Prevalence and Factors Associated with Short Interpregnancy Intervals among Women Attending Antenatal Care at First-Level Hospitals in Lusaka, Zambia
Imanga Ikabongo
University Teaching Hospital, Women and Newborn Hospital, Nationalist Road, Lusaka, Zambia.
Bellington Vwalika
University Teaching Hospital, Women and Newborn Hospital, Nationalist Road, Lusaka, Zambia.
Mwansa K. Lubeya
University of Zambia, School of Medicine, Department of Obstetrics and Gynaecology, Nationalist Road, Lusaka, Zambia.
DOI: https://doi.org/10.55320/mjz.50.3.352
Keywords:Short interpregnancy intervals, antenatal care, maternal adverse outcomes, perinatal adverse outcomes
ABSTRACT
Background: Research has shown that short Interpregnancy Intervals (IPIs) are associated with adverse maternal and perinatal outcomes. The aims and objectives of this study was to determine the prevalence of short IPI’s and further determine the demographic, sociocultural and health care related factors associated with short IPI’s among women of reproductive age in Lusaka, Zambia.
Methodology: A cross sectional study involving 218 women aged between 15 and 49 years attending antenatal clinics at selected Hospitals. Eligible participants were recruited using systematic random sampling method and a structured interviewer administered questionnaire was used to collect the data which was later processed using Epi-Data and exported to STATA for analysis.
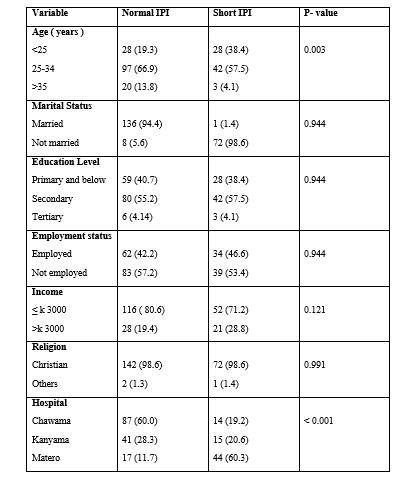
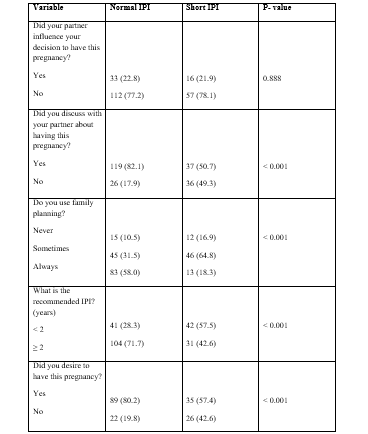
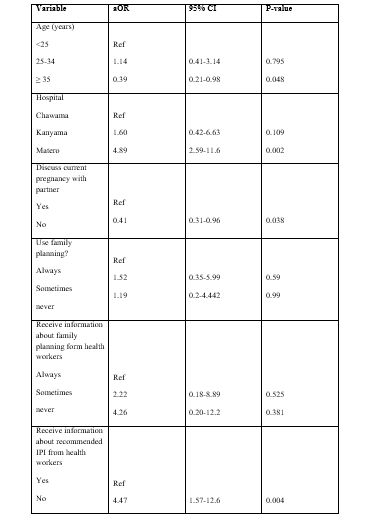
Results: The prevalence of short IPI’s was 33.4%. Among the factors associated with short IPI’s, it was noted that women aged 35 years or older were 61% (aOR=0.39; 95% CI: 0.21-0.98) less likely to have short IPI’s compared to those aged less than 25 years. Furthermore, women from Matero Hospital had 4.89 (95% CI; 2.59-11.6) times higher odds of short IPI’s than women from Chawama Hospital. In addition, women who reported having discussed the pregnancy with their partners were 59% (aOR=0.41; 95% CI; 0.31-0.96) less likely to have short IPI’s compared to those who did not discuss. For those women who indicated that they did not receive information about recommended IPI’s from health care workers, their odds of short IPI’s were 4.47% (95% CI; 1.57-12.6) times higher than those who received the information.
Conclusion: Raising awareness among women on the recommended birth intervals and encouraging partner participation on when to have the next child may help in efforts to avert the problem of short IPI’s and its effect on maternal and perinatal outcomes.
