Assessing a New Medical School in Zambia Using Dundee Ready Educational Environment Measurement: A cross-sectional study.
Christian Chinyere Ezeala
1School of Medicine and Health Sciences, Mulungushi University, Livingstone Campus, Livingstone, Zambia
Mercy Okwudili Ezeala
2Department of Psychiatry, School of Medicine, University of Zambia, Zambia
Wilson Zimba
1School of Medicine and Health Sciences, Mulungushi University, Livingstone Campus, Livingstone, Zambia
DOI: https://doi.org/10.55320/mjz.49.3.360
Keywords:DREEM, Educational Environment, Medical school, students’ perception, Zambia
ABSTRACT
Background: Learners’ perception of learning environment reflects educational program’s effectiveness. For new medical schools, determining effectiveness of teaching and learning is desirable quality assurance process.
Aim: To determine pioneer medical students’ perception of learning environment of a new school using Dundee Ready Educational Environment Measurement (DREEM).
Methods: Quantitative cross-sectional study design was adopted. Consenting medical students in second and third years of Bachelor of Medicine and Surgery degree program were surveyed with a questionnaire comprising a demographic competent and 50 DREEM items. Non-probability sampling was adopted. Completed questionnaires were sorted and rated. The resulting quantitative data were analysed for mean scores with SPSS 21 software. Mean total scores and mean scores in five subscales were determined. Scores on individual items were also analysed. Cronbach’s alpha was used to assess dataset reliability.
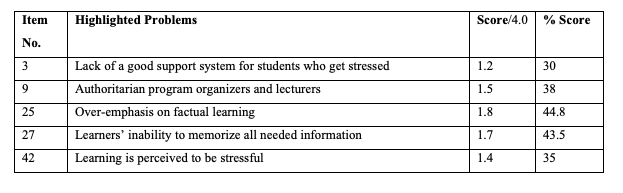
Results: The study recorded 137 participants, 54.2 % females and 45.8 % males. Mean age was 22 (± 4.03) years. Mean total DREEM score was 117.5 (58.8 %) and interpreted as “more positive than negative.” Scores in subscales of perception of learning, perception of teachers, academic self-perception, and perception of atmosphere, were positive with mean scores of 62.9 %, 60.2 %, 63.4 %, and 55.6, respectively. Subscale of social self-perception rated poorly with mean score of 48.9 % and interpreted as “not a nice place.” Single items revealed five major problem areas: lack of adequate support, authoritarian leadership, over-emphasis on factual learning, poor memorizing, and excessive stress.
Conclusion: This analysis revealed major problems and weaknesses in the new school and addressing them could improve educational quality.
INTRODUCTION
Educational environment measurement provides a yardstick for assessing the quality of a medical educational program. For this reason, assessment of learning environments of medical schools is a common practice [1, 2] . It is carried out for a variety of purposes which may include quality assurance, determining students’ satisfaction, strategic planning, and making comparisons of curricula models or training sites[3 -5] . The educational environment comprises several elements, and according to Ezeala [6] , these may be situational factors, curriculum, material resources, organizational culture, and institutional leadership. Learning environments have been described as learner-centred, knowledge-centred, assessment-centred, or community-centred [7] . Land and Johanssen [8] proposed five theoretical foundations of learning environments. These are psychological, pedagogical, technological, cultural, and pragmatic foundations. Psychological foundations are concerned with the learning theories such as cognitivism, constructivism, and cognitivism based upon which a medical education program is designed. The pedagogical foundation looks at how learners acquire knowledge, specifically the teaching approaches adopted in the program. Fundamentally, medical education programs are based on adult learning principles. Technological foundation refers to the application of technology and digital learning in medical education. Cultural foundations point to the values, assumptions, and norms of the educational community. These are expressed in such nuances as interprofessional education, problem-based learning, and contextual learning. This also reflects the way problems are handled within the learning community. Pragmatic foundation emphasizes adaptive procedures in the management of available institutional resources and in addressing challenges to provide optimal learning environment. Proper integration and alignment of these five foundations, otherwise known as grounded design, is necessary to optimise student-centred learning in an environment that is suitable for producing high-quality healthcare workers [6, 8] .
