Challenges of Imaging Obese Patients in General Radiography: A Qualitative Systematic Review to Guide the Training and Practice in Zambia
Osward Bwanga
Midlands University Hospital Tullamore, Radiology Department, Ireland
Mubanga Bwalya
St Francis Central Hospital, Katete and University of Lusaka, Zambia
DOI: https://doi.org/10.55320/mjz.50.1.350
Keywords:Challenge, Obese patient, Radiographer, Radiography Student, Zambia
ABSTRACT
Background: Obese patients are increasingly being referred for medical imaging examinations across the world. Obese patients require a modified standard of care to compensate for challenges caused by both technical and psychological issues related to their weight and body habitus. There have been research studies conducted on this issue, but no systematic review has brought the findings of these studies together to inform training and practice.
Aim: This study was aimed at synthesising primary studies on the challenges faced by radiographers and radiography students in imaging obese patients to guide the training and practice in Zambia.
Methods: This qualitative systematic review was conducted using the Enhancing Transparency in Reporting the Synthesis of Qualitative Research (ENTREQ) guidelines. Two databases (PubMed and ScienceDirect) were systematically searched to identify relevant literature. This was supplemented by other sources: radiography journals, grey literature, and cited references. Data from the included studies were assessed for quality, extracted, and synthesised using thematic analysis.
Results: Five studies were identified and included in this review. Following data analysis, four themes related to challenges faced in imaging obese patients in general radiography emerged: difficulties in communicating without causing psychosocial distress, manual handling risks, limitation of the equipment, and difficulties in positioning and determining the exposure factors for diagnostic radiographic images.
Conclusion: This review provides an in-depth understanding of the challenges faced by radiographers and radiography students in imaging obese patients. Strategies to enhance radiography training and practice have been identified to help educators and radiographers.
INTRODUCTION
There is an increase in the number of obese patients being referred for general radiography examinations for acute and chronic conditions globally.[1-2] The worldwide prevalence of obesity tripled between 1975 and 2016.[3] Obesity is defined by the World Health Organization (WHO) [3] as an abnormal or excessive fat build-up that might harm a person's health. Adult obesity is commonly classified using the body mass index (BMI). [1] It is determined by dividing an individual's weight in kilogrammes by the square of their height in metres (kg/m2). [3] Globally, 13% of people aged 18 and older were predicted to be obese in 2016. A study carried out in Zambia by Rudatsikira et al., [4] found that 14.2% of community-based adults in Lusaka were obese. In the Zambian radiography education system, bariatric radiography has been integrated into the curriculum. However, there are no simulation experiences of imaging obese patients to prepare students for real practice.
Obesity is a leading cause of noncommunicable diseases (NCDs).[2-5] NCDs kill 41 million individuals worldwide each year, accounting for 74% of all fatalities.[5] NCDs are responsible for 29% of all fatalities in Zambia.[6] Cardiovascular illnesses (heart attacks and strokes), malignancies, chronic respiratory disorders, and diabetes are the most common kinds of NCD.[5-7] NCDs contribute significantly to rising healthcare expenditures, which is an issue in Zambia.[6] According to the Zambian Ministry of Health (MOH), the number of NCDs is increasing, putting a strain on medical imaging services.[6] However, positioning, radiation exposure, manual handling, equipment limitations, communication, and general patient care provide significant challenges for radiographers and students when imaging obese patients.[2-9] This may result in missed diagnoses, nondiagnostic findings, cancellation of imaging examinations owing to weight restrictions on X-ray tables, scheduling of improper imaging examinations, and increased radiation exposure. [2-7] It's critical that radiographers are well-equipped to handle the difficulties posed by imaging obese people.
Obese patients place additional needs upon medical facilities and equipment and create technical challenges.[10] To date, reviews on this topic have consisted of literature reviews, [1-11] and not a systematic review. Furthermore, the reviews were conducted 7 and 4 years ago respectively. Since then, a few primary qualitative studies have been published on this subject. Therefore, this study was aimed at synthesising primary studies on the challenges faced by radiographers and radiography students in imaging obese patients. A thorough grasp of this subject can aid in developing ways to improve radiography training and practice.
METHODS
This qualitative systematic review was carried out in accordance with the Enhancing Transparency in Reporting the Synthesis of Qualitative Research (ENTREQ) guidelines.[12] The stages included the formulation of a review question, stating the eligibility criteria, literature search, critical appraisal, data extraction, and data synthesis and analysis.