INTRODUCTION
The interpregnancy interval (IPI) is the spacing between a live birth and the beginning of the following pregnancy. After a live term birth, the World Health Organisation (WHO) recommends an IPI greater than 2 years and less than 5 years.[1] This recommendation is based on studies from across the globe which have shown that both short and long IPI have been associated with adverse pregnancy outcomes. However, the bulk of adverse effects has been linked with short IPI’s.[2] The IPI offers an opportunity to maximise on the woman’s health for better pregnancy outcomes.[3]
Optimal IPI can ensure optimal health for both the mother and infant, whereas sub-optimal IPI has been associated with several maternal and perinatal morbidity and mortality. Avoidance of short IPI’s can be achieved through postpartum provision of contraception, whereas avoidance of long IPI is more problematic since a desired pregnancy may be precluded by factors such as subfertility, availability of partner, economic and occupational issues, or illness.[4] If the IPI is short, the ability of the mother to recover from nutritional depletion after the previous pregnancy, mainly iron deficiency anaemia, is impaired and may result in entering the next pregnancy with low iron, vitamins and minerals.[5] In addition, the mother is at increased risk of maternal morbidities, including obesity, gestational diabetes, placental abruption[6] and premature rupture of membranes.[7] Short IPI has equally been linked to an increase in the risk of prematurity[8] , preterm labour[9] , low birth weight[10] , impaired foetal growth[11] , congenital anomalies[12] , autism spectrum disorders[13] and infant mortality.[14] So, in order to minimise these risks and achieve good reproductive health, the mother needs to be in a state of complete physical, mental and social wellbeing before becoming pregnant again.
Worldwide, birth interval practices differ widely. Particularly, women in developing countries often have shorter IPI’s than they would personally prefer.[15] The reason for short IPI is that many women in developing countries do not use contraception after birth and therefore are likely to become pregnant once fecundity returns. A variety of factors have been known to influence a woman’s IPI, these may include her personal characteristics and the health status of her previous child. Other factors are traditional practices, particularly breastfeeding habits, postpartum abstinence and cultural norms.[16] In addition, access and utilisation of reproductive health services has equally shown to contribute to women’s birth spacing practices.[15] In Zambia, 54% of married women residing in urban areas use contraception compared to 46% of women in the rural areas.[17] An experimental study conducted in an urban clinic in Lusaka district looked at contraceptive access and uptake among married women. It compared the influence of men (the heads of households) on the woman's decision to take up any form of contraception and subsequently avoid unwanted pregnancies.[15] The study concluded that households where men took control of family planning and contraceptive uptake had fewer incidences of unwanted pregnancies as compared to households where the women concealed contraceptive uptake. Therefore, couple involvement in family was found to be essential in lowering the incidence of unwanted pregnancies.
In Zambia, apart from lack of contraceptive uptake and access to family planning services, the other factors such as demographic, sociocultural and health care related factors which cause women to have short IPI have not been well explored despite there being enough information on print and electronic media with regards to family planning. Therefore, this study aimed to explore the predisposing factors for short IPI in Lusaka district, an urban setting where there is adequate access to information.
METHODS
This was a cross-sectional study conducted at three First-Level Hospitals in Lusaka: Kanyama, Matero and Chawama Hospitals. The target population was all pregnant mothers with short interpregnancy intervals accessing antenatal care at these First-Level Hospitals who met the eligibility criteria. A total of 218 participants were recruited using systematic random sampling method. An interviewer administered questionnaire was used to collect the data which was tailored to the study objectives. Both descriptive and inferential techniques of analysis were applied on the data using STATA version 14.2. A binary logistic model was used to assess the association between the predictor and the outcome variables. Variables with a P- value of ≤0.2 in bivariate analysis were entered in another model to conduct multivariate analysis. Statistical significance was considered at a level of 5% and an adjusted odds ratio along with a 95% confidence interval was used to present the estimates of the strength of associations.
