Correlates of Hypertension among Persons Living with HIV at Livingstone Central Hospital: A Crosssectional study
Authors
Sody M. Munsaka University of Zambia, School of Health Sciences, Department of Biomedical Sciences, Lusaka, Zambia
Benson M. Hamooya Mulungushi University, School of medicine and Health Sciences, Livingstone, Zambia
Musalula Sinkala University of Zambia, School of Health Sciences, Department of Biomedical Sciences, Lusaka, Zambia
Malan Malumani Mulungushi University, School of medicine and Health Sciences, Livingstone, Zambia
Mulungushi University, School of medicine and Health Sciences, Livingstone, Zambia
Sepiso K. Masenga Mulungushi University, School of medicine and Health Sciences, Livingstone, Zambia
Background: Persons living with HIV (PLWH) are more likely to develop hypertension and cardiovascular disease than the HIV-negative population. The new hypertension guidelines by the American Heart Association (AHA) and the American College of Cardiology (ACC) lowered the definition of hypertension from systolic and diastolic blood pressure (BP) of.?: 140/90mmHg to .?:
130/80, respectively. This study was aimed at determining the prevalence and factors associated with hypertension in PL WH in Livingstone using the new hypertension diagnostic criteria.
Methods: This was a cross-sectional study. We recruited 226 antiretroviral treated PLWH attending routine visits. Socio-demographic, health and clinical data including BP readings were collected. Interviewer-structured questionnaires adapted from
the World Health Organization Stepwise approach to Surveillance (WHO STEPs) and the international physical activity questionnaire (IPAQ) were used to collect data. Statistical evaluations were employed to elucidate relationships between hypertension and all response variables.
Results: The prevalence of hypertension using the old and new guidelines was 16% and 42%, respectively. Factors significantly associated with increased and reduced odds of developing hypertension after adjustments in multivariate logistic regression were age, body mass index (BMI), employment status, fasting blood sugar (FBS) and table salt consumption, respectively (p<0.05 for all). Using the new AHA/ACC criteria for hypertension shifted the prevalence from 16% ( old criteria) to 42%.
Conclusion: The prevalence of hypertension in PLH in Livingstone was 42% and the major risk factors associated with hypertension in PLWH wereincreasing age, BMI and FBS. We recommend the inclusion of FBS in routine measurements in PLWH. The AHA/ ACC new guidelines should be reenforced in low-cost settings to increase the treatment of hypertension among PL WH.
INTRODUCTION
Susceptibility to non-communicable diseases (NCDs), such as hypertension, is a rising challenge facing persons living with HIV (PLWH), especially in low-income countries1 Collection of comprehensive baseline information that elucidates the underlying health risk factors associated with hypertension is critical for patient quality care, identification, and management of associated cardiovascular risk factors1, 2. Many of the risk factors can be measured during routine clinic visits. This is of particular importance in sub-Saharan Africa where the burden of NCDs is high in PLWH3
In 2017, a report on clinical practice guidelines from the American College of Cardiology (ACC) and the American Heart Association (AHA) Task Force was released to aid in hypertension diagnosis and management4. For many years, systolic and diastolic blood pressure (SBP/DBP) categories of below 120/80 mmHg, 120-139/80-89 mmHg and 140/90 mmHg or higher defined normal, pre-hypertension and hypertension, respectively5. However, according to the new classification, the SBP/DBP reading categories of below 120/80 mmHg, 120- 129/<80 mmHg and 130/80 mmHg or higher define normal, elevated blood pressure (BP) and hypertension 4. Furthermore, the new guidelines also provide new treatment recommendations, including lifestyle changes to manage elevated blood pressure and hypertension4 Among lifestyle and social-economic factors pertinent to hypertension, management are diet, smoking, physical inactivity, being divorced/widowed, and lower education 6 - 8. However, data based on new hypertension guidelines that report on the prevalence and factors associated with hypertension among PLWH living in sub-SaharanAfrica is scarce.
We conducted a cross-sectional analytical study to determine the prevalence and risk factors associated with hypertension in PLWH. Furthermore, focusing on Zambia's health care, we were seeking to provide epidemiological data and compare these data to those collected in other countries. The study aimed: 1. to determine the prevalence of hypertension in PLWH in Livingstone, Zambia using the new AHA/ ACC guidelines; 2. to determine routinely and non-routinely collected factors associated with hypertension in PLWH.
METHODS
Study design and Setting
We conducted a cross-sectional analytical study at Livingstone Central Hospital (LCH), the largest referral hospital ( and hosting the largest ART clinic) in the Southern Province of Zambia. The antiretroviral therapy (ART) Clinic offers ART and general medical services to the community, with approximately 3,800 PLWH enrolled in ART.