Review Question- The following was the review question:
“What are challenges faced by radiographers and radiography students in imaging obese patients in general radiography?”Eligibility Criteria- The inclusion criteria for this study were primary studies that have investigated challenges faced by radiographers and radiography students in imaging obese patients in general radiography, published in English. The study design was restricted to qualitative and mixed methods research studies as per the aim of the review. However, the reviewers excluded quantitative studies, and studies conducted on radiation therapists. Time restrictions were removed due to a lack of relevant studies conducted on this subject.
Literature Search and Outcome- A systematic search of the literature in databases and other sources: radiography journals, grey literature, and cited references was performed in November and December 2022. The electronic searches were performed in two (2) databases: PubMed/MEDLINE and ScienceDirect as most radiography publications are published in these databases. The key terms were derived from three categories based on the population (radiographers and radiography students), exposure (imaging of obese patients), and outcome or themes (challenges). The database searches were complemented by searching in journals: Radiography (UK), Journal of Medical Radiation Sciences, and the Journal of South African Radiographers. The searches were extended to the titles of citations in the reference lists of relevant journal articles.
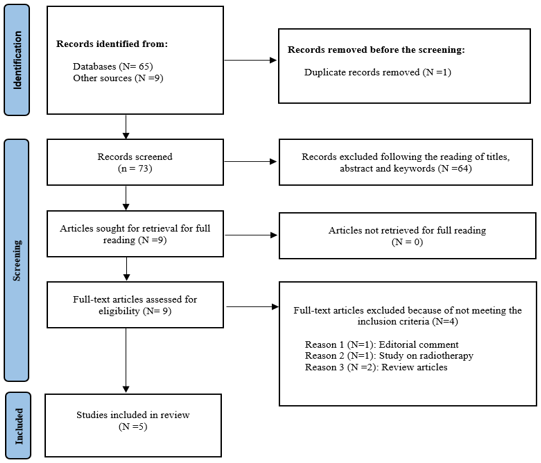
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) criteria were used to guide the literature search and article selection process: identification, screening, eligibility, and inclusion. [13] The search provided 73 records, and the screening of titles/abstracts/keywords narrowed the results down to nine (9) articles for full-text assessment. Four (4) articles were excluded: an editorial comment,[14] a study on radiotherapy, [15] and two (2) reviews.[1-11] The final pool for this review included five (5) primary studies.
Critical appraisal- The reviewers used the Critical Appraisal Skills Programme (CASP) Checklist for qualitative studies [16] to assess the quality of the included five (5) studies independently. Any differences were resolved by common agreement. The scoring of the checklist was standardised and set by both reviewers before the commencement of the review. The assessed study was rated high when it met at least a score of 7, medium with a score of 6 to 4, and low with a score of 3 or less. In addition, 1 was scored if the answer is “Yes” and 0 for “Unclear” and “No”. Table 1 shows the outcome of critical approval.

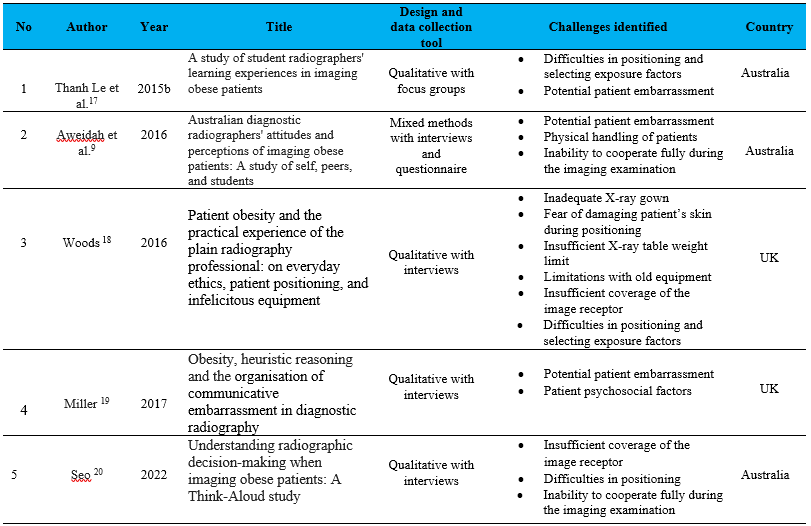
Data extraction- Data was extracted from all included studies by two reviewers. The data extracted included: author (s), year of publication, the title of the study, study design and data collection tool used, challenges identified, participants’ quotes, and country where the study was carried out. Table 2 shows the characteristics of included studies (N = 5).
