Aspiration of Barium Contrast by a Geriatric Patient with Gastroparesis: A case report
Shamiso Chitemamwise
Harare Institute of Technology, Harare, Zimbabwe
Bornface Chinene
Harare Institute of Technology, Harare, Zimbabwe
DOI: https://doi.org/10.55320/mjz.49.3.358
Keywords:Barium swallow, Gastroparesis, aspiration,dysphagia
ABSTRACT
Complications due to aspiration of barium contrast occur rarely during studies of the digestive tract. While lung tissue can tolerate small amounts of Barium large quantities can exceed the lung’s capacity and consequently lead to death especially, in geriatric patients. Barium contrast can affect pulmonary ventilation and perfusion function, causing dyspnoea, hypoxemia and respiratory failure. We herein report a barium swallow case in which an 82-year-old woman aspirated barium on the first swallow and was diagnosed with Gastroparesis. The history, procedure and patient management are discussed. The purpose of the case report is to add to the existing literature on aspiration cases during barium swallow studies and the outcomes after the aspiration. Furthermore, this case report also highlights a need for extra care when attending to senior patients with dysphagia during barium studies.
INTRODUCTION
A barium swallow study is a contrast-enhanced radiographic study commonly used to assess structural characteristics and to some extent the functional characteristics of the oesophagus.[1] This study is commonly requested in cases of dysphagia. It can also be requested for achalasia, oesophageal cancer, gastroesophageal reflux disease (GERD) and assessment of hiatus hernia.[2] The study involves administering a contrast medium to a patient and taking images and videos showing how the contrast moves down the oesophagus. Achalasia is a type of oesophageal motility disorder. A barium swallow is useful for assessing oesophageal motility and it is used for the initial diagnosis. Collapsed stomach symptoms are also similar to those of achalasia and esophageal cancer. It is also known as gastroparesis and can partly be seen on a barium swallow test when the gastroesophageal junction is demonstrated. This report describes a barium swallow case in which the barium aspirated on the first swallow and showed a collapsed stomach in a geriatric woman. The aspiration of barium contrast is a rare complication. While lung tissue can tolerate small amounts of Barium large quantities can exceed the lung’s capacity and consequently lead to death, especially in geriatric patients.[2] Barium contrast can distress the pulmonary ventilation and perfusion function, causing dyspnoea, hypoxemia and respiratory failure. The aim of this report is to add to the existing literature on aspiration cases during barium swallow studies. Furthermore, this case report also highlights a need for extra care when attending to elderly patients with dysphagia during barium studies.
PATIENT PRESENTATION
An 82-year-old female presented to an imaging centre with a request from the referring physician for a barium swallow study. The request was querying achalasia or oesophageal cancer. The patient was experiencing mild chest pains and heartburn. She was also frail and weak as she had been on a liquid diet for almost a month since she was experiencing difficulties in swallowing solid foods. Due to the liquid diet, the patient has lost weight significantly.
