Assessment of Antibiotic Resistance Patterns of Bacterial Pathogens Isolated from Blood Culture Specimens at Livingstone University Teaching Hospital in Zambia
Thresa N. Mwansa
Mulungushi University School of Medicine and Health Sciences, Department of Pathology and Microbiology, Livingstone Zambia
John Amos Mulemena
Mulungushi University School of Medicine and Health Sciences, Department of Pathology and Microbiology, Livingstone Zambia
Warren Chanda
Mulungushi University School of Medicine and Health Sciences, Department of Pathology and Microbiology, Livingstone Zambia
DOI: https://doi.org/10.55320/mjz.49.3.360
Keywords:Antibiotic resistance, Blood stream infections, Imipenem, Escherichia coliLivingstone University Teaching Hospital
ABSTRACT
Background. Bloodstream infections (BSI) are of public health concern because they are usually associated with high fatality rate if therapy is delayed. A combination of these infections with antibiotic resistance increases healthcare costs. In this study, microorganisms identified from blood cultures at Livingstone University Teaching Hospital (LUTH) between 2019 and 2021 were evaluated for their antibiotic resistance patterns.
Methods. This was a single-centre laboratory based retrospective study. Data on isolated organisms from electronic laboratory system generated reports at LUTH microbiology laboratory for a period of 3 years, was analysed with SPSS version 20.
Results. A total of 765 specimens were processed and only 331 (43.3%) met the inclusion criteria. Of the 331 specimens, 61.3% and 38.7% were collected from female and male patients, respectively whereas 65.9% came from out-patient departments and 34.1% from in-patient departments. The commonest bacteria isolate was Escherichia coli (27.2%) followed by Enterobacter agglomerans (22.7%), Klebsiella pneumoniae (13%), Klebsiella oxytoca (6.3%), Enterobacter aerogenes (5.4%), Enterobacter cloacae (5.4%), Citrobacter freundii (4.8%), Serratia marcescens (3.6%), Proteus mirabilis (3.3%), and Staphylococcus aureus (2.7%). Of the common utilized antibiotics, ampicillin (92.9%) was the least effective drug followed by co-trimoxazole (82.7%), nalidixic acid (68.3%), penicillin (66.7%), tetracycline (63.5%), and chloramphenicol (50.3%), while imipenem (15.4%), norfloxacin (35.3%), and nitrofurantoin (38.8%) were the most effective. The patient's gender and hospital location may have an impact on antibiotic resistance.
Conclusion. The most common bacterial pathogens were Gram-negative Enterobacteriaceae that showed increased resistance to various classes of commonly used antibiotics at LUTH but with low resistance to imipenem. Due to the observed multidrug resistant pathogens for BSI, it is cardinal for healthcare facilities to monitor bacteria resistance patterns regularly and encourage the prudent use of antibiotics. However, antibiotic selection for susceptibility testing should be based on the Clinical and Laboratory Standards Institute (CLSI) and Zambia National Formulary (ZNF) recommendations to only test antibiotics1r for BSI instead of those recommended for other infections like urinary tract infections (e.g., tetracyclines).
INTRODUCTION
Bloodstream infections (BSI) are infectious diseases recognized by the presence of viable microorganisms in the bloodstream [1] . Globally, BSI are a major public health burden with high mortality as the infections account for 10-20% of all nosocomial infections and are the eighth leading cause of mortality (15%) in the United States [2-4] . In BSI, patient outcome is critically influenced by delayed therapy, and fast and accurate pathogen diagnostics decisively improves the care of patients [4] . Moreover, the mainstay of therapy for patients with bacteraemia remains antimicrobial therapy, together with the optimal management of its consequences (e.g., shock or metastatic suppurative complications), and surgical treatment of an infection site (e.g., debridement, abscess drainage, or removal of intravascular devices), when appropriate [5] . Thus, early adequate treatment is key and should use available guidelines and direct examination of samples should be performed from the infectious source to clearly identify the causative agent. The mechanism of quick identification of pathogens (like automated blood culture systems) and their susceptibility patterns in patients with bacteraemia is lacking in many healthcare facilities. Few healthcare facilities especially those in urban areas use the traditional method of blood culture bottles that are usually incubated for a number of days (before declaring them negative) with daily subcultures on solid media that subsequently increase the chances of false positives due to possible contamination [6] . Because of this, broad spectrum antibiotics are liberally and mostly unnecessarily used resulting into an increase in emerging resistance and when combined with poor infection control practices, resistant bacteria can easily be disseminated to other patients and the environment [7] .