Data synthesis and analysis- It was carried out manually using a three (3) stage thematic analysis for qualitative systematic reviews developed by Thomas and Harden. [21] In the first step, the extracted data was coded “line-by-line” by the main reviewer. In the second step, initial similar codes were grouped together into “descriptive themes”. In the final stage, “analytical themes” were produced. The process of data synthesis and analysis was reviewed by the second reviewer to enhance the credibility of data synthesis and analysis.
RESULTS
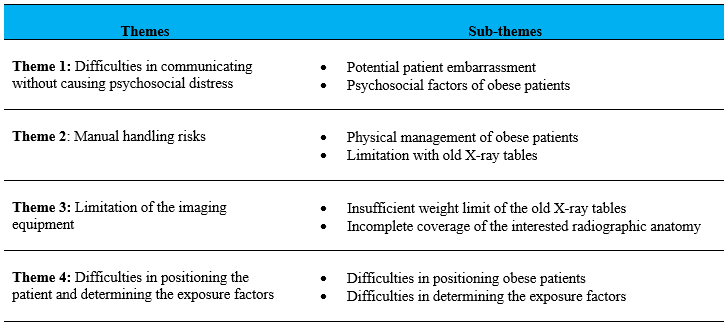
Four (4) themes and eight (8) sub-themes emerged from the data analysis (Table 3).
Theme 1: Difficulties in communicating without causing psychosocial distress
In two studies, [18-19] participants reported finding it difficult to communicate with obese patients without causing psychosocial distress due to their large body habitus. This theme has two sub-themes: potential patient embarrassment and psychosocial factors of obese patients.
Sub-theme 1: Potential patient embarrassment
When patients' weight exceeded the limit for the X-ray table, participants reported experiencing difficulty communicating without appearing to discriminate against them. This often occurred when the referring department did not communicate beforehand, which put the radiographers in a difficult predicament.“If they are obese and approaching that X-ray table limit, have to explain to them that you might need to wait for the only table that will take the excess weight. And, how to approach that without appearing to discriminate against the patient?” ([19] , p131)
In one study,[18] participants reported embarrassing moments when the normal-size X-ray gown failed to fit an obese patient or asked to wear an extra-large size that is different from other patients.
“Even down to X-ray gowns, they're not big enough for obese patients, and you end up having to X-ray them in their own clothes which sometimes can be ok but sometimes not appropriate, and if you sort of give them a gown and it's not big enough it just makes them feel embarrassed.” ([18] , p121)
“We've had bigger gowns made, so we've got a supply of those and then the patient is unaware that they're any different from anyone else.” ([18] , p121)
Participants understood the importance of maintaining patient dignity in the provision of quality medical imaging services. However, inappropriate X-ray gowns were reported as a hindrance to preserving the dignity of obese patients.
Sub-theme 2: Psychosocial factors of obese patients
One study [19] reported the effect of psychosocial factors on obese patients. Obese patients can develop a negative attitude toward radiographers and students due to perceived prejudice and discrimination by healthcare professionals. Participants reported this as a challenge:“Some obese patients are not understanding, and they can get quite offhand, which can be trickier to deal with…you just have to really be…polite, professional and just you know, try not to cause any offense.” ([19] , p132)
Good communication and upholding professionalism emerged as the most effective approach to overcoming this obstacle and preventing further psychological suffering in obese patients with a negative attitude toward staff.
Theme 2: Manual handling risks
Two studies[9-18] revealed manual handling concerns to radiographers and students, as well as the safety of obese patients when getting on and off the X-ray table. Participants testified that the physical handling of obese patients puts them at increased risk of musculoskeletal injuries. This theme has two sub-themes: physical management of obese patients and limitations with old X-ray tables.