Conventionally, educational environment measurement considers learners’ perception of the environment using one or more of several tools [9, 10] . This measurement approach is important because learners’ perception of the educational environment is closely linked to student motivation, approach to learning, and the outcomes of the learning process [11] . In other words, learners’ perception of the learning environment, reflects the educational program’s quality.
The last five years witnessed unprecedented increase in the number of new medical schools in Zambia. This occurred amidst shortage of educational infrastructure, learning resources, and qualified teaching staff. Although regulatory authorities use stringent criteria and processes to license and accredit these medical schools, it is needful to assess the learning contexts of these new schools through the lenses of the learners themselves. Therefore, this study aimed to determine students’ perception of their learning, their teachers, and their sociocultural environment, and to analyse the specific issues affecting teaching and learning in one these new medical schools.
METHODS
Study design and description of the survey instrument:
The study was a quantitative cross-sectional survey of year 2 and year 3 students between 2019 and 2020 (before the pandemic restrictions). It used the Dundee Ready Educational Environment Measurement (DREEM) questionnaire [12] which provided quantitative data. The epistemological stance of the study was positivism.
The survey instrument has 50 items to which participants responded based on a 5-point Likert scale – (i) Strongly agree, (ii) Agree, (iii) No opinion, (iv) Disagree, and (v) Strongly disagree. These were rated 4, 3, 2, 1, and 0, respectively based on a recommended rubric by the questionnaire authors. Nine items were negative statements and were rated in the reverse order whereby at the extremes of the range, strongly agree rated as 0 while strongly disagree rated as 4. The maximum score for each item was 4 while the maximum total DREEM score for the 50 items was 200.
The 50 DREEM items aggregated into 5 subscales as recommended by the authors. These subscales were:
- Perception of learning which has 12 items and maximum score of 48: this domain defines how the respondents view teaching and learning within the academic program.
- Perception of teacher/program organizers which has 11 items and maximum score of 44: this domain evaluates qualities of their lecturers and program organizers.
- Academic self-perception which has 8 items and maximum score of 32: this subscale evaluates the learners’ perception of their achievement in the program.
- Perception of the educational atmosphere which as 12 items and maximum score of 48: The subscale evaluates the learners’ views on the teaching and learning atmosphere of the program.
- Social self-perception which has 7 items and maximum score of 28: In this subscale, we learn about how the learners feel about their social life within the learning setting.
The scores were interpreted based on the DREEM authors’ recommendation [13] . For the total domain, a score of 0 - 50 represented “very poor” educational environment, 51 – 100 represented an educational environment with “plenty of problems”, 101-150 represented an environment that is “more positive than negative”, while a score of 151 – 200 represented an “Excellent” educational environment. Based on the rubric, the following interpretations were applied to scores from the five subscales:
- ‘Perception of learning’ domain (Max score 48): A score between 0 and12 represented a “very poor” perception, 13 and 24 indicated that “teaching is viewed negatively”, 25 and 36 represented “a more positive” view, while scores between 37 and 48 showed that “teaching is highly thought of.”
- ‘Perception of teachers’ domain (max score 44): A score between 0 and 11 indicated “abysmal” view of teachers, 12 and 22 indicated a view that the “teachers needed some training,” 23 and 33, a view that things were “moving in the right direction,” and 34-44, a view that the instructors were “model teachers.”
- ‘Academic self-perception’ domain (max score 32) A score of 0 – 8 symbolised ‘feeling of total failure’, 9 – 16 ‘many negative aspects,’17 – 24 ‘Feeling more on the positive side,’ and 25 – 32 ‘confident.’
- ‘Perception of the Atmosphere’ domain (max score 48): In this domain, a score of 0 – 12 was rated as ‘a terrible environment,’ 13-24 as ‘many issues that need changing,’ 25 -36 as ‘a more positive attitude,’ and 37 – 48 as ‘a good feeling overall.’
- ‘Social Self-Perception domain (max score 28): The scores in this subscale were interpreted thus: 0 -7 ‘miserable,’ 8 – 14 ‘not a nice place,’ 15 – 21 ‘not too bad a place,’ and 22 – 28 ‘very good socially.’