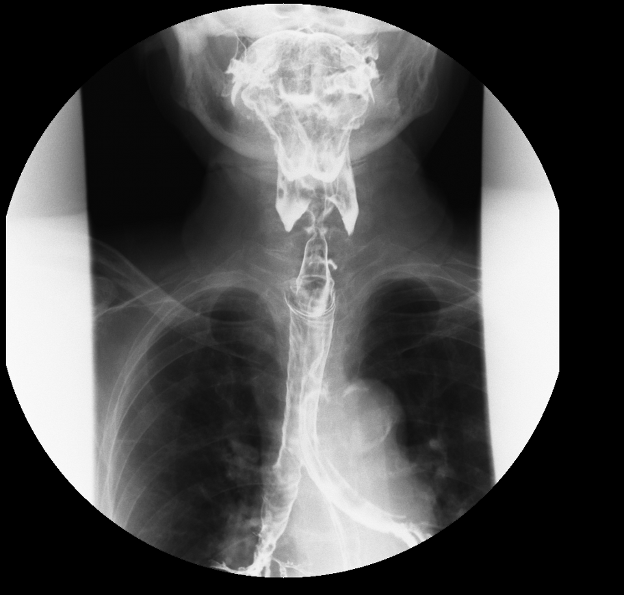
A barium swallow study was performed using a Toshiba Zexira model over the couch fluoroscopic unit. Prior to the study, the patient was asked to starve for eight hours on the booked examination day. On the day, she was asked to remove her clothes and put on a hospital gown and the patient was assisted by their caregiver. The procedure was explained to her including the instructions they were to be given during imaging. She was asked about her allergies to which she said she had no known allergies. The patient was informed of the possible complications such as constipation since the barium sulphate tends to harden and obstruct the bowel and the possibility of aspiration was highlighted. The fluoroscopic couch was tilted to a vertical position and the tube was horizontal. The patient was asked to stand on the footrest facing the tube. Control images of the cervical oesophagus were taken in the anteroposterior view as well as the lateral view. The patient was then given a suspension of the barium sulphate in a tumbler and asked to take a mouthful and hold it in her mouth. She was then asked to swallow whilst images were being taken using 75kV, 40mA and 50ms. Due to uncoordinated swallowing movements, the suspension spilt into the pharynx and the examination had to be stopped at that point. Figure 1 shows the aspiration of barium in the trachea (smaller arrow) and the pooling of barium in the valleculae and pyriform fossae (bigger arrow).
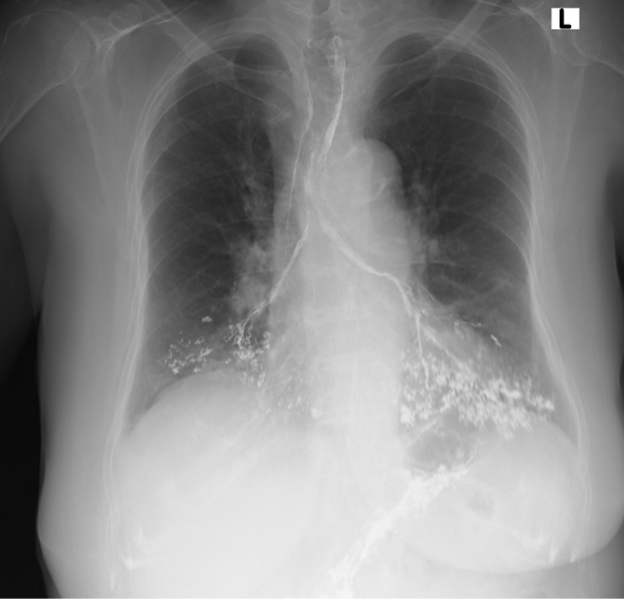
A physiotherapist was called in to perform chest physiotherapy. After that, an erect posterior anterior chest x-ray still showed significant amounts of barium in the tracheobronchial tree (Figure 2).
The images obtained from the barium swallow study suggested a possible lesion in the proximal third oesophagus extending to involve the cervical oesophagus (Figure 1). There was poor distension of the proximal third thoracic oesophagus with no definite narrowing and the stomach remained collapsed. The barium swallow study was limited by aspiration after the first swallow. After physiotherapy, there was still significant barium in the tracheobronchial tree as shown in Figure 3. Figure 4 shows the collapsed stomach and pooling of barium.



After the barium swallow study stopped because of aspiration, further study with CT was suggested for further evaluation. The CT scan showed that there was minimal apparent thickening of the oesophagus at the level of the tracheal carina which may be causing luminal narrowing. The oesophagus is collapsed so its thickness could not be assessed. The CT also showed that there was barium in the bronchoalveolar tree from the barium swallow and most of the barium was seen in the lower left lung (Figure 5). There was apparent thickening of the oesophagus at the oesophogastric junction which is due to a small hiatus hernia. The stomach was collapsed. The patient was then booked for surgery; she came a day before to be observed and monitored. After surgery, she was admitted into ICU for close monitoring and a prokinetic drug metoclopramide (Reglan) was prescribed. She was discharged after one week.