Sub-theme 1: Physical management of obese patients
Difficulties in placing the image receptor for obese patients requiring an anterior-posterior (AP) chest X-ray on the trolley or bed were reported in one study.[18] It emerged that obese patients develop skin conditions and extra care should be taken when positioning or handling them to prevent damaging their skin.“One of the biggest problems we've had, is if you consider a patient who comes for a chest X-ray, and they are large…actually sitting the patient forwards and trying to put the cassette behind them … there's physically not a gap between the bed and the patient, so you're almost trying to push the cassette in and you could hurt them if you don't do it properly.” ([18] , p121)
Participants described radiography as a physical job because it involves moving patients and equipment. This puts radiographers and students at considerable risk of musculoskeletal injuries. This is even worse when dealing with obese patients who may have limited mobility.
“Generally, it's a bit frustrating … being a radiographer is quite a physical job with manual handling of the patients and having an obese patient that isn’t very cooperative makes our job quite difficult.” ([9] , p260)
Sub-theme 2: Limitation with old X-ray tables
Recently, imaging equipment manufacturers are considering obese patients when designing X-ray tables. However, participants reported facing difficulties with the transfer of obese patients from the chair to the old X-ray tables with limited height adjustments: “Some of the older equipment doesn't drop down as far, as low to the ground as the newer stuff, so if you've got one that will drop down a bit lower it means that larger patients are easier to transfer from a chair onto the table, whereas at the moment they might struggle” ([18] , p121). Such medical imaging equipment can also put radiographers and students at increased risk of developing musculoskeletal injuries.Theme 3: Limitation of the imaging equipment
Limitation of the imaging equipment was reported as one of the challenges faced by radiographers and students in imaging obese patients. This theme had two sub-themes: insufficient weight limit of the X-ray table and incomplete coverage of the interested radiographic anatomy.
Sub-theme 1: Insufficient weight limit of the X-ray table
In one study, [18] described participants’ experiences of insufficient weight limits of the X-ray table to accommodate obese patients. This challenge was experienced with old imaging equipment with a weight limit of below 250 kilograms (Kg). It was reported that the X-ray table limits have been increased to 250 kg with modern medical imaging equipment by manufacturers to accommodate obese patients: “We’ve had a few patients over the years that have been too heavy for the X-ray table, generally it means we can't move the tabletop or any of the table functions” ([18] , p121). This was described as a risk because a tabletop can break and cause injury to the patient. In addition, this can damage the motors whose function is to raise and lower the X-ray table.
Sub-theme 2: Incomplete coverage of the interested radiographic anatomy
The adaption of routine imaging practice for obese patients to cover the area of interest was reported in two studies. [18-20] The abdomen was the most examination identified where modification of the standard radiographic technique was required: “The larger the patient, the more likely the bowel is going to be expanded. You would certainly consider that you wouldn’t necessarily get all the anatomy in one exposure for abdominal X-ray” ([20] , p18). Two methods of technique modification were identified: taking two images (upper and lower abdomen) with the image receptor in a landscape and four images to include each quadrant.
“Even the largest cassette (35 by 43) isn't big enough for an obese abdomen. You might have to do it in four separate parts with sort of joining up the images together.”([18] , p122)
“For an obese patient, I would generally be using two shots in the landscape.” ([20] , p19)
Participants reported that taking multiple exposures to completely cover the interested radiographic anatomy increases patient radiation dose. This was a challenge in adhering to the as low as reasonably achievable (ALARA) principle. The modification of the technique was also described as demanding and time-consuming.
Theme 4: Difficulties in positioning the patient and determining the exposure factors
Three studies [17,18,20] reported the challenges faced by radiographers and students in positioning and determining the exposure factors for obese patients. Participants reported having challenges with technical factors which determine the radiographic image's quality.
Sub-theme 1: Difficulties in positioning obese patients
Participants reported that obese patients often suffer from co-morbidities related to their weight and body habitus which makes it difficult for them to move easily. One participant had this to say: “Sometimes large patients are awkward in their movements and so it can be a little bit hard for them to adjust that. You need to allow them a little bit more time to be able to get into the position” ([20] , p20). Another participant added: “The main difficulty is if they struggle to move into the position that we need, sometimes you've got to compromise a little bit” ([18] , p122). Participants also reported finding it difficult to palpate and identify bony landmarks used in positioning. For example, iliac crests for the abdomen. One student said: “It is hard to find anatomical landmarks with obese patients” ([17] , p64). However, these challenges were overcome with bariatric radiography training and experience:
“Obviously the more training you have, the better you are going to be at positioning without using bony landmarks.” ([18] , p121)
“With experience, you can do it partly by eye, can't you?” ([18] , p121)
Sub-theme 2: Difficulties in determining the exposure factors
The reviewed studies reported that obese patients need more exposure to have a diagnostic radiographic image. Determining the exposure factors [Kilovoltage (kVp) and Milliampere-second (mAs)] for the imaging examination while keeping the dose as low as reasonably achievable (ALARA) was reported as a challenge. To overcome this challenge, students reported using automatic exposure control (AEC) which is an inbuilt facility employed to determine appropriate mAs. “I find it hard choosing an exposure for these kinds of patients. Like, you’re not given a guideline and a lot of placement centres use a different exposure and it depends on a machine, and I wouldn’t know what to use on an obese patient. Except to use AEC” ([18] , p63). Radiographers and students found AEC a useful device for determining exposure factors for obese patients to avoid underexposure images and repetition of exposures.