Participants
Participants were enrolled from the ART clinic during their regular attendance to these services.
Eligibility criteria
We included all adults aged 18 years and above living with HIV. Study participants were only recruited after verbally consenting and signing a consent form. We excluded patients seeking healthcare due to an acute illness rather than routine ART clinic reviews and participants who were currently taking antihypertensive medication for purposes of BP classification. Participants with a history of antihypertensive medication but who had not taken their medication for ≥ 2 weeks were included in the study and classified as hypertensive.
Sample size estimation
We used OpenEpi online software (sample size for a proportion or descriptive study) to compute a total sample size of 226 using an estimated prevalence of hypertension of 19.3% (local quarterly monthly records) at 95% significance level and 80% power in an ART population of 3776. The formula is stipulated below:
Sample size (n) = [DEFF*Np(l-p)] / [(d2/Z21- a/2*(N-l)+p*(l-p)]; where N is the population size; p is hypothesized % frequency of outcome factor in the population; d is Confidence limits as % of 100 (absolute+/-%, which is 5%); DEFF is the design effect.
Study variables
The primary response variable was hypertension. The diagnosis of hypertension for participants was initially based on the history of antihypertensive usage and BP readings of 140/90 mmHg or higher according to the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7)5. However, in this study, we used the new AHA/ ACC criteria for hypertension as a BP reading of 130/80 mmHg or higher 4.
Explanatory variables included:
Social demographic characteristics such as age, gender, marital status, employment status, and highest education attained.
Physical activities and dietary lifestyle: daily physical activity, minutes of weekly vigorous and moderate activity, minutes of weekly walking activity, minutes spent seated every weekend and weekday, days per week with fruit intake, days per week with vegetable intake, the addition of salt at the table and while cooking, processed salt intake (intake of salt from processed foods), current alcohol consumption, current or past smoker.
Clinical factors: BMI (weight in kg/height in meters2), waist circumference, duration on ART, ART regimen, use of antihypertensive medication, pulse, pulse pressure [ defined as systolic BP (SBP) minus diastolic BP (DBP)], mean arterial pressure (MAP) ( defined as DBP plus one third pulse pressure), mid-BP (sum ofSBP and DBP, divided by 2), CD4 counts, HIV RNA viral load, fasting blood sugar (FBS), diabetes risk scores, diabetes risk category. Diabetes risk scores were calculated using the International Diabetes Federation (IDF) risk assessment form as previously described elsewhere.
BP measurements
We used the WGNBPA 730 (USA) and SBM 67 (Germany) BP monitors for measurements. For standard measurements, we adapted the new AHA/ ACC guidelines : The patients had not been exercising, smoking, or drinking caffeine, their bladders were empty, and they were seated for more than 30 minutes before measurements were taken in a still position. The limb used to measure BP was supported ensuring that the BP cuff was at heart level. During the measurements, the participants were asked to sit upright, back straight, with feet flat on the floor without legs crossing each other. Three readings were taken and averaged. The average BP was used to reflect the person's BP. Routine BPs taken by attending nurses did not take into account the consideration explained above. Furthermore, our measured BP values were compared to the BP measurements taken by attending nurses during routine visits as reported in the patients' health records25.
Hypertension diagnosis wasbased on the history of antihypertensive drugs ( where hypertensive patients did not take antihypertensive drugs for 2 weeks to satisfy the eligibility criteria) except for four participants where we used BP readings taken on 2 or more occasions (from records) which were consistent with the standard measure news we took. The new diagnosis of hypertension using the AHA criteria for participants with no history of antihypertensive medication usage was based on BP readings taken on 2 occasions.
Antihypertensives
Most participants with a history ( 2 weeks) of using antihypertensive medication were using two antihypertensive drugs, a calcium channel blocker (Amlodipine or Nifedipine) and an Angiotensinconverting enzyme inhibitor (ACE) (Enalapril or Losartan) or a Diuretic (Furosemide or Moduretic).
Data sources/ measurement
For data collection, we used the interviewer structured questionnaire adapted from the WHO STEPs (World Health organization's STEPwise Approach to Surveillance), the international physical activity questionnaire (IPAQ), and the IDF type 2 diabetes risk assessment forms described in our previous study9. These were translated into the local language (Tonga) for participants that could not speak English.
Data analysis
Since data were not normally distributed (p-value < 0.05 , Shapiro-Wilk's test for all continuous variables categorized by hypertension status), we used the non-parametric test Mann-Whitney to compare medians (interquartile range) of continuous variables between normotensives and hypertensives. For categorical variables, we used Chi-Square or Fishers' exact test where appropriate. We selected known risk factors for developing hypertension and variables significant in univariate logistic regression were included in the multivariate logistic regression model. We reported odds ratios (OR), adjusted odds ratios (AOR), and confidence limits at 95%. We used descriptive statistics to compare the proportion of participants in each BP category and hypertension status between JNC 7 and the new AHA/ ACC criteria. To compare routine BP measurements taken by attending nurses and standard BP measurements, we used MannWhitney and non-parametric Spearman correlation coefficient to assess the strength of association. We also reported median differences and their confidence limits (95%).