Antimicrobial resistance (AMR) is another major public health concern, worldwide. In low and medium-income countries (LMIC), AMR monitoring is inadequate, but the extensive usage of antibiotics to prevent and treat infectious diseases has led to the emergence and spread of antibiotic resistance which has influenced a particular force on susceptible bacteria leading to resistant strain survival, consequently increasing medical costs, illness, and mortality [8] . Therefore, surveillance of bloodstream infections from blood cultures and their antibiotic resistance patterns are vital to the care of patients and prevention of BSI [2] . Studies have shown increased prevalence of extended spectrum beta lactamase (ESBL) producing strains and carbapenem resistance strains among blood pathogens [8-10] .
In Zambia, several reports have indicated the presence of antibiotic resistant bacterial pathogens [11-15] , and more recently, a spike in resistance to imipenem, ciprofloxacin and ampicillin by Escherichia coli, Klebsiella pneumoniae, Proteus mirabilis and Proteus species from blood and other specimen sources has been observed [16] . Despite these reports, irrational use of antibiotics is widely practiced and lack of control policies on over-the-counter antibiotics may increase emergence of multidrug resistant (MDR) strains. To circumvent the MDR issue at the hospital level, monitoring of the pathogenic spectrum and changes in bacterial antibiotic resistance help in effective clinical therapy and infection control [17] . Therefore, our study aimed at understanding the resistance patterns of pathogens isolated from blood cultures at Livingstone University Teaching Hospital (LUTH).
METHODS
Study design and site. A single-centre laboratory based retrospective study was conducted at Livingstone University Teaching Hospital (LUTH) on routine specimen isolates from patients who visited the hospital between January 2019 and December 2021. The cultures of patient blood specimens, identification of bacterial isolates and antimicrobial susceptibility testing were conducted on commercially and in-house prepared media that were quality controlled with the American Type Culture Collection (ATCC) standard strains following the Clinical and Laboratory Standards Institute (CLSI) recommendations [18] . The LUTH microbiology laboratory participates in a bacteriology External Quality Assessment (EQA) program and has been accredited by the Southern African Development Community Accreditation Service (SADCAS).
Eligibility criteria. This study included all blood specimens having information on the patient’s gender, age, location (ward/clinic), name of organism and antibiotic susceptibility testing. However, any blood isolated organism without a species name, and with unknown source (i.e., lack of age-, location-, and gender of patient) were excluded from the study.
Data collection and analysis. Data from a Disa*Lab system generated reports on all isolated bacteria from blood specimens at LUTH microbiology laboratory for a period of 3 years (January 2019 to December 2021) was used from which information such as age, gender, patient’s location, name of the bacterium and the antibiotic susceptibility were considered. The collected data was entered, assorted, and coded using Microsoft Excel 365 and then exported to IBM Statistical Package for Social Science (SPSS) version 20 for analysis. Descriptive statistics was used to describe the data. Microsoft Excel 365 was used for graph generation and a chi-square test was used for categorical variables. A p-value of ≤0.05 was considered statistically significant.
Ethical consideration. The ethical clearance was obtained from Mulungushi University School of Medicine and Health Sciences Research Ethics Committee (reference no.: SMHS-MU2-2021-33v1) while permission to use the Disa*Lab system generated data was obtained from Livingstone University Teaching Hospital management. No personal identifiers were included in the study.
RESULTS
Characterization of bacterial organisms isolated from blood specimens
A total of 765 specimens were processed from January 2019 to December 2021 and only 331 (43.3%) met the inclusion criteria for this study. Of the 331 eligible blood specimens, the variations in the number of processed specimens are presented in Figure 1. Briefly, more specimens were processed from females (61.3%) than males (38.7%). Furthermore, it was observed that the number of specimens processed in the year 2020 was higher than specimens processed in the years 2019 and 2021. Patients from the age group 17- to 39-year-old had more blood specimens than those from 0 to 16 years old or 40 to 80 years old. Lastly, there was more blood specimens from the out-patient departments (OPD) than the in-patient departments (IPD). Amongst the bacteria isolates identified, gram-negative strains were the majority with the top five being Escherichia coli (E. coli; 90, 27.2%), Enterobacter agglomerans (E. agglomerans; 75, 22.7%), Klebsiella pneumoniae (K. pneumoniae; 43, 13%), Klebsiella oxytoca (K. oxytoca; 21, 6.3%), and Enterobacter aerogenes (E. aerogenes; 19, 5.4%), as presented in Figure 2.
