure has different loop holes at which failure may be at risk. It takes a good embryologists work, appropriate culture media and strict temperature control for success. An example is the process of ICSI in which identifying normal looking sperm cells and injecting the sperm cells in the ova has many parts that are possible sources of error and resulting failure. The point at which the sperm head is injected and then the tail is cut may offer a degree of failure of the procedure. However, once fertilization is confirmed by the presence of a dividing embryo on day 2, it is assumed that the ICSI procedure is successful. The second reason for reduced pregnancy rates in ICSI would be the likelihood of sperm abnormalities either genetic or not. This in turn would result in first trimester miscarriages and thus an unsuccessful IVF treatment. The sperms obtained by testicular biopsy are picked for fertilization on the basis of normal morphology and a degree of motility. However, there are intrinsic factors about a sperm extracted that may interfere with normal fertilization implantation or growth of the embryo.
Another school of thought has been the culture media to grow embryos after fertilization. Some studies have proposed that culture media has a role on the quality of embryos generated in IVF/ICSI therefore, influencing implantation and pregnancy rates.[21-22] Currently, many culture media are commercially available, each with a different composition. The first culture media in IVF/ICSI were balanced salt solutions to which glucose and phosphate were added. Subsequently, more complex culture media formulations with the addition of non-essential amino acids, chelators (EDTA), vitamins and antibiotics were introduced.[23] Sequential culture media were designed to take into account the changing metabolic needs of the embryo from the cleavage to the blastocyst stage. Culture media studies are beyond the scope of this study but are worth looking into as factors associated with failure or success.
Despite all these changes in culture media, it is still unclear whether the composition of the media affects embryo quality and IVF success rates and which culture medium leads to the best IVF outcome.
Fresh vs Frozen
This study revealed that use of fresh embryos was more likely to yield a successful treatment compared to using frozen embryos. Even though this result is not statistically significant, it gives some insight on the likely outcome in the two groups. This however differs from the findings by Wang et al[24] who reported that implantation and ongoing pregnancy rates were statistically significantly higher in the freeze-only transfer cohort than in the matched fresh transfer cohort and that ongoing pregnancy rate for freeze-only was 52.0% (95% CI, 49.4–54.6) and for fresh was 45.3% (95% CI, 42.7–47.9). Another study by Vuong et al[25] , reported that among infertile women without polycystic ovary syndrome who were undergoing IVF, the transfer of frozen embryos did not result in significantly higher rates of ongoing pregnancy or live birth than the transfer of fresh embryos. It is therefore inconclusive on the difference in the outcomes of success in the two groups.
Day of embryo transfer
It was noted in this study that there was a higher success in IVF treatment when day 5 embryos were used than the day 2 or day 3 embryos. This is similar to what has been found in other studies, even though the results in this study were statistically insignificant OR=1.5 ( P=0.5; at 95%CI 0.42-4.96).
It has been reported that morphologic assessment and grading of day 2 or 3 embryos have limited predictive value for further embryonic development. Some studies have shown that recruitment at the blastocyst stage yields better results than at day 3. Furthermore, pregnancy rates of up to 50% can be acquired by the transfer of blastocysts when compared with embryo transfer at the cleavage stage. The idea behind transfer of blastocyst is the increased chance of getting an advanced embryo with higher chances of implantation and survival. A review of related literature pointed out that day 5 ET with expanded blastocysts had a significantly higher implantation rate than non-expanding or non-cavitating embryos and, thus, single blastocyst transfer might be more successful than Single Embryo Transfer.[26] For instance, about 60% of women who received single blastocyst transfers had at least one excellent quality blastocyst and the pregnancy rate was 40.8% for these patients in a Belgian study.[27] Another study conducted in Saudi Arabia demonstrated that the success of day 5 transfers was a continuum of the number of good quality cleavage stage embryos and the availability of at least one blastocyst for transfer.[28]
Hypertension
Hypertension is a non-communicable disease that affects sight, cardiac function as well as renal function. Its effects on reproduction are not highly investigated. Further, the effect of the medication on reproduction are equally not fully understood. Chronic hypertension can cause poor egg quality; also, many hypertensive women suffer from obesity which is mostly due to excess estrogen production which can lead to infertility.[29] It is thought that the microvascular and macrovascular damage on several organs in the body does not spare those of the genital tract, even when the genital tract is well vascularized. In this study we noted that there was no difference in the outcomes of a live birth in chronic hypertensive and normotensive women. The subsequent development of hypertensive disorders such as pre-eclampsia and eclampsia were not investigated in this study. Similarly, no effect of chronic hypertension on the pregnancy outcomes of a live birth in women undergoing IVF treatment.[30]
HIV