DISCUSSION
This study revealed several challenges experienced by radiographers and students when imaging obese patients. Obesity is becoming a worldwide public health issue.[3] This has implications for medical imaging in terms of the increased workload associated with a variety of obesity-related co-morbidities, such as NCDs.[2] As a result, rather than reacting to circumstances as they happen, it is critical that radiographers and students are well-prepared to manage obese patients. [2-22] According to the College of Radiographers, [22] radiology departments should have guidelines for managing obese patients: informing the department of any obese patient referral, manual handling, and overall patient care. This ensures that obese patients receive efficient and seamless imaging services free from problems or delays.
Difficulty in communicating with obese patients without causing embarrassment was one of the challenges identified in this review. Literature has reported negative attitudes toward obese patients from healthcare professionals. In a survey carried out by Sobczak and Leoniuk [23] , 48.4% of medical professionals indicated having witnessed staff’s negative attitude toward obese patients. In another study conducted by Sagi-Dain et al.,[24] about 59% of patients reported disrespect from healthcare professionals. This can lead to psychological distress for obese patients who may already have low self-esteem and reluctance to engage with staff due to fears of embarrassment. [2] Therefore, to obtain the complete participation of their patients and maximise the likelihood of a successful imaging examination, students and radiographers should always be polite and communicate effectively.
Another challenge identified in this review was manual handling risks. In the radiology department, the manual handling of patients puts radiographers and students at considerable risk of musculoskeletal injuries.[22] The Occupational Health and Safety Act of 2010 of the Republic of Zambia, [25] requires employers to provide a safe working environment for employees. This includes providing mechanical lifting (bariatric) equipment. There is evidence that the use of mechanical lifting (bariatric) equipment is effective in reducing the incidence of musculoskeletal injuries to staff. [22-26] However, underdeveloped nations find it difficult to buy bariatric equipment owing to limited resources. Developing countries such as Zambia are still struggling to modernise imaging equipment where 60% is old and obsolete. [8,27,28] The bariatric equipment includes hoists, wide wheelchairs, and larger and wider trolleys/beds. Our review also found that radiographers and radiography students were afraid of damaging the patient’s skin. To address this issue, the College of Radiographers [22] recommends taking extra precautions while dealing with obese patients, who frequently suffer from skin excoriation, rashes, and ulcers.
The other challenges identified in this review were the old X-ray table's insufficient weight limit and incomplete anatomy coverage. X-ray tables have a weight limit, and this must not be exceeded to avoid breaking the table and injuring the patient. The table weight limits will also reduce when the motors are being used to raise and lower the table. [2] For this reason, radiographers and radiography students should be aware of the X-ray table limit. Generally, manufacturers write the weight limit on the front side of the table. It is good practice to write the table weight limit in the imaging control room for quick reference. In the last decade, the X-ray table limits have been increased to accommodate the bariatric population.[11] When purchasing new imaging equipment, it is important to consider modern equipment with a limit of 250 kg sufficient for all patients.[2] Imaging of the abdomen can be challenging also if the patient exceeds the image receptor standards sizes of 35 by 43 or 43 by 43. To overcome this challenge, radiographers in our review recommended modification of the standard imaging practice by imaging the abdomen in two- or four-parts using landscape orientation. This finding agrees with the literature.[1-2]
Difficulties in positioning the obese patient were another challenge identified in this review. Obese patients often suffer from a number of co-morbidities associated with their weight and body habitus such as oedema and dyspnoea which might affect their ability to cooperate fully during an examination. [22] This is physically challenging to radiographers and students and time-consuming in busy departments. In addition, this review found that it was challenging to palpate anatomical landmarks used when positioning and centering obese patients due to extensive fat, especially for abdomen examinations. To overcome these challenges, Thanh Le et al.,[1] recommends the use of the patient’s elbow joint to approximate the level of the iliac crest which is the landmark used when centering for the abdomen.