Age, WC, BMI, and diabetes risk were also categorized to ease interpretation.P values less than 0.05 were considered significant and are shown in bold. We used SPSS statistical software for data analysis.
RESULTS
General characteristics of participants
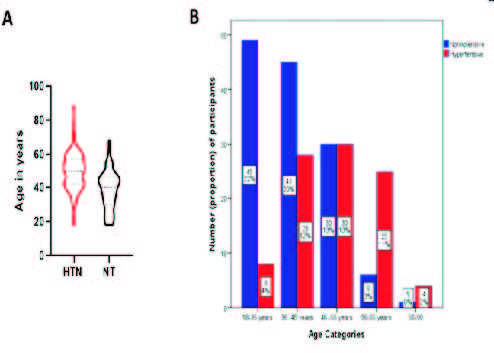
We found that the prevalence of hypertension in the study population was 42% as determined using the new AHA/ ACC criteria and 16% as determined using the JNC 7 criteria (Table 1 ). The age range was 18 to 88 years old and 66% werefemale(n, 149)
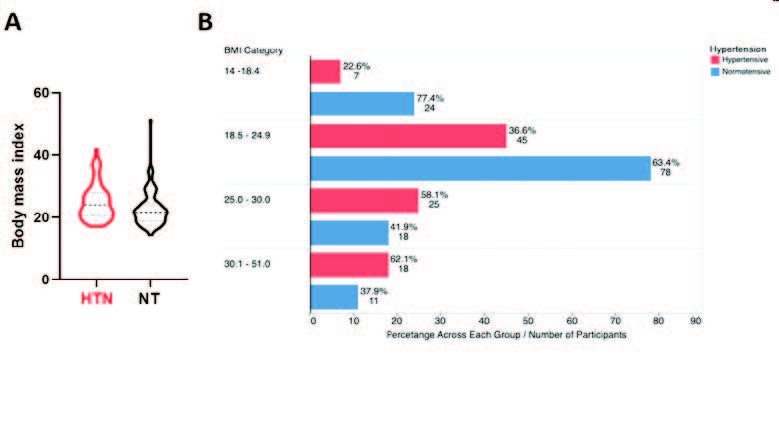
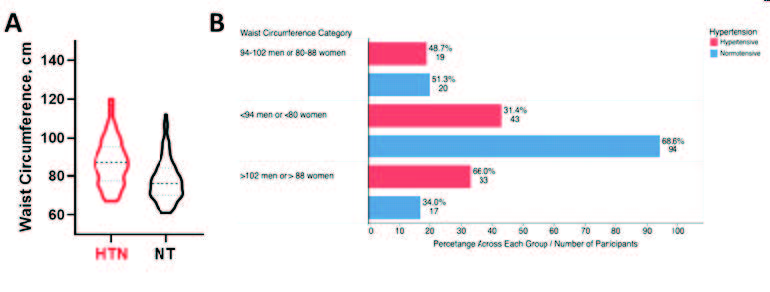
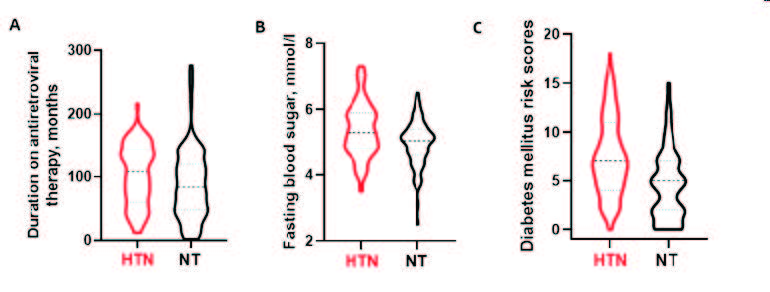
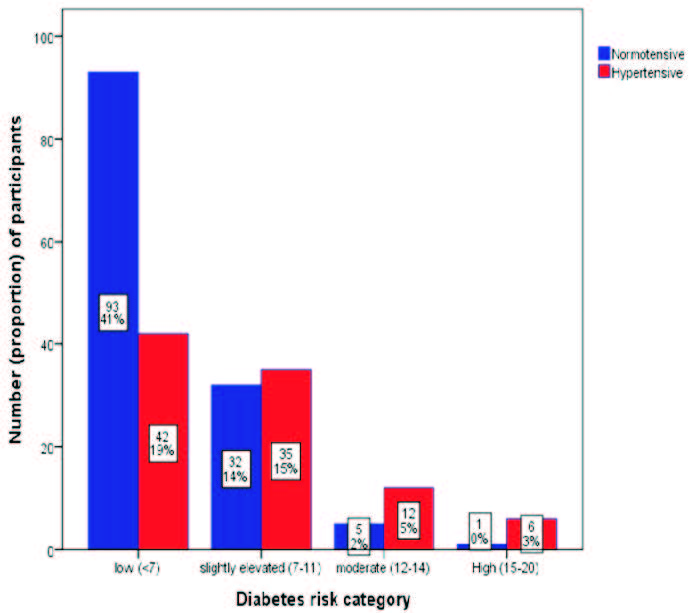
BMI (Fig 3A), BMI category (Fig 3B), WC (Fig 4A), WC category (Fig 4B), duration on ART (Fig 5A), fasting blood sugar (Fig 5B), diabetes risk scores (Fig SC), diabetes risk category (Fig 6), pulse pressure, mean arterial pressure, and mid-BP, were associated with hypertension, p<0.05 (Table 3). There was no specific ART regimen that was associated with hypertension. Pulse, CD4 count, and HIV RNA viral load were analogous between hypertensives and normotensive, p>0.05.