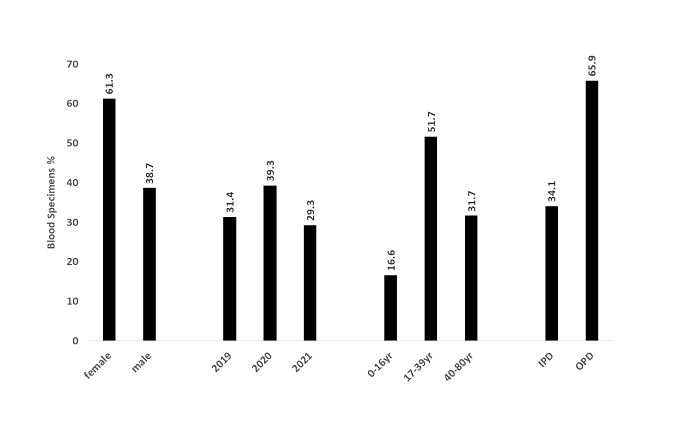
Figure 1: The processed blood specimens based on patient gender, year, patient age group and patient location. The numbers represent percentage frequencies of specimens. IPD: in-patient departments, OPD: out-patient departments, yr: year.
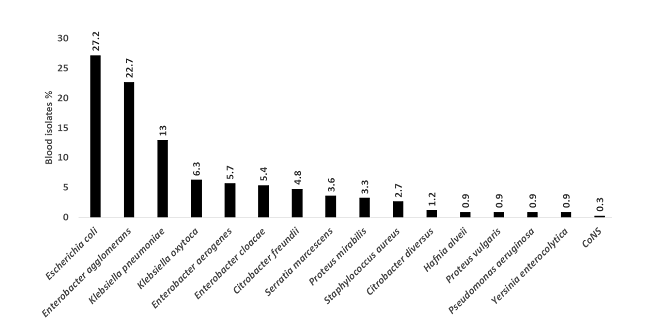
Figure 2: Bacteria isolates from blood specimens. The numbers indicate percentage frequencies of the isolate. CoNS: Coagulase negative Staphylococci.
Assessment of susceptibility pattern of blood isolates Antibiotic
susceptibility testing was conducted with a panel of antibiotics that are commonly used at LUTH. The resistance percentage of used antibiotics showed ampicillin (92.9%) as the least effective drug followed by co-trimoxazole (82.7%), nalidixic acid (68.3%), penicillin (66.7%), tetracycline (63.5%), and chloramphenicol (50.3%) whereas the most effective antibiotics were imipenem (15.4%), norfloxacin (35.3%) and nitrofurantoin (38.8%) as shown in Figure 3.
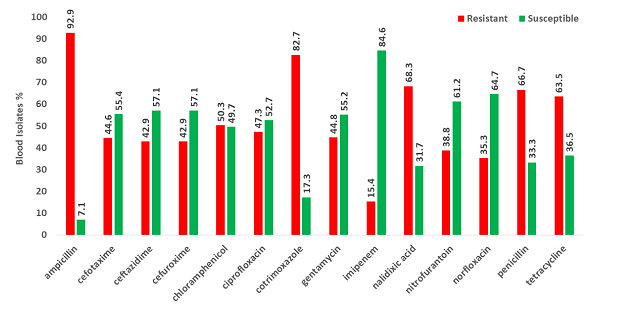
Figure 3: Susceptibility pattern of blood isolates on commonly used antibiotics at LUTH. Percentage frequencies are shown.