The survey tool also included a demographic component from which information on year of study, age, gender, nationality, and marital status were collected.
Study setting:
The setting of this study was a new medical school in the Southern Province of Zambia which began operations in January 2018. The school operated a traditional six-years competency-based medical education curriculum involving one year of basic sciences, two years premedical studies in the basic medical sciences disciplines, and three years clinical education that is largely hospital based. The contents of the premedical phase disciplines were synchronised along body organs and systems.
Ethical Statement:
The proposal for the study was cleared by the school’s ethics committee. Each potential participant received a document that explained the purposes and involvement in the study (information sheet) and a copy of the questionnaire. Consenting students signed hard copies of the consent form and were allowed to voluntarily complete and return the questionnaire unassisted. Reminders were posted on the classes’ social media, with each reminder emphasizing participant autonomy. Participants were not allowed to write their names or any identifying information on the questionnaire and consent forms. Access to all returned copies of the questionnaire were restricted to the investigators and confidentiality was maintained in line with the school’s ethics committee guidelines.
Sample size and sampling procedure:
The sample size was calculated based on the total enrolment in the specified classes, a margin of error of 5 %, confidence interval of 95 %, and population proportion of 50 %. Only students enrolled in and actively engaged in the medical education program of the school were included in the study. Simple convenience non-probability sampling was used with every student given opportunity to participate.
Data Analysis:
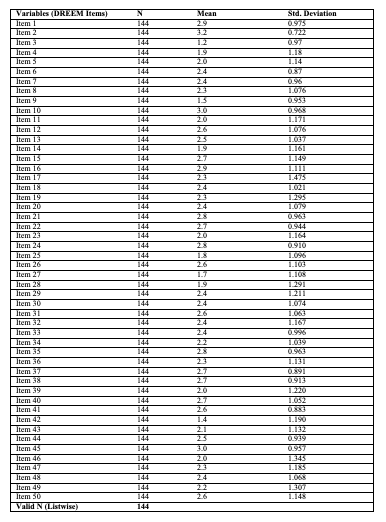
The returned copies of the questionnaire were sorted and checked for complete and correct responses. Demographic data were analysed quantitatively. The responses to the DREEM items were rated based on the above rubric and the data analysed descriptively for mean and standard deviation using SPSS software (version 21). Cronbach’s alpha coefficient was determined as a measure of internal consistency (reliability) of the test data for the total dataset and for each DREEM subscale.
RESULTS
Demographics:
The total number of students enrolled in the medical education program at the time of the study was 210. Using a response distribution of 50 %, this gave a sample size of 137. A total of 150 questionnaires were randomly distributed to the students. The number of usable completed questionnaires included in this report was 144, giving a response rate of 96 %. Of these, 96 were from year 2 while 48 were from year 3; 78 (54.2 %) were females and 66 (45.8 %) were males. The mean age was 22 years (standard deviation 4.0).
DREEM Scores:
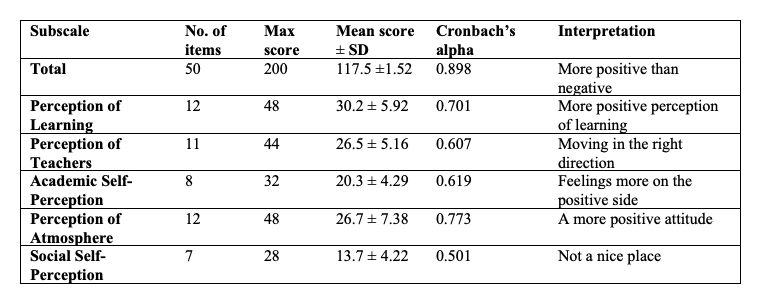
The overall mean score for the total 50 DREEM items was 117.5 ± 21.5 (table 1). This corresponds to an interpretation of “More positive than negative” perception of the educational environment.
The mean scores for the five subscales of the DREEM tool and their interpretations are shown in table 1. All the subscales recorded a positive perception apart from the subscale of social self-perception which recorded a mean score less than 50 % and interpreted as “not a nice place.”