Fig 3. Distribution of body mass index between hypertensive and normotensive participants. Median body mass index (BMI) (panel A) and BMI categories (panel B) compared between hypertensive and normotensive participants
Fig 4. Distribution of waist circumference between hypertensive and normotensive participants. Median waist circumference (WC) (panel A) and WC categories (panel B) compared between hypertensive and normotensive participants
Fig 5. Duration on antiretroviral therapy, fasting blood sugar and diabetes risk scores between hypertensive and normotensive participants
Fig 6. Hypertension distribution by diabetes category
Multivariate analysis of factors associated with hypertension
We included all factors associated with hypertension in logistic regression in multivariate analysis. Age, BMI, employment status, table salt consumption (inversely association), and fasting blood sugar remained significantly associated with hypertension after adjustments, as shown in Table 4.
Comparison of the JNC 7 and AHA/ACC diagnostic criteria for hypertension
We compared the classification of the patients in our study using the JNC 7 and AHA criteria. We found that by using the new AHA/ ACC criteria, 26% more normotensive individuals (based on the JNC 7 criteria) were classified as hypertensive (Table 5).
While using the JNC 7 criteria puts the prevalence of hypertension in our study at 16%, the new AHA/ ACC criterion shifts the prevalence to 42% representing a 26% shift of those previously considered normotensive into the hypertensive category. The reported prevalence of hypertension in PLWH in low- and middle-income countries ranges from 4 to 54% 10 - 11. In ART-treated PLWH, a prevalence ofhypertension ofbetween 17 to 38% has been reported 12 - 15 using the JNC 7 criteria, lower than what we reported. However, with the new AHA/ ACC criteria, our results indicate an urgent need for intervention. However, further investigations are required to understand the outcomes of hypertension in PLWH when using the new hypertension guidelines as previous studies of cardiovascular events, stroke, etc. relied on different definitions of hypertension. So, we do not know whether the new guidelines will improve the prior epidemiological models.
Factors associated with hypertension in PLWH
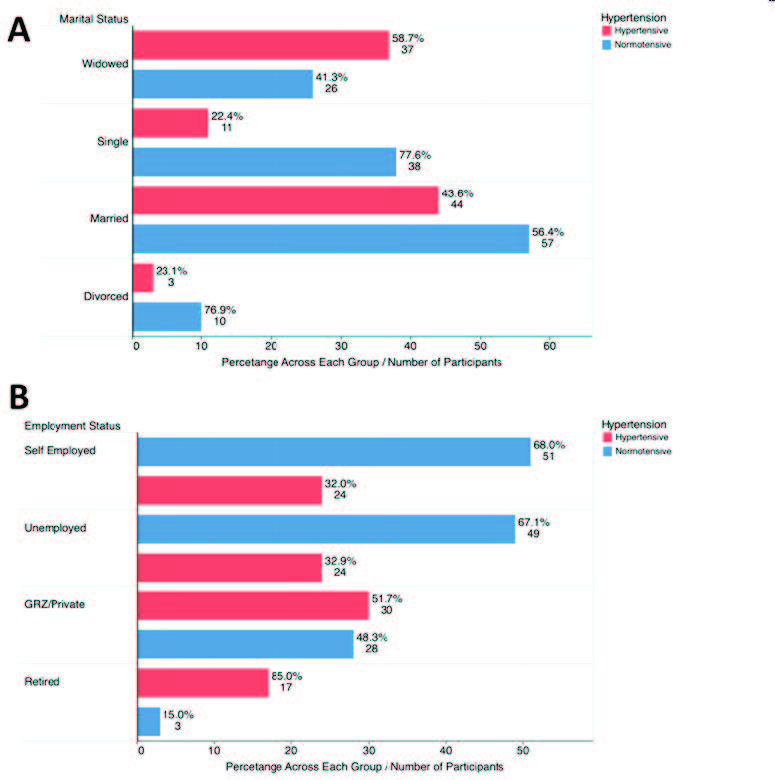
Among the social-demographic data collected, three were positively associated with hypertension, including the age of participants, employment status and marital status. In the Zambian setting, the patients' age is always recorded, while the rest are non-routine data. The new AHA/ ACC does not recommend consideration for employment status, marital status, or level of education when assessing risk for hypertension or treatment. However, most hypertensives in this study were married ( 46% hypertensive versus 43% normotensive), and in formal employment (31 % hypertensive versus 21 % normotensive). Furthermore, the JNC 7 and AHA/ACC does not consider the influence of these factors on blood pressure. Here, we suggest that further studies are needed to determine how an individual's employment status, marital status, and level of education are related to hypertension in low income countries.