It was reported that longer duration of infection is associated with greater relative fertility reduction for HIV-positive women.[31] The results in this study were however insignificant on the association of HIV infection with successful IVF treatment. In the same light it was thought that HIV would reduce or have no association with failed IVF treatment. This is thought because HIV causes vasculitis and this may affect implantation. Additionally, the effect of the virus maybe the production of natural killer cells or radicals that eventually prevent implantation. The effect of poor egg production may also be at play. The odds of success in this study 1.1 (P= 0.76 at 95% CI 0.63- 1.85). this was statistically insignificant. Coll et al[32] also reported that among HIV-infected patients treated with IVF, the usual reproductive outcome parameters failed to detect any underlying mechanism that could explain the lower pregnancy rate. It would appear that the oocyte of an HIV-infected women begins the IVF process with some further undetectable handicap. It was noted in this study that HIV patients exhibited some level of ovarian resistance as they needed higher doses of ovarian stimulation drugs. This resistance may reflect an underlying sub-clinical (normal menses) and sub-analytical (comparable basal FSH values) hypogonadism. A potential hypothesis might be mitochondrial dysfunction as a result of the use of antiretroviral drugs. However, it was reported that, neither the type of treatment regimen used nor the total duration of HAART were associated with ovarian resistance.[32]
However, the following should be considered while interpreting the abovementioned findings. First, this was a retrospective cross-sectional study, we could not establish causality of failed IVF treatment. Some of the variables had many strata, such as the type or additional procedures to IVF treatment, this made it difficult to have statistically significant results and therefore a larger study population will be needed to determine association in the other variables that had insignificant results at 95%CI. We could only assess factors that were documented on the clinic record, therefore trends and changes in the study period could not be assessed.
The failed IVF due to miscarriage could not be thoroughly investigated as there were no available details of patients that had done Ante natal care (ANC) from other places. Lapses in ANC would have contributed to failed treatment could not be studied due to the study design. Furthermore, a survival analysis would have been used in this case.
The order of number of embryos transferred with associated multiple gestation and the associated success with multiple gestation were not studied. The study design could not allow for this. This would have been a good association to determine whether we should have a limit to the number of embryos transferred in each cycle. It is worth noting that there were no adverse events related to maternal or neonatal morbidity or mortality as far as the clinic was informed.
CONCLUSION
We report a success rate of 31% for IVF treatment at Lusaka IVF and fertility clinic between October 2015 to December 2018. This compares favorably with the success rates recorded in other IVF centers in the world. The factors associated with successful IVF treatment were the age of the woman, number of embryos transferred and use of donor sperms. Post-menopausal women were 3 times more likely to have a successful treatment than premenopausal women undergoing the same treatment and the use of donor oocytes is cited as the likely reason. It was also observed that use of donor sperm had 4 times likelihood for success than use of sperm obtained from a biopsy. There is need to engage the law makers through the Zambia Association of Obstetricians and Gynecologists (ZAGO) to come up with a legal framework that will guide on the handling of gametes which will include sperm and oocyte donation and receiving, freezing and transportation. The law should also guide on surrogacy and any agencies intending to manage such services as the demand for such services is present.
What is already known on this topic - The factors that contribute to the success of IVF treatment in other parts of the world.
What this study adds - Success rate of IVF treatment in the Zambian population is 31% with age and higher order of embryos transferred being a factor.
How this study might affect research, practice or policy - There is need to engage the law makers to come up with a legal framework that will guide on the handling of gametes which will include sperm and oocyte donation and receiving, freezing, transportation and surrogacy.
AUTHOR CONTRIBUTIONS
MM: conceptualization, data curation, formal analysis, investigation, methodology and writing – original draft. FNM: conceptualization, data curation, refinement, and writing- review and editing.BV& SET: overall oversight conceptualization, formal analysis, methodology, supervision and writing- review and editing
ACKNOWLEDGEMENTS
I would like to thank God for the favor he has granted upon me to pursue this study and art of medicine. In the midst of hurdles and difficulties he has made possible what seemed impossible in our humanly eyes. I would like to thank my lecturers from the Department of Obstetrics and Gynecology that have taught me the art to practice with meekness diligence and respect for the patient. I would like to thank not in any order my teachers in this art; Prof B Vwalika my study supervisor, Prof. M Mwanahamuntu, Prof. L Kasonka, Dr. S. N’ganjo, Miss (Dr) Kafula, Dr S. Macha and Dr W Munga that have been very helpful with great insight and meaningful contribution to my practice and the study. I would like to thank my seniors and colleagues in the department for the skills I have learnt. I would like to acknowledge Mr. Steven Aziz who brainstormed and gave good critique and insight to the study. I would like to thank the Zambia National Service for the support rendered during the study. I wish to express gratitude to Lusaka IVF and fertility clinic through Dr Edward T Sali, Prof. Peter Plateau and Dr Gilbert Ahimbisibwe for being so instrumental in the study as well as my studies. I would also like to thank UNZABREC for the guidance on pertinent ethical concerns with the study. Finally, I would like to thank my family for the care, understanding and support during the study.