The last challenge identified in this review was difficulties in determining the exposure factors for obese patients. This finding agrees with Whitley et al., [2] who pointed out that it is very difficult to assess the extra exposure required for an obese patient using manual exposure factors, especially for abdominal and lumber spine X-rays. Due to their weight, obese patients need an increase in kVp and mAs to obtain better image quality. [11-22] However, increasing the kVp for improved penetration of X-rays increases the radiation dose to the patient.[26-29] However, as obese patients frequently struggle to hold their breath, an increase in mAs will result in a longer exposure duration with the potential for motion artifacts. [22] The use of AEC, grid, tight collimation, and compression of the region of interest are other methods for enhancing image quality that has been documented in the literature. [2-22] With training and practice, radiographers and radiography students can provide high-quality radiographic images for obese patients, according to the findings of our review.
LIMITATIONS OF THE STUDY
The findings of our review are only as reliable as the findings reported in each of the included studies.[30] The other limitation is a limited number of studies (N=5) conducted on this subject and included in the review. Despite these limitations, the findings of this qualitative systematic review provide an in-depth understanding of the challenges faced by radiographers and students in imaging obese patients using the available literature.
CONCLUSION
This review has provided a better understanding of the challenges faced by radiographers and students in imaging obese patients during general radiography. Practical and psychosocial challenges related to obese patients arise due to their weight and body habitus. To overcome this and acquire high-quality radiographic images, a change in normal imaging technique is necessary. This comes with training and expertise in bariatric radiography. It is important for educators to prepare radiographers through adequate academic and practical training. This can include offering a postgraduate course in bariatric radiography. Employers should also support radiographers with bariatric equipment to circumvent musculoskeletal injuries.
COMPETING INTEREST
The reviewers declare no conflict of interest.
AUTHORS’ CONTRIBUTIONS
The main reviewer, Osward Bwanga conceptualised this review, extracted and analysed the data, and prepared the manuscript for publication. Mubanga Bwalya assisted the main reviewer to search for the literature, assessment of the quality of the identified studies, extracting the data, performing member checking, and preparing the final manuscript.
REFERENCES
- Le NTT, Robinson J, Lewis SJ. Obese patients and radiography literature: what do we know about a big issue? J Med Radiat. 2015a; 62: 132- 141.
- Whitley AS, Jefferson G, Sloane KHC, Anderson G, Hoadley G. Clark’s positioning in radiography. 13th ed. London: CRC Press Ltd; 2015.
- World Health Organisation. Obesity and overweight; 2021. From https: //www. who. int/ news-room/fact-sheets/detail/obesity-and-overweight (Accessed 20 December 2022).
- Rudatsikira E, Muula AS, Mulenga D, Siziya S. Prevalence and correlates of obesity among Lusaka residents, Zambia: a population-based survey. Int Arch Med. 2012;5(1):14. doi:10.1186/1755-7682-5-14.
- World Health Organisation. Noncommunicable diseases; 2022. From https: //www. who.int/ news-room/fact-sheets/detail/obesity-and-overweight (Accessed 15 December 2022).
- Ministry of Health. Prevention and control of non-communicable diseases in Zambia-The case for investment. Lusaka: The Ministry of Health; 2016.
- Glanc P, O'Hayon BE, Singh DK, Bokhari SA, Maxwell CV. Challenges of pelvic imaging in obese women. Radiographics. 2012 Oct;32(6):1839-62. doi: 10.1148/ rg.326125510. PMID: 2306517
- Ministry of Health. National health strategic plan 2017-2021. Lusaka: The Ministry of Health; 2017.
- Aweidah L, Robinson J, Cumming S, Lewis S. Australian diagnostic radiographers' attitudes and perceptions of imaging obese patients: A study of self, peers and students. Radiography 2016; 22: e258-e263.
- Carucci LR. Imaging obese patients: problems and solutions. Abdom Imaging. 2013 Aug;38(4):630-46. doi: 10.1007/s00261-012-9959-2. PMID: 23008055.