Among dietary and lifestyle non-routinely collected variables, factors such as daily physical activity, the addition of salt at the table, and processed salt intake (negative association) were all positively associated with hypertension (Table 2), and this is in tandem with the recent hypertension report guidelines 4.
The clinical factors associated with hypertension included BMI, WC, and duration on ART, pulse pressure, MAP, mid-BP, FBS, diabetes risk scores, and risk category (Table 3). Among these, only BMI is routinely collected in Zambian hospitals. While BP components such as pulse pressure, MAP, and mid-BP are expected to be different between hypertensive and normotensive, we only included these variables in the analysis to indirectly assess the effect of antihypertensive drugs. It is expected that hypertensive patients taking antihypertensives will present with BP readings similar to r lower than those of normotensive individuals except when either the patient has hypertension that does not respond to the current treatment or dues to poor adherence to the hypertension medication. We found in our study that PP, MAP, and mid-BPs were higher in hypertensive patients. This is because all hypertensives in the study had not taken their medication for more than two weeks. Since we did not collect data on adherence to antihypertensive drugs and cannot ascertain the cause for this.
Hypertensive patients had high diabetes risk scores and FBS (Table 3). Often the factors associated with hypertension are likely related to diabetes risk too 16. Hence, we employed a diabetes risk assessment tool to assess if hypertensive patients were at risk of developing diabetes mellitus type 2 in 10 years. The value for diabetes risk assessment scores has been describing our recent previous study conducted in PLWH. Conducting diabetes risk assessment would be cardinal among PLWH9 let alone hypertensive.
We performed a multivariate logistic regression to assess each variable's contribution toward hypertension status (Table 4). Being older [1.0 (1.03, 1.15); AOR 95%CI] was positively associated with hypertension in HIV while those who were overweight (BMI =25-29.9) and obese (BMI equal to or greater than 30) were eight (p=0.043) and twenty-three (p=0.027) times more likely to be hypertensive, respectively. These findings are consistent with another study conducted locally in Zambia17 and other studies reviewed4. Fasting blood sugar was positively associated with hypertension (p=0.038) as those with higher fasting blood sugars were twice more likely to be hypertensive (1.0, 4.1, 95% CI). Being unemployed had reduced effect on hypertension [0.19 (0.04, 0.95); AOR 95% CI]. Unexpectedly, those who added salt onto the table had reduced odds [0.17 (0.04, 0.95; AOR, 95%)] for the development of hypertension compared to those who rarely or never add salt on the table. These results were contrary to a study conducted in neighbouring Zimbabwe, where adding salt to food at the table (AOR 2.77, 95% CI 1.41-5.43) was an independent risk factor for uncontrolled hypertension. However, the study population was not PLWH. In our study, we did not quantify the amount of salt the participants consumed. Hence, further studies are needed to ascertain the role of table salt as a risk factor for hypertension in PLWH. Several studies consistently report that higher salt intake is positively associated with BP and hypertension 18 - 20, albeit not in PLWH. A previous study reported that among the Zambian population, salt consumption was more than twice that recommended by WHO19. There is a general paucity of studies and no study known to us that has addressed salt intake and its relation to BP and hypertension in HIV. There is also the issue of salt sensitivity which varies among individuals21, 22. However, our study was beyond the scope of assessing actual salt quantities and sensitivity.