The association of independent study variables with antibiotic resistance
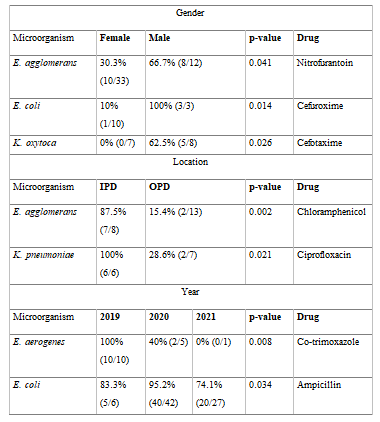
In trying to understand the association of independent variables with antibiotic resistance, a chi-square test was conducted. Table 1 shows the resistant pattern of some blood isolated bacteria with respect to patient gender, patient location, and year of isolation. The authors observed high levels of E. agglomerans resistance to nitrofurantoin (p-value = 0.041) E. coli resistance to cefuroxime (p-value = 0.014), K. oxytoca resistance to cefuroxime (p-value = 0.026) in males compared to females. This is in part due to the differences in the numbers of isolates tested between males and females. Furthermore, patient location (IPD vs OPD) had a negative effect on chloramphenicol and ciprofloxacin. E. agglomerans and K. pneumoniae isolates from IPD were resistant to chloramphenicol (p=0.002) and ciprofloxacin (p=0.021) whereas the resistance of E. aerogenes to co-trimoxazole (p=0.008) and E. coli to ampicillin (p=0.034) varied on the year the bacteria were isolated (Table 1). These resistance variations could be in part due to the differences in the numbers of isolates tested between IPD vs OPD and years of isolation (2019 vs 2020 vs 2021), respectively.
Table 1: The resistant pattern of some blood isolated bacteria with respect to patient gender, patient location, and year of isolation.
DISCUSSION
Bacteraemia is the presence of viable bacteria in the circulatory system that may result from an existing focus of infection, a site with commensal flora or direct inoculation of contaminants via a trauma. According to this study, the majority of bacteraemia cases at LUTH involved female patients (61.3%) and were acquired in the community because the OPD saw the greatest rates of infections (65.9%). Additionally, there were more bacteraemia cases in patients aged 17 to 80 years than in children (0-16years) but this study could not establish whether getting older was a risk factor for BSI because of the wider range of age intervals. Elsewhere, Laupland et al.[19] , found that older age and male patients were at higher risk of developing BSI. Future studies should consider assessing age as continuous variable in establishing whether older age may be a risk factor for BSI. However, the current study found more female patients (61.3%) with bacteriemia cases than male patients (38.7%) and was not in agreement with Laupland et al.’s study findings. This discrepancy might be because of the variation in study population, study design and the numbers of antibiotic-exposed isolates. The results of a different retrospective study conducted in the United States by Page et al. [20] that found more cases of community-acquired severe sepsis than healthcare-associated severe sepsis and hospital-acquired severe sepsis agreed with the current study findings of more community-acquired BSI. The presence of bacteria in blood has long been regarded as a sign of infection since human blood has generally been thought of as a completely sterile environment consisting only of blood cells, platelets, and plasma [21] . Although the possibility of a healthy human blood microbiome is a contested idea that calls for additional research, the current study does not address the question of whether microbial cells or cell-free microbial DNA may be detected in healthy human blood [21, 22] . Considering the idea that human blood is a sterile environment, any bacterial isolate was therefore considered as a potential blood pathogen in our investigation. As a result, E. coli (27.2%), E. agglomerans (22.7%), K. pneumoniae (13%), K. oxytoca (6.3%), E. aerogenes (5.7%), E. cloacae (5.4%), C. freundii (4.7%), S. marcescens (3.6%), P. mirabilis (3.3%), and S. aureus (2.7%) were the most frequently found blood pathogens at LUTH. Similar study results showed that E. coli was the most frequent cause of bacteraemia [23] and that Enterobacteriaceae, Coagulase-negative Staphylococci and S. aureus predominated blood infections in HIV-positive individuals [24] .
Additionally, our susceptibility study found that LUTH had the highest proportion of resistant bacteria that had 63.5% to 92.9% resistance to ampicillin, tetracycline, co-trimoxazole, nalidixic acid, and penicillin. Studies have reported an increased trend of BSI caused by methicillin-resistant S. aureus (MRSA) and third-generation cephalosporin-resistant E. coli which subsequently exert pressure on prolonged hospital stay thereby increasing the healthcare costs [25] . High concentrations of gram-negative bacteria that were resistant to a variety of antibiotics, including ceftazidime (42.9%), cefuroxime (42.9%), and cefotaxime (44.6%), were found in our study. This shows that if a gram-negative bacterium is found in BSI, antibiotic drug selection for treatment should be based on susceptibility testing results because the practice of starting BSI patients on broad-spectrum antibiotics may be contributing to the development of multidrug resistance that is currently being observed. Furthermore, our study discovered that imipenem had an 84.6% sensitivity, norfloxacin had a 64.7% sensitivity, and nitrofurantoin had a 61.2% sensitivity. These results were consistent with the Serretiello et al. study's conclusion that E. coli had a high level of carbapenem and amikacin sensitivity [26] . Despite the fact that these antibiotics were still effective against isolated blood pathogens, the pathogens were slowly developing resistances, possibly as a result of their overuse, so various hospitals should consider implementing an efficient antimicrobial resistance surveillance system, such as antimicrobial stewardship programs and/or using the global antimicrobial resistance surveillance system (GLASS) to monitor the antibiotic resistant levels [23] .