RESULTS

DISCUSSION
This was facility based cross sectional study conducted in order to assess the prevalence and factors associated with short IPI among pregnant women at First-Level Hospitals in Lusaka district. As a result, the overall prevalence of short IPI (<24 months) among the pregnant women in this study was 33.4 %. The factors independently associated with short IPI were Age of the woman and Hospital, whether the woman had received information about the recommended birth intervals and if she had discussed her current pregnancy with her partner. The prevalence in this study was higher than the estimated national prevalence and the prevalence in Zimbabwe[18] , where about 15.8% and 11.2 % of women had short IPI respectively. This difference may be attributed to the sample population. Whereas the two studies were nationwide, this study focused only on a few urban Hospitals.
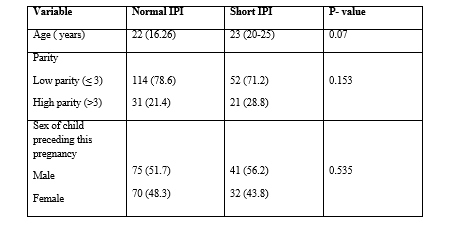
In this study, women aged 35 years or older were 61% less likely to have short IPI compared to those women aged less than 25 years. This is in keeping with a similar study conducted in Tanzania[19] where it was noted that IPI was shorter in younger women less than 20 years. This finding may be attributed to early marriages, high fertility rate and an unmet need for family planning in those less than 25 years old. A study by Ross and Winfrey[20] found that women at greatest risk for having an unmet need for family planning were young women below the age of 20 years. These women subsequently had short IPI. Another reason could be that fertility reduces with age above 35 years and older women could be having better ability to make independent decisions concerning their reproductive goals compared to younger women. The older women might have also been tending towards completing their family sizes and hence spacing their pregnancies more appropriately.
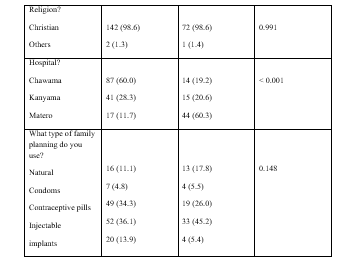
In addition, women from Matero First-Level Hospital had 4.89 times higher odds of short IPI than women from Chawama First-Level Hospital. This can be explained by possible lack of contraceptive health awareness in Matero as compared to Chawama townships, which may require further investigations. Lack of contraceptive use has been documented in literature as one of the strongest predictors of short IPI.[21] Contraceptives delay conception after a child birth and are one of the best practices that can lead to achievement of recommended birth intervals and therefore optimal maternal and child health outcomes.[22] We would expect that lack of contraceptive use would be a significant factor leading to short IPI, however this was not demonstrated in this study as only the minority (12.6%) of the respondents said they never used any form of contraception. Similar findings were reported in a study done in Democratic Republic of Congo which did not show any significant association between modern contraceptive use and child spacing.[23] Hence, more investigations need to be undertaken in Matero Township, where most of the study participants at Matero First-Level Hospital came from, in order to ascertain the true extent of the problem.
This study equally found that those women who discussed the decision to have the current pregnancy with their partners had less odds of having short IPI than those who did not. This could probably be due to the fact that women and couples who plan their pregnancy may follow the recommendations for child spacing and therefore end up with optimal IPI’s. It could be argued that proper communication between couples about reproductive goals has a positive outcome on birth spacing. The level of reproductive health decision making among couples such as when to have the next pregnancy, family size and family planning use among others can result in benefits which impact positively on the family in general.[24] This brings to light the importance of couple communication when it comes to family planning. Men who are the heads of households play a critical role in decision making and hence, influence the woman’s uptake of contraceptives. In addition, studies done in rural Uganda[25] and Saudi Arabia[26] found that lack of partner support was highly associated with short IPI.
Finally, women who did not receive information about recommended IPI’s were 4.47 times more likely to have short IPI compared to those who received information. This finding is higher than what was observed in a similar study conducted in Ethiopia[16] which revealed that mothers who had poor knowledge about optimal IPI were 3 times more likely to practice short IPI. This may be explained by the fact that having awareness about the disadvantages of short IPI and the advantages of optimal IPI for both mother and child makes them use modern contraceptives until the appropriate time. However, a study in Egypt found that there was no significant difference in IPI’s between a control group and an experimental group which was given information about the recommended birth interval and advantages of healthy birth spacing.[27]
CONCLUSION
According to the World Health Organization and the Zambian government, the recommended IPI should be between 2 to 5 years before attempting the next pregnancy after a live birth. However, despite this recommendation, this study found a higher proportion of women (33.4%) getting pregnant before the recommended period of time. Age of the woman, Hospital, whether the woman received information about recommended IPI and if she discussed her current pregnancy with her partner were independently associated with short IPI. Therefore, it implies that raising awareness among women on the recommended birth intervals and encouraging partner participation on when to have the next child might help in the efforts to avert the problem of short IPI. Besides, further studies need to be undertaken, with a larger sample size within the urban and rural setting, including those who attend antenatal clinics at private facilities so as to ascertain the true prevalence and determinants of short IPI.