Compared to those with normal WC (<94 cm men; <88 cm women), individuals with a WC between 94- 102 for men and 80 to 88 for females and those with a WC above 102 for men and above 88 for females were sixteen times (1.2, 198.9; 95% CI) and 290 times respectively, more likely to be hypertensive (p<0.05). Individuals with more extended sedentary lifestyles, which is the amount of time spent seated, were more likely to be hypertensive [1.0 (1.00, 1.01); AOR, 95%CI, p=0.021] while minutes of moderate physical activity were associated with a lowerrisk of being hypertensive [0.98 (0.97, 1.00) 95%CI, p=0.048]. These results are consistent with previous studies and the AHA/ACC report on hypertension4• Our results provide evidence that several non-routinely collected variables should be incorporated into routine ART services and care to prevent hypertension and its attendant adverse outcomes.
Contextualizing the usage of new AHA/ACC guidelines in low-cost settings in PLWH
The treatment and care of PL WH previously overlooked the burden ofNCD comorbidity such as hypertension. Recently (2018), the Zambian Government, through the Ministry of Health integrated hypertension management in PLWH (see www.hivst.org). However, the guidelines are not detailed and lack the most critical hypertension diagnosis, treatment, and care emphasized in the new AHAi ACC criteria.
Using the new AHA/ACC criteria to diagnose hypertension shifted 26% of normotensives into hypertension (Table 5). This is consistent with the AHAi ACC report 4 . The advantage of this is that most the patients can prevent hypertension-related health complications through lifestyle changes alone, such as reducing salt intake, increasing physical activity, reducing sedentary time, and eating more plant based diets4, 23, 24. 4,23,24. These changes are feasible in low cost settings and can potentially reduce the burden and complications of hypertension.
The 10-year risk for heart disease and stroke using the atherosclerotic cardiovascular disease (ASCVD) risk calculator elaborated in the new AHA/ ACC guidelines is uncommon in Zambia and SSA countries. ASCVD risk components include age, sex, race, SBP, DBP, total cholesterol, high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, history of diabetes, smoking status, antihypertensive drug history, history of statin use, and aspirin use. Screening for ASCVD in low-cost settings is feasible, although testing for LDL and HDL is not yet routine at Livingstone Central Hospital.
Our study shows that the new AHA/ ACC guidelines are needed. We would, therefore, encourage integrating the guidelines into routine care for PLWH25 .
LIMITATIONS
We did not collect data on drug adherence to antihypertensive medications to ascertain the cause of uncontrolled BPs in hypertensive patients. Further, we did not have a comparison group (HIV negative) to ascertain the effect of HIV and ART on hypertension and factors related to hypertension.
CONCLUSION
The prevalence of hypertension in PLWH using the previous JNC 7 and new AHA/ACC criteria was 16% and 42%, respectively. A significant number of non-routinely collected variables ( employment status, dietary salt, fasting blood sugar, physical activity, sedentary hours) were associated with hypertension; hence, there is much need for intensifying monitoring and incorporating additional modifiable non-routine risk factors for hypertension in HIV care. The new AHA/ACC guidelines are indispensable and critical for care, hence the urgent need to integrate them in managing hypertension, especially among PLWH.
ABBREVIATIONS
3TC, Lamivudine; ABC, abacavir; ACC, American college of cardiology; AHA, American heart association; ACE, Angiotensin converting enzyme inhibitors; AOR, adjusted odds ratio; ART, antiretroviral therapy; ASCVD, atherosclerotic cardiovascular disease; AZT, azidothymidine, also called zidovudine; BMI, body mass index; BP, blood pressure; DBP, diastolic blood pressure; EFV, efavirenz ; FBS, fasting blood sugar; GRZ, government; HDL, high-density lipoprotein; HIV, human immunodeficiency virus; IDF, international diabetes federation; IPAQ, international physical activity questionnaire; IQR, interquartile range; JNC 7, Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; LCH, Livingstone Central Hospital; LDL, low-density lipoprotein; LPV /r, lopinavir/ritonavir ; MAP, mean arterial pressure; NCD, non-communicable disease; NVP, nevirapine ; OR, odds ratio; PLWH, persons with HIV; PP, pulse pressure; SBP, systolic blood pressure; TDF, tenofovir disoproxil fumarate ; WC, waist circumference; WHO STEPS, World health organization stepwise approach to surveillance; WHO, World Health Organizations;
DECLARATIONS
Ethics approval and consent to participate
Ethical approval was obtained from the University of Zambia Biomedical Research Ethics Committee (UNZABREC) (Assurance No. FWA00000338 IRB00001131 of IORG0000774) on 24th May 201 7. Permission to conduct the study was granted by the Livingstone Central Hospital Administration. All participants were asked to consent by signing a consent form before being included in the study. All data collected were de-identified and used for research purposes only.