DISCUSSION
Barium swallow studies are commonly used in identifying causes of dysphagia. It is generally a safe test but like any other procedure, there are occasional complications. Possible complications include leakage of barium from an unsuspected perforation, allergic reaction to the barium drink or constipation due to obstruction of the bowel by the contrast agent.[3] The above-mentioned complications usually occur after the procedure has been completed. However, there is a complication which results in the immediate stopping of the procedure, this is when aspiration occurs. Aspiration occurs when barium leaks into the trachea and it calls for an immediate stop of the procedure. Alternative modalities can be considered if the acquired images do not provide a diagnosis.[4] They make use of a fluoroscopic unit that can take spot films and videos which are important for diagnosis as they give the physician or radiologist a chance to observe exactly how the swallowing process occurred during the procedure even if they were not there at the time of the procedure. In a study by Nin[5] , barium studies were proven to improve significant radiologic findings related to chronic cough in 11.5% of patients. Barium swallow studies have also been successfully used in diagnosing gastroesophageal reflux disease, oesophageal cancer and other conditions. The barium study is therefore a global test that can be used to assess both functional and structural diseases of the oesophagus. It is also simple, non-invasive, and inexpensive and rarely has any complications.
Achalasia is characterized by oesophageal aperistalsis and impaired relaxation of the lower oesophageal sphincter during swallowing. Patients often present with progressive dysphagia, heartburn, chest pain, regurgitation and varying degrees of unintentional weight loss.[6] According to Patel[7] , “the annual incidence of achalasia is approximately 1 in 100,000 people worldwide, with an overall prevalence of 9 to 10 in 100,000 people.”
Barium swallow studies are carried out in cases of high or low dysphagia, persistent vomiting, gastroesophageal reflux disease (GERD), assessment of hiatus hernia, generalized epigastric pain or assessment of fistula.[8, 9, 10] The patient in this case presented with dysphagia, weight loss, mild chest pain and heartburn. The barium swallow study was terminated after one mouthful as there was aspiration. Although there is a paucity of cases clearly stating that aspiration occurred from one mouthful, in this case, it can be attributed to the uncoordinated swallowing movements due to the difficulty in swallowing experienced by most people with ageing.[11, 12] Barium aspiration occurs occasionally in studies of the upper gastrointestinal tract and usually, only small amounts pass into the airways.[13] When only small amounts of barium leak into the airways, the patient is likely to remain asymptomatic such that the only evidence is a visible passage of barium into the larynx and trachea on the image. However, when a larger volume of barium leaks into the airways, the patient may become symptomatic presenting dyspnoea, fever, coughing and hypoxia. In this case, the patient coughed immediately after the barium leaked into the airways. According to Murphy[13] , the largest case review that has been published shows that out of 22 adult patients who aspirated, there were eight fatalities. He suggests that this is likely to be an overstated mortality rate of barium aspiration with literature not recording many cases of mild aspiration. A case report by Vatharaj4, describes a 70-year-old lady who aspirated large amounts of barium and received supportive care, antibiotics and chest physiotherapy. The lady recovered with no residual chest symptoms. This 70-year-old lay’s case is similar to this case in that after physiotherapy, there was still a significant amount of barium in the airways but the patient had no residual symptoms.