DECLARATIONS
For the conduct of this research, approval was obtained from the Biomedical Research Ethics Committee of the University of Zambia School of Medicine (UNZABREC, reference number: REF 1440-2020). Permission was also sought from the National Health Research Authority (REF No. NHRA000012/30/03/2021) and the Lusaka district health management team. Data to support this study can be accessed upon request from the main investigator.
CONFLICT OF INTEREST: None
FUNDING DECLARATION
The Ministry of Technology and Science of the Republic of Zambia.
ACKNOWLEDGEMENTS
Dr. Patrick Kaonga, for the help rendered during the process of data analysis. All the medical staff from the participating Hospitals and all the women who voluntarily agreed to take part in this study.
REFERENCES
- World Health Organization. Report of a WHO Technical Consultation on Birth Spacing: Geneva, Switzerland 13-15 June 2005. World Health Organization; 2007. Accessed November 15, 2022. https://apps.who.int/iris/handle/10665/69855
- Conde-Agudelo A, Rosas-Bermúdez A, Kafury-Goeta AC. Birth spacing and risk of adverse perinatal outcomes: a meta-analysis. JAMA. 2006; 295(15):1809-1823. doi:10.1001/jama.295.15.1809
- Conde-Agudelo A, Rosas-Bermúdez A, Kafury-Goeta AC. Effects of birth spacing on maternal health: a systematic review. Am J Obstet Gynecol. 2007; 196(4):297-308. doi:10.1016/j.ajog.2006.05.055
- Thiel de Bocanegra H, Chang R, Howell M, Darney P. Interpregnancy intervals: impact of postpartum contraceptive effectiveness and coverage. Am J Obstet Gynecol. 2014; 210(4):311.e1-311.e8. doi:10.1016/j.ajog.2013.12.020
- Lubeya MK, Vwalika B. Anaemia in pregnancy among pregnant women in Lusaka District, Zambia. Med J Zambia. 2017; 44(4):238-243. doi:10.4314/mjz.v44i4
- Hutcheon JA, Nelson HD, Stidd R, Moskosky S, Ahrens KA. Short interpregnancy intervals and adverse maternal outcomes in high-resource settings: An updated systematic review. Paediatr Perinat Epidemiol. 2019; 33(1):O48-O59. doi:10.1111/ppe.12518
- DaVanzo J, Razzaque A, Rahman M. The Effects of Birth Spacing on Infant and Child Mortality, Pregnancy Outcomes, and Maternal Morbidity and Mortality in Matlab, Bangladesh. : 160.