DISCUSSION
The study analysed the learning context of the new Mulungushi University School of Medicine and Health Sciences located in Zambia using the Dundee Ready Educational Environment Measurement tool. Chan et al[14] recently pointed out in a systematic review that academic achievement, quality of life, academic resilience, positive attitude, and preparedness for practice, correlated positively with learners’ perception of the educational environment when measured with the DREEM tool. In this study, a total DREEM score of 117.5/200 (58.8 %) indicated that the students were positive about their learning environment. This is comparable to previous reports from studies conducted in other similar institution in Zambia[15] , sub-Saharan Africa [16, 17,] and elsewhere[18, 19] . The observed DREEM scores were however lower that observations from medical schools located in Western countries and reflects the more difficult settings of medical schools in sub-Saharan Africa. Most of these school operate the traditional lecture-based curriculum. Roff[20] and Zawawi [21] independently concluded that medical schools operating a traditional curricula often record DREEM scores that are lower that 60 % (i.e. 120/200) when compared to medical schools operating problem-based curricula. The learning environment of this new school need to be improved to enhance the quality of its academic delivery and improve the quality of the educational products.
The subscale scores similarly showed positive perception in four of the five DREEM subscales. The subscales of perception of learning, perception of teachers, academic self-perception, and perception of the learning atmosphere all had positive rating with scores that were greater than 50 %. These are admirable ratings for a new medical school located in a resource constrained setting. These scores are very similar to those reported in the studies cited above[15, 18, 19] . The subscale of social self-perception, however, was rated poorly, recording a mean DREEM score below 50 %. The rating in this subscale also appears lower that those reported by other studies[15] . This low rating may be due to limited social interaction for the students at the time of this study as the medical school was located away from the main University Campuses in Kabwe, it had no recreational facilities, and no residential services (all the students were living off-campus). The University has since made admirable efforts to address these social challenges.
In an earlier report, Ezeala[15] opined that in addition to curriculum models, behaviour and beliefs of instructors and the methods of curriculum delivery may play significant roles in determining the quality of the educational environment. Results from the analysed specific items scores indicated that system issues such as teacher and program managers’ authoritarian behaviour, inadequacy of support for stress management, and the tendency to overemphasize factual learning, compounded the stress associated with learning in this medical school. These issues needed to be appropriately addressed to improve learning in the school and the overall quality of medical education. The constructivist educational philosophy intones that the learner should take charge of his/her learning. This way, the learner has opportunity to reflect on and construct meaning from educational experiences. This also reduces classroom dictatorship. However, despite general acceptance of student-centred learning in medical education, persistent reports of teacher authoritarianism in African medical schools are worrisome[15, 16] . The authors of this work believe that students should be trained in stress management strategies[22, 23] and that the program content and delivery strategies should be periodically reviewed to de-emphasize excessive factual content, which may result in surface learning strategies with the consequent poor learning outcomes24.
DECLARATIONS
AUTHORS’ CONTRIBUTIONS
All the authors contributed equally to the conception. Development and execution of the study.
FUNDING:
The study received no internal or external funding.
CONFLICT OF INTEREST:
The authors declare no conflict of interests.
REFERENCES
- Boukhris K, Zedini C, El Ghardallou M. Nurse students' perception of the academic learning environment in Tunisian institutes of nursing sciences: A multisite cross-sectional study. Nursing Education Today 2022;111:105316. https://doi.org/10.1016/j.nedt.2022.105316
- Rusticus SA, Wilson D, Jarus T, O’Flynn-Magee K, Albon S. Exploring student perceptions of the learning environment in four health professions education programs. Learning Environment Research 2022;25(1):59-73. https://doi.org/10.1007/s10984-021-09349-y
- Debroy A, Ingole A, Mudey A. Promotion H. Teachers' perceptions on student evaluation of teaching as a tool for faculty development and quality assurance in medical education. Journal of Education and Health Promotion. 2019; 8: 218. Doi: 10.4103/jehp.jehp_47_19
- Ezeala CC, Moleki MM. Undergraduate Students’ Perception of the Educational Environment of a Medical School Provided a Framework for Strategic Planning. Current Trends in Medicine and Medical Research 2020:5:72-81. Retrieved from: https://stm1.bookpi.org/index.php/ctmmr-v5/article/view/969
- Till H. Identifying the perceived weaknesses of a new curriculum by means of the Dundee Ready Education Environment Measure (DREEM) Inventory. Medical Teacher 2004;26(1):39-45.