CONFLICT OF INTEREST
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Abbreviations
AMH: Anti-Mullerian hormone
ART: Assisted reproductive technique
ASHRM: American society for human reproductive medicine
CDC: Center for disease control
DET: Double embryo transfer
DHEA: Dehydroepiandosterone
ET: Embryo transfer
ESHRE: European society of human reproduction and embryology
FSH: Follicle stimulating hormone
FER: Frozen Embryo Replacement
HFRA: Human fertilization reproduction authority
LH: Luteinizing hormone
LIVF: Lusaka IVF and fertility clinic
IVF: In-vitro fertilization
ICSI: Intra cytoplasmic sperm injection
PCOS: Polycystic ovarian syndrome
SART: Society for Assisted Reproductive Technology
SET: Single Embryo Transfer
TESA: Testicular sperm aspiration
WHO: World Health Organization
UNZABREC: University of Zambia Biomedical Research Ethics Committee
Definition of terms
Oocyte - Female gamete
Sperm - Male gamete
Embryo -The result of fusion of the male and female gamete
In-vitro fertilization - The fertilization of an egg by a sperm outside the human body (oviducts)
Infertility - Failure to conceive after 1 year of uninterrupted penile-vaginal sexual intercourse
Primary infertility - Infertility in a person who has never conceived.
Secondary infertility - Infertility in a person that has conceived before.
Premenopausal - The period in a womans life immediately preceding menopause.
Postmenopausal - The period in a womans life after menopause.
Clinical pregnancy - Positive quantitative pregnancy test 2 weeks following embryo transfer.
Successful IVF - Pregnancy outcome of a live birth(s) following IVF treatment.
REFERENCES
- Mascarenhas MN, Flaxman SR, Boerma T, Vanderpoel S, Stevens GA. National, regional, and global trends in infertility prevalence since 1990: a systematic analysis of 277 health surveys. PLoS Med. 2012; 9(12):e1001356.
- Kalima-Munalula MN, Ahmed Y, Vwalika B. Factors associated with infertility among women attending the gynaecology clinic at University Teaching Hospital, Lusaka, Zambia. Med J Zambia. 2017;44(1):41–4.
- York N. Infertility therapy-associated multiple pregnancies (births): an ongoing epidemic. 2003;
- Consortium (EIM) EIM, Reproduction ES of H, Embryology (ESHRE), Kupka MS, D’Hooghe T, Ferraretti AP, et al. Assisted reproductive technology in Europe, 2011: results generated from European registers by ESHRE. Hum Reprod. 2016;31(2):233–48.
- De Geyter C, Calhaz-Jorge C, Kupka MS, Wyns C, Mocanu E, Motrenko T, et al. ART in Europe, 2014: results generated from European registries by ESHRE: The European IVF-monitoring Consortium (EIM) for the European Society of Human Reproduction and Embryology (ESHRE). Hum Reprod. 2018;33(9):1586–601.
- Preutthipan S, Amso N, Curtis P, Shaw RW. Effect of maternal age on clinical outcome in women undergoing in vitro fertilization and embryo transfer (IVF-ET). J Med Assoc Thail Chotmaihet Thangphaet. 1996;79(6):347–52.
- Masbou AK, Friedenthal JB, McCulloh DH, McCaffrey C, Fino ME, Grifo JA, et al. A comparison of pregnancy outcomes in patients undergoing donor egg single embryo transfers with and without preimplantation genetic testing. Reprod Sci. 2019; 26(12):1661–5.
- Ellis K. Promoting rights or avoiding litigation? The introduction of the Human Rights Act 1998 into adult social care in England. Eur J Soc Work. 2004;7(3):321–40.
- Schwarze JE, Canales J, Crosby J, Ortega-Hrepich C, Villa S, Pommer R. DHEA Use to Improve Likelihood of IVF/ICSI Success in Patients With Diminished Ovarian Reserve: A Systematic Review and Meta-analysis. Obstet Gynecol Surv. 2019;74(9):535–6.
- Munné S, Alikani M, Ribustello L, Colls P, Martínez-Ortiz PA, Group RP, et al. Euploidy rates in donor egg cycles significantly differ between fertility centers. Hum Reprod. 2017;32(4):743–9.
- Sunderam S, Kissin DM, Zhang Y, Folger SG, Boulet SL, Warner L, et al. Assisted reproductive technology surveillance—United States, 2016. MMWR Surveill Summ. 2019;68(4):1.
- Ioannou D, Fortun J, Tempest HG. Meiotic nondisjunction and sperm aneuploidy in humans. Reproduction. 2019;157(1):R15–31.