What the study adds
The prevalence of hypertension in people living with HIV may be twice higher using AHA/ ACC guidelines
People living with HIV attending routine antiretroviral treatment clinics should be screened for risk factors associated with the development of hypertension. Such risk factors may include: dietary salt intake, fasting blood sugar, physical activity, and sedentary hours.
Consent for publication
Not applicable
Availability of data and materials
All data generated or analyzed during this study are included in this published article. For other data, these may be requested through the corresponding author.
Competing interests
The authors declare that they have no competing interests
Funding
This work is supported by the Fogarty International Center of the National Institutes of Health under the Award Number D43 TW009744
Author's contributions
SKM and SM conceived the study. SKM, BMH, MS, MM and SM contributed to the writing of the manuscript. SM is the principal investigator. SKM is the senior author and guarantor. All authors read, provided feedback, and approved the final manuscript.
Acknowledgements are very grateful to all Laboratory personnel and the Senior Medical Superintendent's office at Livingstone Central Hospital for their support and enthusiasm for research projects. We would also like to thank the LCH medical clinic nurses for their continued support and assistance during the data collection process.
TABLES:
Variables
Normotensive, n(%) 131 (58.0)
Hypertensive, 95 (42.0%)
Pvalue
Hypertension status based on old criteria
Normotensive, nltotal (%)
131 (100)
60 (63.2)
<0.001
191/226 (85.5%)
Hypertensive, nltotal (%)
0 (0.0)
35 (36.8)
35/226 (15.5%)
Age,median years (/QR)
40 (30, 46)
50 (42, 57)
<0.001
Age category (years)
18-35
49 (37.4)
8(8.4)
<0.001
36-45
45 (34.4)
28 (29.5)
30 (22.9)
30 (31.6)
56-65
6 (4.6)
25 (26.3)
66-90
1 (0.8)
4 (4.2)
Gender, n (%)
Female
89 (67.9)
60 (63.2)
0.454
Male
42 (32.1)
35 (36.8)
Marital status
Married
57 (43.5)
44 (46.3)
0.001
Widowed
26 (19.8)
37 (38.9)
Single
38 (29.0)
11 (11.6)
Divorced
10 (7.6)
3 (3.2)
Employment Status
GRZ/Private
28 (21.4)
30 (31.6)
<0.001
Self employed
51 (38.9)
24 (25.3)
Retired
3 (2.3)
17 (17.9)
Unemployed
49 (37.4)
24 (25.3)
Highest Education attained
No formal education
5 (3.8)
4 (4.2)
0.339
Primary
28 (21.4)
20 (21.1)
Secondary
76 (58.0)
46 (48.4)
Tertiary
22 (16.8)
25 (26.3)
IQR, interquartile range; GRZ, government; n, number of participants;
%, percentage
Variables
Normotensive n(%) 131 (58.0)
Hypertensive n (%), 95 (42.0%)
P Value
Daily physical activity
Yes
69 (52.7)
35 (36.8)
0.018
No
62 (47.3)
60 (63.2)
Minutes of Weekly vigor ous activity, median (/QR)
AHA, American heart association; ACC, American college of cardiology; BP, blood pressure; JNC 7, Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure
REFERENCES
Bloomfield GS, Hogan JW, Keter A, Sang E, Carter EJ, Velazquez EJ et al. Hypertension and obesity as cardiovascular risk factors among HIV seropositive patients in Western Kenya. PLoSONE2011; 6: e22288.
Maher D, Waswa L, Baisley K, Karabarinde A, UnwinN. Epidemiology ofhypertension in lowincome countries: a cross-sectional populationbased survey in rural Uganda. J Hypertens 2011; 29: 1061-1068.
Mateen FJ, Kanters S, Kalyesubula R, Mukasa B, Kawuma E, Kengne AP et al. Hypertension prevalence and Framingham risk score stratification in a large HIV-positive cohort in Uganda. J Hypertens 2013; 31: 1372-1378; discussion 1378.
Whelton PK, Carey RM, Aronow WS, Casey DE, Collins KJ, Dennison Himmelfarb C et al. 2017 ACC/AHA/AAPA/ABC/ACPM/ AGS/APhA/A SH/A SPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/ American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2017. doi:10.1161/ HYP. 0000000000000066.
ChobanianAV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 2003; 289: 2560-2572.
Clark SJ, Gomez-O live FX, Houle B, Thorogood M, Klipstein-Grobusch K, Angotti N et al. Cardiometabolic disease risk and HIV status in rural South Africa: establishing a baseline. BMC Public Health 2015; 15. doi: 10.1186/sl2889-015-1467-1.