- Ezeala CC. Analysis of the undergraduate students’ learning environment in a medical school in Zambia. DLitt et Phil Thesis, Pretoria: University of South Africa 2016.
- National Research Council. How people learn: Brain, mind, experience, and school: Expanded edition. Washington DC: National Academies Press; 2000 Sep 11.
- Land SM, Hannafin MJ, Oliver K. Student-centered learning environments: Foundations, assumptions, and design. In: Theoretical Foundations of Learning Environments 2012 Mar 22 (pp. 3-25). Routledge.
- Soemantri D, Herrera C, Riquelme A. Measuring the educational environment in health professions studies: a systematic review. Medical Teacher 2010;32(12):947-52.
- Mousavi A, Mohammadi A, Mojtahedzadeh R, Shirazi M, Rashidi H. E-Learning Educational Atmosphere Measure (EEAM): A New Instrument for Assessing E-Students' Perception of Educational Environment. Research in Learning Technology 2020;28.
- Lizzio A, Wilson K, Simons R. University students' perceptions of the learning environment and academic outcomes: implications for theory and practice. Studies in Higher
- Roff S, McAleer S, Harden RM, Al-Qahtani M, Ahmed AU, Deza H, Groenen G, Primparyon P. Development and validation of the Dundee Ready Education Environment Measure (DREEM). Medical Teacher 1997;19(4):295-9.
- McAleer S, Roff SJAmeg. A practical guide to using the Dundee Ready Education Environment Measure (DREEM). AMEE Medical Education Guide 2001;23(5):29-33.
- Chan CYW, Sum MY, Tan GMY, Tor P-C, Sim K. Adoption and correlates of the Dundee Ready Educational Environment Measure (DREEM) in the evaluation of undergraduate learning environments–a systematic review. Medical Teacher 2018;40(12):1240-7.
- Ezeala CC, Moleki MM. Evaluation of the educational environments of undergraduate medicine and pharmacy programmes at the University of Zambia. Research and Development in Medical Education 2018;7(1):14-20.
- Ogun OA, Nottidge TE, Roff S. Students’ perceptions of the learning environment in two Nigerian medical schools offering different curricula. Ghana Medical Journal 2018;52(3):116-21.
- Ezomike U, Madubogwu C, Azuike E. Evaluation of the educational environment of a new medical school in southeast Nigeria. Nigerian Journal of Clinical Practice 2020;23(10):1462.
- Bakhshialiabad H, Bakhshi G, Hashemi Z, Bakhshi A, Abazari F. Improving students' learning environment by DREEM: an educational experiment in an Iranian medical sciences university. BMC Medical Education (2011–2016). 2019;19(1).
- Bavdekar S, Save S, Pillai A, Kasbe A. DREEM Study: Students Perceptions of Learning Environment in a Medical College in Mumbai, India. The Journal of the Association of Physicians of India 2019;67(4):50-4.
- Roff S. The Dundee Ready Educational Environment Measure (DREEM)—a generic instrument for measuring students’ perceptions of undergraduate health professions curricula. Medical Teacher 2005;27(4):322-5.
- Zawawi AH, Elzubeir M. Using DREEM to compare graduating students′ perceptions of learning environments at medical schools adopting contrasting educational strategies. Medical Teacher 2012;34(sup1):S25-S31.
- Ribeiro ÍJ, Pereira R, Freire IV, de Oliveira BG, Casotti CA, Boery EN. Stress and quality of life among university students: A systematic literature review. Health Professions Education 2018;4(2):70-7.
- Dyrbye LN, Sciolla AF, Dekhtyar M, Rajasekaran S, Allgood JA, Rea M, et al. Medical school strategies to address student well-being: a national survey. Academic Medicine 2019;94(6):861-8.
- Cavanagh A, Vanstone M, Ritz S. Problems of problem-based learning: Towards transformative critical pedagogy in medical education. Perspectives on Medical Education 2019;8(1):38-42.
Medical Journal of Zambia, Vol 49, 3
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.