Multidrug-resistant (MDR) pathogens are making common infections more difficult to treat or untreatable, and burdensome to the health care system. Studies have shown increased prevalence of ESBL producing strains and carbapenem resistance strains among blood pathogens [8-10] . The MDR patterns of bacterial isolates from our study clearly suggest that ESBL producing strains may be circulating at LUTH. Intensifying infections control and prevention practices, periodic antibiogram studies and implementing the antimicrobial stewardship program may reduce the generation of MDR strains and regulate antibiotic prescribing at the hospital level. Due to the retrospective nature of our study, we were unable to determine the current levels of antibiotic resistance at LUTH. Consequently, prospective antibiogram tests are warranted. Furthermore, it was observed that tetracycline was tested on blood isolates when it is not recommended for treating BSI but urinary tract infection. Therefore, antibiotic selection for susceptibility testing should be based on the CLSI and Zambia National Formulary recommendations.
CONCLUSION
A surge in MDR strains that cause blood stream infections has been reported in our study. Imipenem was still useful in treating these infections, but it risks of being overused. Additionally, S. aureus and Enterobacteriaceae were the most typical causes of blood stream infections at Livingstone University Teaching Hospital. Therefore, in order to minimize the numbers of MDR strains and manage blood stream infections caused by Enterobacteriaceae and S. aureus, the selection of antibiotics must be supported by laboratory evidence. Broad-spectrum antibiotics should only be prescribed as a last resort. If not, the high expense of treating bacterial infections may have an adverse effect on mortality and morbidity rates due to the observed dismal antibiotic resistant picture.
Declarations
Data Availability. The primary data used to support the findings of this study are included in the article.
Author’s contribution. TNM did data collection, analysis and wrote the manuscript. JAM performed data analysis and manuscript review. WC conceptualized the study, performed data analysis, and wrote the manuscript. All authors approved the current version of the manuscript.
Competing interests. The authors declare that there is no conflict of interest regarding the publication of this paper.
Funding Statement. The study received no funding
Acknowledgments. We would like to sincerely thank all members of staff in the Laboratory department at Livingstone Central Hospital for their work in generating data used in this study.
REFERENCES
- Viscoli C. Bloodstream Infections: The peak of the iceberg. Virulence 2016;7(3):248-51.
- Kp P, Arora V, Pp G. Bloodstream Bacterial Pathogens and their Antibiotic Resistance Pattern in Dhahira Region, Oman. Oman Medical Journal 2011;26(4):240-79.
- Wenzel RP, Edmond MB. The impact of hospital-acquired bloodstream infections. Emerging Infectious Diseases 2001;7(2):174.
- Lamy B, Sundqvist M, Idelevich EA. Bloodstream infections - Standard and progress in pathogen diagnostics. Clin Microbiol Infect 2020;26(2):142-50.
- Timsit J-F, Soubirou J-F, Voiriot G, Chemam S, Neuville M, Mourvillier B, et al. Treatment of bloodstream infections in ICUs. BMC Infectious Diseases 2014;14(1):489.
- Towns ML, Jarvis WR, Hsueh PR. Guidelines on blood cultures. J Microbiol Immunol Infect 2010;43(4):347-9.
- Akova M. Epidemiology of antimicrobial resistance in bloodstream infections. Virulence 2016;7(3):252-66.
- Opintan JA, Newman MJ. Prevalence of antimicrobial resistant pathogens from blood cultures: results from a laboratory based nationwide surveillance in Ghana. Antimicrobial Resistance & Infection Control 2017;6(1):64.
- Saeed DK, Farooqi J, Shakoor S, Hasan R. Antimicrobial resistance among GLASS priority pathogens from Pakistan: 2006-2018. BMC infectious diseases 2021;21(1):1231-.