The images that were taken in this case managed to show that the stomach remained collapsed. This could be attributed to the fact that very little amount of the barium made it to the stomach as most of it had leaked into the airways. However, after further evaluation using CT, the oesophagus and the stomach were collapsed. In a case report by Vatharaj[4] , the patient was imaged using high-resolution CT which showed a mass in the cervical oesophagus and was managed with radiotherapy. In this case, CT was useful in a further study of the patient’s gastrointestinal tract such that a conclusion was reached that the patient’s oesophagus was collapsed resulting in luminal narrowing and the stomach was also collapsed. CT was a better substitute for fluoroscopic imaging as there is better tissue differentiation in this modality. Endoscopic ultrasonography can also be used to assess the digestive tract. It combines endoscopy with ultrasound to produce detailed images of the digestive tract.[14]
The CT findings also included a small hiatus hernia. Surgery is an effective way of treating hiatal hernias. It has a 90 to 95% chance of relieving symptoms such as acid reflux. According to Leonard,[15] small hiatus hernia with mild symptoms such as heartburn, and gastroesophageal reflux disease does not require surgery for treatment but can be treated with medications or changes in lifestyle. However, in this case, the patient was treated for a small hiatus hernia with surgery. Gastroparesis is managed by assessment and correction of nutritional state, relief of symptoms and improvement of gastric emptying. The nutritional state should be managed by oral dietary modification. Pharmacological therapy can be employed for the relief of symptoms and improvement of gastric emptying. Medications including metoclopramide and erythromycin are used to stimulate stomach muscles whilst diphenhydramine can be used if nausea and vomiting persist. Some patients may not be able to eat or drink and in this case a jejunostomy tube is placed in the small intestines and this is a temporary solution used when gastroparesis is severe.[14] In this case, the patient was prescribed metoclopramide to be taken before meals over a period of 12 weeks after which a review will be made.
Conclusion
Barium swallow studies are the gold standard in diagnosing dysphagia, oesophageal motility and oesophageal cancer. Endoscopic ultrasonography can also be used but it is not the first port of call since it is an invasive procedure. This case report confirms the suggestion by Murphy,[13] that cases in literature stating that in major aspiration cases there is a high risk of fatality is an overstatement as the patient in this case recovered with no residual symptoms after a major aspiration. Furthermore, this case shows that extra care has to be taken when carrying out a barium swallow procedure with geriatric patients who already have dysphagia as there is a risk of aspiration which may lead to other complications.
REFERENCES
- Yadlapati R. 2019. Oesophageal Motility Testing. [Online]. [Viewed 30/11/21]. Available from https://hopkinsmedicine.org
- Bell D, J. 2021. Barium Swallow. [Online]. [Viewed 30/11/21]. Available from https://www.radiopeadia.org
- Arasi, T, V. 2020. What is Barium Swallow Test? [Online]. [Viewed 30/11/21]. Available from https://emedicinehealth.com
- Varatharaj, A. 2011. Barium Aspiration. [Online]. [Viewed 30/11/21]. An international Journal of Medicine. Volume 105, Issue no 9. Pages 903-904
- Nin C,S. 2013. Barium Swallow Study in Routine Clinical Practice. [Online]. [Viewed 1/12/21]. Available from https://europepmc.org
- Kraichely R.E and Farrugia, G. 2006. Achalasia: physiology and etiopathogenesis. [Online]. [Viewed 1/12/21]. Available from https://academic.oup.com
- Patel D.A. 2017. An overview of achalasia. [Online]. [Viewed 1/12/21]. Available from https://ncbi.nlm.nil.gov
- Chieng, R. 2022. Barium Swallow. [Online]. [Viewed 31/07/22]. Available from https://radiopedia.org
- Chen, A. 2022. Barium Swallow. [Online]. [Viewed 01/08/22]. Available from https://www.ncbi/nlm.nih.gov
- Dreis, M. 2021. What is a barium Swallow Test? [Online]. [Viewed 01/08/22]. Available from https://www.ncbi.nlm.nih.gov
- Christmas, C. 2019. Swallowing Disorders in the Older Population. [Online]. [Viewed 31/07/22]. Available from https://www.ncbi.nlm.nih.gov
- Sura, L. 2012. Dysphagia in the Elderly. [Online]. [Viewed 30/07/22]. Available from https://www.ncbi.nlm.nih.gov
- Murphy A. 2021. Barium Aspiration. [Online]. [Viewed 1/12/21]. Available from https://radiopeadia.org
- Mayo Clinic. 2020. Diagnosis and Management of Patients with Gastroparesis. [Online]. [Viewed 1/12/21]. Available from https://www.mayoclinic.org
- Leonard J. 2018. What to know about Hiatal Hernia Surgery. [Online]. [Viewed 1/12/21]. Available from https://medicalnewstoday.com
Medical Journal of Zambia, Vol 49, 3
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.