- Kushnir VA, Safdie M, Darmon SK, Albertini DF, Barad DH, Gleicher N. Age-specific IVF outcomes in infertile women with baseline FSH levels≥ 20 mIU/mL. Reprod Sci. 2018; 25(6):893–8.
- Fang Y, Wu R, Lee JM, Chan LHM, Chan KYJ. Microfluidic in-vitro fertilization technologies: Transforming the future of human reproduction. TrAC Trends Anal Chem . 2023; 116959.
- áez MP, Ausió J, Devaux A, González-Rojo S, Fernández-Díez C, Bony S, et al. Paternal contribution to development: sperm genetic damage and repair in fish. Aquaculture. 2017;472:45–59.
- man EE, Garcia-Velasco JA, Pellicer A. Oocyte donation and endometriosis: what are the lessons? In: Seminars in reproductive medicine. Thieme Medical Publishers; 2013. p. 173–7.
- Sharma V, Allgar V, Rajkhowa M. Factors influencing the cumulative conception rate and discontinuation of in vitro fertilization treatment for infertility. Fertil Steril. 2002;78(1):40–6.
- Allyse M, Amer H, Coutifaris C, Falcone T, Famuyide A, Flyckt R, et al. American Society for Reproductive Medicine position statement on uterus transplantation: a committee opinion. Fertil Steril. 2018;110(4):605–10.
- Jungheim ES, Ryan GL, Levens ED, Cunningham AF, Macones GA, Carson KR, et al. Embryo transfer practices in the United States: a survey of clinics registered with the Society for Assisted Reproductive Technology. Fertil Steril. 2010;94(4):1432–6.
- Balasubramanyam S. Knowledge and attitudes of women towards multiple embryo transfer, fetal reduction and multiple pregnancy. Int J Infertil Fetal Med. 2010; 1:31–4.
- Mantikou E, Youssef MA, van Wely M, van der Veen F, Al-Inany HG, Repping S, et al. Embryo culture media and IVF/ICSI success rates: a systematic review. Hum Reprod Update. 2013;19(3):210–20.
- Zegers-Hochschild F, Schwarze JE. The Chilean experience: Cultural and political factors shaping human embryo assessment during IVF. In: Human Embryos and Preimplantation Genetic Technologies. Elsevier; 2019. p. 127–33.
- Gardner DK, Schoolcraft WB. Culture and transfer of human blastocysts. Curr Opin Obstet Gynecol. 1999; 11(3):307–11.
- Wang A, Santistevan A, Cohn KH, Copperman A, Nulsen J, Miller BT, et al. Freeze-only versus fresh embryo transfer in a multicenter matched cohort study: contribution of progesterone and maternal age to success rates. Fertil Steril. 2017;108(2):254–61.
- LN, Dang VQ, Ho TM, Huynh BG, Ha DT, Pham TD, et al. IVF transfer of fresh or frozen embryos in women without polycystic ovaries. N Engl J Med. 2018; 378 (2):137–47.
- Rienzi L, Ubaldi F, Iacobelli M, Ferrero S, Minasi MG, Martinez F, et al. Day 3 embryo transfer with combined evaluation at the pronuclear and cleavage stages compares favourably with day 5 blastocyst transfer. Hum Reprod. 2002;17(7):1852–5.
- Blank C, Wildeboer RR, DeCroo I, Tilleman K, Weyers B, De Sutter P, et al. Prediction of implantation after blastocyst transfer in in vitro fertilization: a machine-learning perspective. Fertil Steril. 2019;111(2):318–26.
- Alfaraj S, Alzaher F, Alshwaiaer S, Ahmed A. Pregnancy outcome of day 3 versus day 5 embryo transfer: a retrospective analysis. Asian Pac J Reprod. 2017;6(2):89.
- Farland LV, Grodstein F, Srouji SS, Forman JP, Rich-Edwards J, Chavarro JE, et al. Infertility, fertility treatment, and risk of hypertension. Fertil Steril. 2015;104(2):391–7.
- Dayan N, Lanes A, Walker MC, Spitzer KA, Laskin CA. Effect of chronic hypertension on assisted pregnancy outcomes: a population-based study in Ontario, Canada. Fertil Steril. 2016;105(4):1003–9.
- Marston M, Zaba B, Eaton JW. Relative patterns of sexual activity and fertility among HIV positive and negative women—evidence from 46 DHS. PLoS One. 2018;13(10):e0204584.
- Coll O, Suy A, Figueras F, Vernaeve V, Martínez E, Mataró D, et al. Decreased pregnancy rate after in-vitro fertilization in HIV-infected women receiving HAART. Aids. 2006;20(1):121–3.
Medical Journal of Zambia, Vol 50, 2
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.