Kavishe B, Biraro S, Baisley K, Vanobberghen F, Kapiga S, Munderi P et al. High prevalence of hypertension and of risk factors for noncommunicable diseases (NCDs): a populationbased cross-sectional survey of NCDS and HIV infection in Northwestern Tanzania and Southern Uganda. BMC Med 2015; 13. doi: 10.1186/s12916-015-0357-9.
Edwards JK, Bygrave H, Van den Bergh R, Kizito W, Cheti E, Kosgei RJ et al. HIV with non-communicable diseases in primary care in Kibera, Nairobi, Kenya: characteristics and outcomes 2010-2013. Trans R Soc Trop Med Hyg 2015; 109:440-446.
Masenga SK, Toloka P, Chiyenu K, Imasiku I,
Mutengo H, Ulungu ON et al. Type 2 diabetes mellitus prevalence and risk scores in treated PLWHIV: a cross-sectional preliminary study. BMCResearchNotes2019; 12: 145.
Martin-Iguacel R, Negredo E, Peck R, Friis-M0ller N. Hypertension Is a Key Feature of the Metabolic Syndrome in Subjects Aging with HIV. Curr Hypertens Rep 2016; 18: 46.
Nguyen KA, Peer N, Mills EJ, Kengne AP. Burden, Determinants, and Pharmacological Management of Hypertension in HIV-Positive Patients and Populations: A Systematic Narrative Review.AIDSRev2015; 17: 83-95.
Peck RN, Shedafa R, Kalluvya S, Downs JA, Todd J, Suthanthiran M et al. Hypertension, kidney disease, HIV and antiretroviral therapy among Tanzanian adults: a cross-sectional study.BMCMed2014; 12. doi:10.1186/s12916-014-0125-2.
Muhammad S, Sani MU, Okeahialam BN. Cardiovascular disease risk factors among HIV-infected Nigerians receiving highly active antiretroviral therapy. Niger Med J 2013; 54:
185-190.
Kagaruki GB, Mayige MT, Ngadaya ES, Kimaro GD, Kalinga AK, Kilale AM et al. Magnitude and risk factors of non-communicable diseases among people living with HIV in Tanzania: a cross sectional study from Mbeya and Dar es Salaam regions. BMC Public Health 2014; 14: 904.
Dimala CA, Atashili J, Mbuagbaw JC, Wilfred A, Monekosso GL. Prevalence of Hypertension in HIV/ AIDS Patients on Highly Active Antiretroviral Therapy (HAART) Compared with HAART-Nai:ve Patients at the Limbe Regional Hospital, Cameroon. PLoS ONE 2016; 11: e0148100.
Cheung BMY, Li C. Diabetes and Hypertension: Is There a Common Metabolic Pathway? Curr AtherosclerRep2012; 14: 160-166.
Rush KL, Goma FM, Barker JA, Ollivier RA, Ferrier MS, Singini D. Hypertension prevalence and risk factors in rural and urban Zambian adults in western province: a cross-sectional study. Pan Afr Med J 2018; 30. doi:10.11604/pamj.2018.30.97.14717.
Ware LJ, Charlton K, Schutte AE, Cockeran M, Naidoo N, Kowal P. Associations between dietary salt, potassium and blood pressure in South African adults: WHO SAGE Wave 2 Salt & Tobacco. Nutr Metab Cardiovasc Dis 2017; 27: 784-791.
Oelke ND, Rush KL, Goma FM, Barker J, Marek P, Pedersen C. Understanding Perceptions and Practices for ZambianAdults in Western Province at Risk for Hypertension: An Exploratory Descriptive Study. Glob J Health Sci2016;8: 248-259.
Azinge EC, Sofola OA, Silva BO. Relationship between salt intake, salt-taste threshold and blood pressure in Nigerians. West Afr J Med 2011; 30: 373-376.
Kirabo A. A new paradigm of sodium regulation in inflammation and hypertension. Am J Physiol Regul Integr Comp Physiol 2017; 313: R706-R710.
Choi HY, Park HC, Ha SK. Salt Sensitivity and Hypertension: A Paradigm Shift from Kidney Malfunction to Vascular Endothelial Dysfunction. Electrolyte Blood Press 2015; 13:
7-16.
He FJ, MacGregor GA. Reducing population salt intake worldwide: from evidence to implementation. Prog Cardiovasc Dis 201O; 52: 363-382.
He FJ, Li J, MacGregor GA. Effect of longer-term modest salt reduction on blood pressure: Cochrane systematic review and meta-analysis ofrandomised trials. BMJ2013; 346: f1325.
Munsaka, S. M., Hamooya, B. M., Malumani, M., Chiluba, B. C., & Masenga, S. K. (2022). Blood Pressure Monitoring Variation in Routine Antiretroviral Therapy Clinic Visits: A Cross-Sectional study. Journal of Preventive and Rehabilitative Medicine, 4(1 ), 53-58.