- Fuentes-Afflick E, Hessol NA. Interpregnancy interval and the risk of premature infants. Obstet Gynecol. 2000; 95(3):383-390. Doi: 10.1016/s0029-7844(99)00583-9
- Adam I, Ismail MH, Nasr AM, Prins MH, Smits LJM. Low birth weight, preterm birth and short interpregnancy interval in Sudan. J Maternal-Foetal Neonatal Med Off J Eur Assoc Perinat Med Fed Asia Ocean Perinat Soc Int Soc Perinat Obstet. 2009; 22(11):1068-1071. Doi: 10.3109/14767050903009222
- Basso O, Olsen J, Knudsen LB, Christensen K. Low birth weight and preterm birth after short interpregnancy intervals. Am J Obstet Gynecol. 1998; 178(2):259-263. Doi: 10.1016/s0002-9378(98)80010-0
- van Eijsden M, Smits LJ, van der Wal MF, Bonsel GJ. Association between short interpregnancy intervals and term birth weight: the role of folate depletion. Am J Clin Nutr. 2008; 88(1):147-153. doi:10.1093/ajcn/88.1.147
- Chen I, Jhangri GS, Chandra S. Relationship between interpregnancy interval and congenital anomalies. Am J Obstet Gynecol. 2014; 210(6):564.e1-564.e8. doi:10.1016/j.ajog.2014.02.002
- Zerbo O, Yoshida C, Gunderson EP, Dorward K, Croen LA. Interpregnancy Interval and Risk of Autism Spectrum Disorders. Pediatrics. 2015; 136(4):651-657. doi:10.1542/peds.2015-1099
- McKinney D, House M, Chen A, Muglia L, DeFranco E. The influence of interpregnancy interval on infant mortality. Am J Obstet Gynecol. 2017; 216(3):316.e1-316.e9. doi:10.1016/j.ajog.2016.12.018
- Ashraf N, Field E, Lee J. Household Bargaining and Excess Fertility: An Experimental Study in Zambia. Am Econ Rev. 2014; 104(7):2210-2237. doi:10.1257/aer.104.7.2210
- Aleni M, Mbalinda SN, Muhindo R. Birth Intervals and Associated Factors among Women Attending Young Child Clinic in Yumbe Hospital, Uganda. Int J Reprod Med. 2020; 2020:1326596. doi:10.1155/2020/1326596
- Zsa ZSA, Moh M of H, Uth-Vl UTHVL, ICF. Zambia Demographic and Health Survey 2018. Published online January 1, 2020. Accessed November 15, 2022. https://dhsprogram.com/publications/publication-fr361-dhs-final-reports.cfm
- Rutstein SO. Trends in birth spacing. Published online September 1, 2011. Accessed November 15, 2022. https://dhsprogram.com/publications/publication-cr28-comparative-reports.cfm
- Sanga LA, Mtuy T, Philemon RN, Mahande MJ. Inter-pregnancy interval and associated adverse maternal outcomes among women who delivered at Kilimanjaro Christian Medical Centre in Tanzania, 2000-2015. PloS One. 2020; 15(2):e0228330. doi:10.1371/journal.pone.0228330
- John A. Ross WLW. Contraceptive Use, Intention to Use and Unmet Need during the Extended Postpartum Period. 2001; 27(1):20.
- Tessema GA, Zeleke BM, Ayele TA. Birth interval and its predictors among married women in Dabat District, Northwest Ethiopia: A retrospective follow up study. Afr J Reprod Health. 2013; 17(2):39-45. doi:10.4314/ajrh.v17i2
- Rutaremwa G, Kabagenyi A, Wandera SO, Jhamba T, Akiror E, Nviiri HL. Predictors of modern contraceptive use during the postpartum period among women in Uganda: a population-based cross sectional study. BMC Public Health. 2015; 15(1):262. Doi: 10.1186/s12889-015-1611-y
- Chirwa TF, Mantempa JN, Kinziunga FL, Kandala JD, Kandala NB. An exploratory spatial analysis of geographical inequalities of birth intervals among young women in the Democratic Republic of Congo (DRC): a cross-sectional study. BMC Pregnancy Childbirth. 2014; 14(1):271. Doi: 10.1186/1471-2393-14-271
- Schwandt HM, Skinner J, Hebert LE, Cobb L, Saad A, Odeku M. Inadequate birth spacing is perceived as riskier than all family planning methods, except sterilization and abortion, in a qualitative study among urban Nigerians. BMC Womens Health. 2017; 17(1):80. Doi: 10.1186/s12905-017-0439-2
- Muhindo R, Okonya JN, Groves S, Chenault M. Predictors of Contraceptive Adherence among Women Seeking Family Planning Services at Reproductive Health Uganda, Mityana Branch. Int J Popul Res. 2015; 2015:e574329. doi:10.1155/2015/574329
- Rasheed P, Al-Dabal BK. Birth interval: perceptions and practices among urban-based Saudi Arabian women. East Mediterr Health J Rev Sante Mediterr Orient Al-Majallah Al-Sihhiyah Li-Sharq Al-Mutawassit. 2007; 13(4):881-892.
- Abdel-Tawab N, Loza S, Zaki A. Helping Egyptian Women Achieve Optimal Birth Spacing Intervals through Fostering Linkages between Family Planning and Maternal/Child Health Services. Population Council; 2008. doi:10.31899/rh4.1136
Medical Journal of Zambia, Vol 50, 3
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.