- Gandra S, Mojica N, Klein EY, Ashok A, Nerurkar V, Kumari M, et al. Trends in antibiotic resistance among major bacterial pathogens isolated from blood cultures tested at a large private laboratory network in India, 2008-2014. Int J Infect Dis 2016;50:75-82.
- Mulongo T, Kamvuma K, Phiri CN, Mulemena JA, Chanda W. Elevators and staircase handrails as potential sources of nosocomial pathogens at Ndola Teaching Hospital, Zambia. 2021.
- Chanda W, Mulemena JA, Manyepa M, Kamvuma K. Antimicrobial stewardship and oxazolidinones use, a consideration for a Zambian health system. Medical Journal of Zambia 2019;46(3):165-71.
- Chanda W, Manyepa M, Chikwanda E, Daka V, Chileshe J, Tembo M, et al. Evaluation of antibiotic susceptibility patterns of pathogens isolated from routine laboratory specimens at Ndola Teaching Hospital: A retrospective study. PLOS ONE 2019;14(12):e0226676.
- Chiyangi H, Muma JB, Malama S, Manyahi J, Abade A, Kwenda G, et al. Identification and antimicrobial resistance patterns of bacterial enteropathogens from children aged 0–59 months at the University Teaching Hospital, Lusaka, Zambia: a prospective cross sectional study. BMC infectious diseases 2017;17(1):1-9.
- Mshana SE, Matee M, Rweyemamu M. Antimicrobial resistance in human and animal pathogens in Zambia, Democratic Republic of Congo, Mozambique and Tanzania: an urgent need of a sustainable surveillance system. Annals of Clinical Microbiology and Antimicrobials 2013;12(1):1-10.
- Kasanga M, Mukosha R, Kasanga M, Siyanga M, Mudenda S, Solochi BB, et al. Antimicrobial resistance patterns of bacterial pathogens their distribution in university teaching hospitals in Zambia. Future Microbiol 2021;16:811-24.
- Tian L, Zhang Z, Sun Z. Antimicrobial resistance trends in bloodstream infections at a large teaching hospital in China: a 20-year surveillance study (1998-2017). Antimicrobial Resistance & Infection Control 2019;8(1):86.
- CSLI. Performance Standards for antimicrobial susceptibility testing. 26 ed. Wayne PA: Clinical and laboratory standards institute; 2016.
- Laupland KB, Pasquill K, Steele L, Parfitt EC. Burden of bloodstream infection in older persons: a population‐based study. BMC Geriatrics 2021;21(1):31.
- Page DB, Donnelly JP, Wang HE. Community-, Healthcare-, and Hospital-Acquired Severe Sepsis Hospitalizations in the University HealthSystem Consortium. Crit Care Med 2015;43(9):1945-51.
- Castillo DJ, Rifkin RF, Cowan DA, Potgieter M. The Healthy Human Blood Microbiome: Fact or Fiction? Front Cell Infect Microbiol 2019;9:148.
- Zozaya-Valdés E, Wong SQ, Raleigh J, Hatzimihalis A, Ftouni S, Papenfuss AT, et al. Detection of cell-free microbial DNA using a contaminant-controlled analysis framework. Genome Biol 2021;22(1):187.
- Sirijatuphat R, Sripanidkulchai K, Boonyasiri A, Rattanaumpawan P, Supapueng O, Kiratisin P, et al. Implementation of global antimicrobial resistance surveillance system (GLASS) in patients with bacteremia. PLOS ONE 2018;13(1):e0190132.
- Franceschini E, Santoro A, Menozzi M, Bacca E, Venturelli C, Zona S, et al. Epidemiology and Outcomes of Bloodstream Infections in HIV-Patients during a 13-Year Period. Microorganisms 2020;8(8).
- de Kraker MEA, Davey PG, Grundmann H, on behalf of the Bsg. Mortality and Hospital Stay Associated with Resistant Staphylococcus aureus and Escherichia coli Bacteremia: Estimating the Burden of Antibiotic Resistance in Europe. PLOS Medicine 2011;8(10):e1001104.
- Serretiello E, Santella B, Folliero V, Iervolino D, Santoro E, Manente R, et al. Prevalence and Antibiotic Resistance Profile of Bacterial Pathogens in Aerobic Vaginitis: A Retrospective Study in Italy. Antibiotics (Basel, Switzerland) 2021;10(9):1133.
Medical Journal of Zambia, Vol 49, 3
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.