- Uppot RN. Technical challenges of imaging and image-guided interventions in obese patients. Br J Radiol. 2018;91(1089):20170931. doi:10.1259/bjr.20170931
- Tong A, Flemming K, McInnes E, Oliver S, Craig J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Medical Research Methodology, 2012;12 (181). doi: 10.1186/1471-2288-12-181. PMID: 23185978; PMCID: PMC3552766.
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline. 2015. Available from http://www.prisma-statement.org/ (accessed on 12 December 2022).
- Alqahtani SJ, Knapp KM. Imaging patients with obesity. J Med Radiat Sci. 2022;69(1):3-4. doi:10.1002/jmrs.560
- Winters E, Poole C. Challenges and impact of patient obesity in radiation therapy practice. Radiography (Lond). 2020 Aug;26(3):e158-e163. doi: 10.1016/j.radi. 2020.01. 005. Epub 2020 Feb 4. PMID: 32052747.
- Critical appraisal skills programme (CASP) checklist for qualitative research. 2018. From https://casp-uk.net/casp-tools-checklists/(Accessed on 18 November 2022).
- Thanh Le NT, Robinson J, Jayne Lewis S. A study of student radiographers' learning experiences in imaging obese patients. J Med Imaging Radiat Sci. 2015b Sep;46 (3S) :S61-S68.e1. doi: 10.1016/j.jmir.2015.05.002. Epub 2015 Jul 17. PMID: 31052110.
- Woods AL, Miller PK, Sloane C. Patient obesity and the practical experience of the plain radiography professional: on everyday ethics, patient positioning and infelicitous equipment. Radiography 2016; 22: 118-123.
- Miller PK, Woods AL, Sloane C, Booth L. Obesity, heuristic reasoning and the organisation of communicative embarrassment in diagnostic radiography. Radiography. 2017 May;23(2):130-134. doi: 10.1016/j.radi.2016.12.002. Epub 2017 Jan 6. PMID: 28390544.
- Seo G, Robinson J, Punch A, Jimenez Y, Lewis S. Understanding radiographic decision‐making when imaging obese patients: A Think‐Aloud study. J Med Radiat Sci. 2022; 69: 13–23. 10.1002/jmrs.543
- Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008 Jul 10;8:45. doi: 10.1186/1471-2288-8-45. PMID: 18616818; PMCID: PMC2478656.
- College of Radiographers. Bariatric patients: guidance and advice for the radiography workforce. London: The College of Radiographers; 2013.
- Sobczak K, Leoniuk K. Attitudes of medical professionals towards discrimination of patients with obesity. Risk Manag Healthc Policy. 2021;14:4169-4175. Published 2021 Oct 7. doi:10.2147/RMHP.S317808
- Sagi-Dain L, Echar M, Paska-Davis N. Experiences of weight stigmatization in the Israeli healthcare system among overweight and obese individuals. Isr J Health Policy Res.2022; 11 (5). https://doi.org/10.1186/s13584-022-00518-9
- Republic of Zambia. Occupational Health and Safety Act of 2010 of the Republic of Zambia. Lusaka: Government printers; 2011.
- Ehrlich RA, Coakes DM. Patient care in radiography: with an introduction to medical imaging. 10th ed. London: Elsevier; 2020.
- Ng'andwe EM, Bwanga O. Factors affecting the ability of radiographers to deliver imaging services in rural parts of Zambia. Radiography. 2022;28(3):758-765. doi: 10.1016/j.radi.2022.03.005. Epub 2022 Apr 2. PMID: 35379554.
- Bwanga O, Chanda E. Challenges in radiation protection in healthcare: A case of Zambia. EAS Journal of Radiology and Imaging Technology. 2020; 2(1):7-14.
- Bwanga O. Causes of reject and repeat of digital radiographic images: a literature review to guide the practice of radiography in Zambia. Medical Journal of Zambia, 2021; 48(1):38 - 45. https://doi.org/10.55320/mjz.48.1.766
- Bwanga O. How to conduct a qualitative systematic review to guide evidence-based practice in radiography. International Journal of Sciences: Basic and Applied Research. 2020; 52 (1): 205-213.
Medical Journal of Zambia, Vol 50, 1
The Medical Journal of Zambia, ISSN 0047-651X, is published by the Zambia Medical Association.
© This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.